Minarcik robbins 2013_ch7-neoplasm
•Als PPT, PDF herunterladen•
21 gefällt mir•2,699 views


Empfohlen
Weitere ähnliche Inhalte
Was ist angesagt?
Was ist angesagt? (20)
Andere mochten auch
Andere mochten auch (11)
Ähnlich wie Minarcik robbins 2013_ch7-neoplasm
Ähnlich wie Minarcik robbins 2013_ch7-neoplasm (20)
Mehr von Elsa von Licy
Mehr von Elsa von Licy (20)
Kürzlich hochgeladen
Kürzlich hochgeladen (20)
Minarcik robbins 2013_ch7-neoplasm
- 1. Neoplasia
- 2. NEOPLASIA (TUMORS) Definitions Nomenclature Biology of Tumor Growth Epidemiology Molecular Basis of Cancer Molecular Basis of Carcinogenesis Agents (The Usual Suspects) Host Defense (Tumor Immunity) Clinical Features of Tumors
- 3. Defnition of Neoplasia “A neoplasm is an abnormal mass of tissue, the growth of which exceeds and is uncoordinated with that of the normal tissues and persists in the same excessive manner after cessation of the stimuli which evoked the change” - Willis Genetic changes Autonomous Clonal
- 4. Nomenclature – Benign Tumors -oma = benign neoplasm (NOT carcin-, sarc-, lymph-, or melan-) Mesenchymal tumors (mesodermal derived) chrondroma: cartilaginous tumor fibroma: fibrous tumor osteoma: bone tumor Epithelial tumor (ecto- or endo- derived) adenoma: tumor forming glands papilloma: tumor with finger like projections papillary cystadenoma: papillary and cystic tumor forming glands polyp: a “tumor” that projects above a mucosal surface
- 6. Downloaded from: Robbins & Cotran Pathologic Basis of Disease (on 28 July 2005 03:41 PM) © 2005 Elsevier
- 7. Tumor Stalk Colonic Polyp: Tubular Adenoma
- 8. Nomenclature – Malignant Tumors Sarcomas: mesenchymal tumor chrondrosarcoma: cartilaginous tumor fibrosarcoma: fibrous tumor osteosarcoma: bone tumor Carcinomas: epithelial tumors adenocarcinoma: gland forming tumor squamous cell carcinoma: squamous differentiation undifferentiated carcinoma: no differentiation note: carcinomas can arise from ectoderm, endoderm, or less likely, mesoderm
- 14. Tumors with mixed differentiation Teratoma tumor comprised of cells from more than one germ layer arise from totipotent cells (usually gonads) benign cystic teratoma of ovary is the most common teratoma Aberrant differentiation (not true neoplasms) mixed tumors: e.g. pleomorphic adenoma of salivary gland carcinosarcoma Hamartoma: disorganized mass of tissue whose cell types are indiginous to the site of the lesion, e.g., lung Choriostoma: ectopic focus of normal tissue (heterotopia), e.g., pancreas, perhaps endometriosis too Misnomers hepatoma: malignant liver tumor melanoma: malignant skin tumor seminoma: malignant testicular tumor lymphoma: malignant tumor of lymphocytes
- 15. Downloaded from: Robbins & Cotran Pathologic Basis of Disease (on 28 July 2005 03:41 PM) © 2005 Elsevier
- 18. Natural History Of Malignant Tumors 1. 2. Malignant change in the target cell, referred to as transformation Growth of the transformed cells 3. Local invasion 4. Distant metastases.
- 19. Differentiation Well differentiated neoplasm Poorly differentiated neoplasm Resembles mature cells of tissue of origin Composed of primitive cells with little differentiation Undifferentiated or “anaplastic” tumor Correlation with biologic behavior Benign tumors are well differentiated Poorly differentiated malignant tumors usually have worse prognosis than well differentiated malignant tumors.
- 20. If cells LOOK BAD, they are probably going to BEHAVE BAD Looking “bad” means NOT looking like the cells they supposedly arose from!
- 21. If cells LOOK GOOD, they are probably going to BEHAVE GOOD Looking “good” means looking like the cells they supposedly arose from!
