Case Review #13: 50 year old female with progressive Adult Idiopathic Scoliosis
•
1 gefällt mir•624 views

A 50 year old female presented with a progressive 58° thoracic curve, and 60° lumbar curve. No previous surgeries. KIM/SRP Classification 3

Empfohlen
Empfohlen
Weitere ähnliche Inhalte
Was ist angesagt?
Was ist angesagt? (20)
Ähnlich wie Case Review #13: 50 year old female with progressive Adult Idiopathic Scoliosis
Ähnlich wie Case Review #13: 50 year old female with progressive Adult Idiopathic Scoliosis (20)
Mehr von Robert Pashman
Mehr von Robert Pashman (15)
Kürzlich hochgeladen
Kürzlich hochgeladen (20)
Case Review #13: 50 year old female with progressive Adult Idiopathic Scoliosis
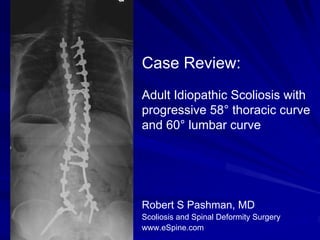
- 1. Case Review: Adult Idiopathic Scoliosis with progressive 58° thoracic curve and 60° lumbar curve Robert S Pashman, MD Scoliosis and Spinal Deformity Surgery www.eSpine.com
- 2. Patient History 50-year-old female, diagnosed with Adult Idiopathic Scoliosis, no previous surgeries. No non idiopathic history such as neuromuscular problems or structural abnormalities including congenital abnormalities of her spine. The patient is otherwise in good health, having quit smoking approximately 8 years ago. The scoliosis and progressive deformity are associated with significant pain that related to her right flank where the curve is of its largest magnitude, and the patient is also having neck, thoracic and low back pain, and radiculopathy, which is currently being managed by escalating amounts of narcotics. Her shoulders are level. She has a right rib hump, left flank fullness associated with a significant flank crease on concave right side. Pelvis seems to be level. Leg lengths are equal and neurologically she is intact. She is well-balanced in the frontal and sagittal planes and looks otherwise healthy www.eSpine.com
- 3. Pre-op X-rays The patient has a 58° upper thoracic, 60° lumbar curve with significant rotation. She has significant fractional 58° lumbosacral obliquity but otherwise is well-balanced in the frontal and sagittal plane. The patient's symptoms will definitely be progressive over 60° the long term. We know that statistically because adults with curves greater than 50° progress at approximately 1° per year. www.eSpine.com
- 4. Indications for Surgery Adult progressive idiopathic scoliosis, 60° lumbar progression with compensatory thoracic curve. Lumbosacral anomaly with significant lumbosacral obliquity. Stenosis of foramen with low back pain. Failed conservative therapy. Low back pain and radicular symptoms. www.eSpine.com
- 5. Surgical Strategy Posterior spinal instrumented fusion using Alphatec pedicle screw rod construct from T3 to sacral pelvis, 5.5 stainless steel. Spinal osteotomy Smith-Petersen and a Ponte osteotomy, T5-6, T6- 7, T7-8, T8-9, T9-10, T10-11, T12-L1, L1-2, L3-4, L4-5, L5-S1, 11- level, for mobilization of rigid spinal deformity. Interlaminar decompression for concave stenosis L2-3, L3-4, L4-5, L5-S1 under loupe and headlight magnification. Interlaminar laminotomies with facetectomy lateral recess release on the left-hand side at L3-4, L4-5, L5-S1. Posterior spinal fusion with locally harvested autogenous bone and rhBMP T3 to sacral pelvis. Motor evoked potentials. Intraoperative fluoroscopy. www.eSpine.com
- 6. Post-Op Films The patient is balanced in both the frontal and 28° sagittal planes. 30° www.eSpine.com
- 7. Pre-Op/Post-op Comparison The patient’s curvature was reduced by 50%, from 60° to 30°. She 28° gained several inches in 58° height, and was very happy with the outcome 60° of her surgery. 30° www.eSpine.com
- 8. Pre-Op/Post-op Comparison The patient is balanced in the sagittal plane, and no longer has symptoms in her legs. www.eSpine.com