- 23. “ANAPLASIA” = CANCER ***Pleomorphism Size shape Abnormal nuclear morphology ***Hyperchromasia High nuclear cytoplasmic ratio Chromatin clumping Prominent nucleoli Mitoses Mitotic rate Location of mitoses Loss of polarity
- 25. Dysplasia Literally means abnormal growth Malignant transformation is a multistep process In dysplasia some but not all of the features of malignancy are present, microscopically Dysplasia may develop into malignancy Uterine cervix Colon polyps Graded as low-grade or high-grade, often prompting different clinical decisions Dysplasia may NOT develop into malignancy HIGH grade dysplasia often classified with CIS
- 28. Tumor Growth Rate Doubling time of tumor cells Lengthens as tumor grows 30 doublings (109 cells) = 1 g (months to years) 10 more doublings (1 kg) = lethal burden (“) Fraction of tumor cells in replicative pool May be only 20% even in rapidly growing tumors Tumor stem cells Rate at which tumor cells are shed or lost Apoptosis Maturation Implications for therapy
- 29. “clonal”
- 30. Schematic Representation Of Tumor Growth
- 31. Features of Malignant Tumors Cellular features Local invasion Capsule Basement membrane Metastasis Unequivocal sign of malignancy Seeding of body cavities Lymphatic Hematogenous
- 39. Significance of Nodal Mets Example of breast cancer Halsted radical mastectomy Sentinel node biopsy Prognostic Number of involved nodes is an important component of TNM staging system Therapeutic Overall risk of recurrence Extent of nodal involvement Histologic grade and other considerations “Adjuvant” chemotherapy
- 40. Benign vs Malignant Features Feature Benign Malignant Rate of growth Progressive but slow. Mitoses few and normal Variable. Mitoses more frequent and may be abnormal Differentiation Well differentiated Some degree of anaplasia LOCAL INVASIO N Cohesive growth. Poorly cohesive Capsule & BM and not breached infiltrative! Metastasis Absent infiltrative! May occur
- 46. Geographic & Environmental Sun exposure Smoking and alcohol abuse Body mass Overweight = 50% increase in cancer Environmental vs. racial factors Melanomas 6x incidence New Zealand vs. Iceland Blacks have low incidence of melanoma, so do normally pigmented areas like areolae on white people Japanese immigrants to USA Viral exposure Human papilloma virus (HPV) and cervical cancer Hepatitis B virus (HBV) and liver cancer (Africa, Asia) Epstein-Barr Virus (EBV) and lymphoma
- 47. Change In Incidence Of Various Cancers With Migration From Japan To The United States
- 48. Age Predisposing Factors for Cancer Most cancers occur in persons ≥ 55 years Childhood cancers Genetic predispostion Familial cancer syndromes Leukemias & CNS neoplasms Bone tumors Early age at onset Two or more primary relatives with the cancer (“soil” theory) Multiple or bilateral tumors Polymorphisms that metabolize procarcinogens, e.g., nitrites Nonhereditary predisposing conditions Chronic inflammation? Precancerous conditions Chronic ulcerative colitis Atrophic gastritis of pernicious anemia Leukoplakia of mucous membranes Immune collapse?
- 49. Defnition of Neoplasia “A neoplasm is an abnormal mass of tissue, the growth of which exceeds and is uncoordinated with that of the normal tissues and persists in the same excessive manner after cessation of the stimuli which evoked the change” - Willis Genetic changes Autonomous Clonal
- 50. MOLECULAR BASIS of CANCER NON-lethal genetic damage A tumor is formed by the clonal expansion of a single precursor cell (monoclonal) Four classes of normal regulatory genes PROTO-oncogenes Oncogenes Oncoproteins DNA repair genes Apoptosis genes Carcinogenesis is a multistep process
- 51. TRANSFORMATION & PROGRESSION Self-sufficiency in growth signals Insensitivity to growth-inhibiting signals Evasion of apoptosis Defects in DNA repair: “Spell checker” Limitless replicative potential: Telomerase Angiogenesis Invasive ability Metastatic ability
- 53. Normal CELL CYCLE Phases INHIBITORS: Cip/Kip, INK4/ARF Tumor (really growth) suppressor genes: p53
- 54. ONCOGENES Are MUTATIONS of NORMAL genes (PROTO-oncogenes) Growth Factors Growth Factor Receptors Signal Transduction Proteins (RAS) Nuclear Regulatory Proteins Cell Cycle Regulators Oncogenes code for Oncoproteins
- 55. Category PROTOOncogene Mode of Activation Associated Human Tumor GFs PDGF-β chain SIS Fibroblast HST-1 growth factors INT-2 TGFα HGF Overexpression Astrocytoma Osteosarcoma Overexpression Stomach cancer Amplification Bladder cancer TGFα Breast cancer Melanoma Overexpression Astrocytomas HGF Hepatocellular carcinomas Overexpression Thyroid cancer
- 56. Category PROTOOncogene Mode of Activation Associated Human Tumor GF Receptors EGF-receptor family ERB-B1 (ECFR) Overexpression Squamous cell carcinomas of lung, gliomas ERB-B2 Amplification Breast and ovarian cancers CSF-1 receptor FMS Point mutation Leukemia Receptor for neurotrophic factors RET Point mutation Multiple endocrine neoplasia 2A and B, familial medullary thyroid carcinomas PDGF receptor PDGF-R Overexpression Gliomas Point mutation Gastrointestinal stromal tumors and other soft tissue tumors Receptor for stem KIT cell (steel) factor
- 57. Category PROTOOncogene Mode of Activation Associated Human Tumor Signal Transduction Proteins GTP-binding Point mutation Colon, lung, and pancreatic tumors H-RAS Point mutation Bladder and kidney tumors N-RAS Nonreceptor tyrosine kinase K-RAS Point mutation Melanomas, hematologic malignancies ABL Translocation Chronic myeloid leukemia Acute lymphoblastic leukemia RAS signal transduction BRAF Point mutation Melanomas WNT signal transduction β-catenin Point mutation Hepatoblastomas, hepatocellular carcinoma
- 58. Category Nuclear Regulatory Proteins PROTOOncogene Mode of Activation Associated Human Tumor Transcrip. C-MYC activators Translocation Burkitt lymphoma N-MYC Amplification Neuroblastoma, small cell carcinoma of lung L-MYC Amplification Small cell carcinoma of lung
- 59. MYC Encodes for transcription factors Also involved with apoptosis
- 60. P53 and RAS p53 Activates DNA repair proteins Sentinel of G1/S transition Initiates apoptosis Mutated in more than 50% of all human cancers RAS H, N, K, etc., varieties Single most common abnormality of dominant oncogenes in human tumors Present in about 1/3 of all human cancers
- 62. Tumor (really “GROWTH”) suppressor genes TGF-β COLON E-cadherin STOMACH NF-1,2 NEURAL TUMORS APC/β-cadherin GI, MELANOMA SMADs GI RB RETINOBLASTOMA P53 EVERYTHING!! WT-1 WILMS TUMOR p16 (INK4a) GI, BREAST (MM if inherited) BRCA-1,2 BREAST KLF6 PROSTATE
- 64. DNA REPAIR GENE DEFECTS DNA repair is like a spell checker HNPCC (Hereditary Non-Polyposis Colon Cancer [Lynch]): TGF-β, β-catenin, BAX Xeroderma Pigmentosum: UV fixing gene Ataxia Telangiectasia: ATM gene Bloom Syndrome: defective helicase Fanconi anemia
- 65. LIMITLESS REPLICATIVE POTENTIAL TELOMERES determine the limited number of duplications a cell will have, like a cat with nine lives. TELOMERASE, present in >90% of human cancers, changes telomeres so they will have UNLIMITED replicative potential
- 66. TUMOR ANGIOGENESIS Q: How close to a blood vessel must a cell be? A: 1-2 mm Activation of VEGF and FGF-b Tumor size is regulated (allowed) by angiogenesis/anti-angiogenesis balance
- 68. Invasion Factors Detachment ("loosening up") of the tumor cells from each other Attachment to matrix components Degradation of ECM, e.g., collagenase, etc. Migration of tumor cells
- 70. METASTATIC GENES? NM23 KAI-1 KiSS
- 71. CHROMOSOME CHANGES in CANCER TRANSLOCATIONS and INVERSIONS Occur in MOST Lymphomas/Leukemias Occur in MANY (and growing numbers) of NON-hematologic malignancies also
- 72. Malignancy Translocation Affected Genes Chronic myeloid leukemia (9;22)(q34;q11) Ab1 9q34 bcr 22q11 Acute leukemias (AML and ALL) (4;11)(q21;q23) AF4 4q21 MLL 11q23 (6;11)(q27;q23) AF6 6q27 MLL 11q23 Burkitt lymphoma (8;14)(q24;q32) c-myc 8q24 IgH 14q32 Mantle cell lymphoma (11;14)(q13;q32) Cyclin D 11q13 IgH 14q32 Follicular lymphoma (14;18)(q32;q21) IgH 14q32 bcl-2 18q21 T-cell acute lymphoblastic leukemia (8;14)(q24;q11) c-myc 8q24 TCR-α 14q11 (10;14)(q24;q11) Hox 11 10q24 TCR-α 14q11 Ewing sarcoma (11;22)(q24;q12) Fl-1 11q24
- 73. Carcinogenesis is “MULTISTEP” NO single oncogene causes cancer BOTH several oncogenes AND several tumor suppressor genes must be involved Gatekeeper/Caretaker concept Gatekeepers: ONCOGENES and TUMOR SUPPRESSOR GENES Caretakers: DNA REPAIR GENES Tumor “PROGRESSION” ANGIOGENESIS HETEROGENEITY from original single cell
- 74. Carcinogenesis: The USUAL (3) Suspects Initiation/Promotion concept: BOTH initiators AND promotors are needed NEITHER can cause cancer by itself INITIATORS (carcinogens) cause MUTATIONS PROMOTORS are NOT carcinogenic by themselves, and MUST take effect AFTER initiation, NOT before PROMOTORS enhance the proliferation of initiated cells
- 76. Q: WHO are the usual suspects? Inflammation? Teratogenesis? Immune Suppression? Neoplasia? Mutations?
- 77. A: The SAME 3 that are ALWAYS blamed! 1) Chemicals 2) Radiation 3) Infectious Pathogens
- 78. CHEMICAL CARCINOGENS: INITIATORS “PRO”CARCINOGENS DIRECT β-Propiolactone Dimeth. sulfate Diepoxybutane Anticancer drugs (cyclophosphamide, chlorambucil, nitrosoureas, and others) Acylating Agents 1-Acetyl-imidazole Dimethylcarbamyl chloride Polycyclic and Heterocyclic Aromatic Hydrocarbons Aromatic Amines, Amides, Azo Dyes Natural Plant and Microbial Products Aflatoxin B1 Hepatomas Griseofulvin Antifungal Cycasin from cycads Safrole from sassafras Betel nuts Oral SCC
- 79. CHEMICAL CARCINOGENS: INITIATORS OTHERS Nitrosamine and amides (tar, nitrites) Vinyl chloride angiosarcoma in Kentucky Nickel Chromium Insecticides Fungicides PolyChlorinated Biphenyls (PCBs)
- 80. CHEMICAL CARCINOGENS: PROMOTORS HORMONES PHORBOL ESTERS (TPA), activate kinase C PHENOLS DRUGS, many “Initiated” cells respond and proliferate FASTER to promotors than normal cells
- 81. RADIATION CARCINOGENS UV: BCC, SCC, MM (i.e., all 3) IONIZING: photons and particulate Hematopoetic and Thyroid (90%/15yrs) tumors in fallout victims Solid tumors either less susceptible or require a longer latency period than LEUK/LYMPH BCCs in Therapeutic Radiation
- 82. VIRAL CARCINOGENESIS HPV SCC EBV Burkitt Lymphoma HBV HepatoCellular Carcinoma (Hepatoma) HTLV1 T-Cell Malignancies KSHV Kaposi Sarcoma
- 83. H. pylori CARCINOGENESIS 100% of gastric lymphomas (i.e., M.A.L.T.omas) Gastric CARCINOMAS also!
- 84. HOST DEFENSES IMMUNE SURVEILLENCE CONCEPT CD8+ T-Cells NK cells MACROPHAGES ANTIBODIES
- 85. CYTOTOXIC CD8+ T-CELLS are the main eliminators of tumor cells
- 86. How do tumor cells escape immune surveillance? Mutation, like microbes ↓ MHC molecules on tumor cell surface Lack of CO-stimulation molecules, e.g., (CD28, ICOS), not just Ag-Ab recognition Immunosuppressive agents Antigen masking Apoptosis of cytotoxic T-Cells (CD8), i.e., the damn tumor cell KILLS the T-cell!
- 87. Effects of TUMOR on the HOST Location anatomic ENCROACHMENT HORMONE production Bleeding, Infection ACUTE symptoms, e.g., rupture, infarction METASTASES
- 88. CACHEXIA Reduced diet: Fat loss>Muscle loss Cachexia: Fat loss AND Muscle loss TNF (α by default) IL-(6) PIF (Proteolysis Inducing Factor)
- 89. PARA-Neoplastic Syndromes Endocrine (next) Nerve/Muscle, e.g., myasthenia w. lung ca. Skin: e.g., acanthosis nigricans, dermatomyositis Bone/Joint/Soft tissue: HPOA (Hypertrophic Pulmonary OsteoArthropathy) Vascular: Trousseau, Endocarditis Hematologic: Anemias
- 90. ENDOCRINE Cushing syndrome Small cell carcinoma of lung ACTH or ACTH-like substance Pancreatic carcinoma Neural tumors Syndrome of inappropriate antidiuretic hormone secretion Small cell carcinoma of lung; intracranial neoplasms Antidiuretic hormone or atrial natriuretic hormones Hypercalcemia Squamous cell carcinoma of lung Parathyroid hormone-related protein (PTHRP), TGF-α, TNF, IL-1 Breast carcinoma Renal carcinoma Adult T-cell leukemia/lymphoma Ovarian carcinoma Hypoglycemia Fibrosarcoma Insulin or insulin-like substance Other mesenchymal sarcomas Hepatocellular carcinoma Carcinoid syndrome Bronchial adenoma (carcinoid) Serotonin, bradykinin Pancreatic carcinoma Gastric carcinoma Polycythemia Renal carcinoma Erythropoietin Cerebellar hemangioma Hepatocellular carcinoma
- 91. GRADING/STAGING GRADING: HOW “DIFFERENTIATED” ARE THE CELLS? STAGING: HOW MUCH ANATOMIC EXTENSION? TNM Which one of the above do you think is more important?
- 92. WELL? (pearls) MODERATE? (intercellular bridges) POOR? (WTF!?!) GRADING for Squamous Cell Carcinoma
- 93. ADENOCARCINOMA GRADING Let’s have some FUN!
- 94. LAB DIAGNOSIS BIOPSY CYTOLOGY: (exfoliative) CYTOLOGY: (FNA, Fine Needle Aspirate)
- 95. IMMUNOHISTOCHEMISTRY Categorization of undifferentiated tumors Leukemias/Lymphomas Site of origin Receptors, e.g., ERA, PRA
- 96. TUMOR MARKERS HORMONES: (Paraneoplastic Syndromes) “ONCO”FETAL: AFP, CEA ISOENZYMES: PAP, NSE PROTEINS: PSA, PSMA (“M” = “membrane”) GLYCOPROTEINS: CA-125, CA-195, CA-153 MOLECULAR: p53, RAS NOTE: These SAME substances which can be measured in the blood, also can be stained by immunochemical methods in tissue
- 97. MICRO-ARRAYS THOUSANDS of genes identified from tumors give the cells their own identity and FINGERPRINT and may give important prognostic information as well as guidelines for therapy. Some say this may replace standard histopathologic identifications of tumors. What do you think?
Hinweis der Redaktion
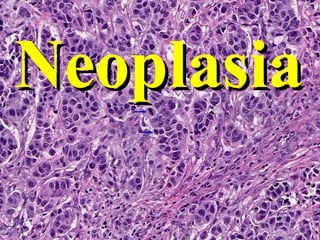
- Poorly differentiated carcinoma of breast. Best tumor pics are from the Iowa virtual microscope! Iowa Histopathology
- Outline of topics!
- Papillary adenoma of colon. Note the fingerlike projections of the tumor. Iowa Histopathology
- Figure 7-2 Colonic polyp.. Gross appearance of several colonic polyps. Also called adenomas. Sometimes called tubular adenomas, sometimes adenomatous polyp, sometimes “villous” adenoma.
- Colonic polyp. This benign glandular tumor (adenoma) is projecting into the colonic lumen and is attached to the mucosa by a distinct stalk.
- This view shows the transition from normal squamous epithelium into invasive carcinoma. Can you tell by the appearance that the SCC “arose” from the squamous epithelium?
- A hallmark of well differentiated squamous cell carcinoma is that the nests of invading cells still attempt to make keratin which then gets deposited in the center of the nests, resulting in a keratin "pearl". A “pearl” in a squamous cell carcinoma qualifies it to be “well” differentiated. From the Iowa Collection
- Another characteristic of a well differentiated squamous cell carcinoma is that it still makes visible intercellular bridges. Squamous cell carcinomas in which intercellular bridges (i.e., desmosomes, or tonofibrils) can be identified, but NOT pearls are often called “moderately” differentiated.
- Adenocarcinoma of colon arising in a case of ulcerative colitis. Do you think that most adenocarcinomas arise from tissues or organs that are “glandular” themselves? Ans : YES!
- Lymph node with undifferentiated large cell carcinoma of the lung. If these epithelial tumor cells formed little circular or tubular structures called “glands”, it might better be termed “adenocarcinoma”. If it showed any attempt at keratin formation, “pearls”, or intercellular bridges between tumor cells, it might best be termed “squamous cell” carcinoma. From the Iowa collection
- Misnomers are often REDUNDANT, to try to correct the misnomer.
- Figure 7-4 A, Gross appearance of an opened cystic teratoma of the ovary. Note the presence of hair, sebaceous material, and tooth. You do not need a microscope to appreciate this tumor produces both connective tissue as well as epithelial derived elements. Remember, pure “epithelial” tumors may evoke a fibrous response, such as breast or pancreas or prostate adenocarcinomas, but the connective tissue us regarded as NON-neoplastic.
- A microscopic view of a similar tumor shows sebaceous glands, respiratory epithelium, bone, and bone marrow. Don’t mistake this for a “fibrous reaction” to an epithelial tumor.
- Dermoid cyst of ovary (a component of benign cystic teratoma) Iowa Collection
- Another linear process, such as the epics of inflammation or healing.
- Can “undifferentiated” also be called very very very very very poorly differentiated? ANS: YES Why might a “well” differentiated malignance be more difficult to diagnose than a “poorly” differentiated malignancy? Every time you think you understand the concept of differentiation, guys like Dr. John B. Gurdon and Dr. Shinya Yamanaka come along.
- The strong relationship between histology and biologic behavior
- The Mormon Tabernacle Choir
- Leiomyoma of the uterus. This benign, well-differentiated tumor contains interlacing bundles of neoplastic smooth muscle cells that are virtually identical in appearance to normal smooth muscle cells in the myometrium. Looking “good” means looking like the cells they supposedly arose from!
- Dysplasia means potential PRE-cancer. Anaplasia means cancer. The three words: pleomorphism, hyperchromasia, and increased mitoses, are the three most widely used terms to describe malignant tumors on pathology reports.
- Anaplastic large cell carcinoma of lung showing cellular and nuclear variation in size and shape. No differentiation into squamous or glandular epithelium is evident. This is what we mean when we say, it looks “bad”, i.e., pleomorphic, hyperchromatic. This is a classic image of a tumor in which any pathologist would call malignant as a knee jerk reflex after looking at it for one nanosecond, even if it took him 10 minutes to put his key into his car ignition that morning. Ugly and nasty are also two more terms commonly used. Looking “bad” means NOT looking like the cells they supposedly arose from!
- Do you remember from chapter 1 that DYS- was one of the seven -plasia brothers? Dysplastic cells are also often referred to as “atypical” cells.
- This epithelium shows severe dysplasia: Note that dysplastic basal cells characterized by cuboidal shape, high nuclear cytoplasmic ratio, hyperchromatism, mitotic activity, and some loss of orientation to the basement membrane, occupy the lower two thirds of the surface rather than just the basal row of cells. More differentiated cells which occupy the outer third, though still retaining some dysplastic nuclear features have the appearance of maturing squamous cells rather than basal cells, and eventually become flattened on the surface.
- Carcinoma in situ: This section shows that the dysplastic basiloid cells go all the way to the surface and never undergo significant differentistion towards more differentiated flattened squamous cells. Note however that the basement membrane is still intact. The torturingly and unnecessary insane pressure to differentiate “severe” dysplasias from carcinomas-in-situ has prompted the various “-IN” classification systems, e.g., CIN-III, VIN-III, PIN-III. Is high grade dysplasia any different from carcinoma-in-situ from a microscopic, behavioral, or medical-legal point of view? Ans: NO!
- Does “maturation” or “differentiation” make a cell lose its clonality? Answer: NO
- Figure 7-12 Biology of tumor growth. The left panel depicts minimal estimates of tumor cell doublings that precede the formation of a clinically detectable tumor mass. It is evident that by the time a solid tumor is detected, it has already completed a major portion of its life cycle as measured by cell doublings. The right panel illustrates clonal evolution of tumors and generation of tumor cell heterogeneity. New subclones arise from the descendants of the original transformed cell, and with progressive growth the tumor mass becomes enriched for those variants that are more adept at evading host defenses and are likely to be more aggressive. (Adapted from Tannock IF: Biology of tumor growth. Hosp Pract 18:81, 1983.)
- Figure 7-13 Schematic representation of tumor growth. As the cell population expands, a progressively higher percentage of tumor cells leaves the replicative pool by reversion to G0, differentiation, and death. Radiation and chemotherapy work on dividing cells, so the size of the non-proliferative pool is important. The MORE differentiated a cell is, the less likely it is to multiply.
- Some wise ass pathologist my tell you he knows of some benign tumors which metastasize.
- Can you imagine this tumor being well defined and/or being “encapsulated”?
- Note the sharply demarcated border and a thin capsule in this neoplasm which is composed of both proliferating fibrous stroma (fibro) and glands (adenoma). The tumor is at the right and normal breast is at the left. As shown in this view the fibroadenoma, a benign tumor, is well circumscribed and has a fibrous capsule. This view shows the proliferation of benign appearing fibroblasts (arrows) (i.e. the "fibro" component), and several glands (the "adeno" component).
- Can you imagine THIS tumor being well defined and/or being “encapsulated”? ANS: NO The invasiveness aspect of solid tumors is how “cancer” got its name, i.e., “crab”-like
- Invasiveness (aka, “infiltration”) has BOTH gross as well as microscopic connotations. The fibrous (i.e., “scirrous”) response is NOT considered to be neoplastic , like a teratoma or carcinosarcoma, but a reaction to the neoplasm. This fibrous response is also called desmoplasia.
- Adenocarcinoma of the breast. Note that the fibrous stroma of the beast is infiltrated by tumor cells arranged in nests with some gland formation. The dense fibrous stroma results in the tumor having a very firm consistency (scirrhous carcinoma). Every pathologist could look at this image, and instantly know it was carcinoma. You don’t have to zoom in and look at the nuclei, if the glands are growing every which way.
- If you did this autopsy, and you were blind, could you still diagnose metastatic disease to the liver? ANS: YES What if the “nodules” were all tiny and diffuse? Would you suspect cirrhosis instead? YES!
- Lymph node with metastatic adenocarcinoma. In this case only a few remnants of normal lymph node tissue are seen. Find them. In fact, this could even be a PRIMARY with some lymphoid tissue reacting to it, especially if you could not see the unique diagnostic features of a lymph node such as a subcapsular sinus.
- Adjuvant chemotherapy in breast cancer reduces the incidence of recurrence and metastasis, but is toxic. Such treatment is not advised when the risk of recurrence is very low. Grade and stage are important prognostic factors, but are being supplemented by newer biologic markers. Nodal dissections are NOT curative or even therapeutic, they are only PROGNOSTIC!!!!!!
- In some tumors, like smooth muscle tumors, counting mitoses may be the main way to differentiate a benign from a malignant process! “If you want to think od “anaplasia” as DE-differentiation, you can, but remember, differentiation NEVER occurs backwards! “LOCAL INVASION” is in HUGE ALL CAPS font because it is the single most important differentiating feature. ALL malignancies can potentially metastasize, but there is at least one common benign condition which is also said to “metastasize”. Can you name it? Is there an absolute line of difference between benign and malignant? Probably not.
- Figure 1 indicates the most common cancers expected to occur in men and women in 2005. Among men, cancers of the prostate, lung and bronchus, and colon and rectum account for more than 56% of all newly diagnosed cancers. Prostate cancer alone accounts for approximately 33% (232,090) of incident cases in men. Based on cases diagnosed between 1995 and 2000, about 90% of these estimated new cases of prostate cancer are expected to be diagnosed at local or regional stages, for which 5-year relative survival approaches 100%.
- Cancer INCIDENCE
- Cancer DEATH rates
- Notice that although there are FIVE bullets on this slide, it really is the THREE USUAL SUSPECTS, isn’t it? FAT is the biggest factor in the sex-specific, high incidence cancers, i.e., prostate and preast.
- Figure 7-25 The change in incidence of various cancers with migration from Japan to the United States provides evidence that the occurrence of cancers is related to components of the environment that differ in the two countries. The incidence of each kind of cancer is expressed as the ratio of the death rate in the population being considered to that in a hypothetical population of California whites with the same age distribution; the death rates for whites are thus defined as 1. The death rates among immigrants and immigrants' sons tend consistently toward California norms. (From Cairns J: The cancer problem. In Readings from Scientific American-Cancer Biology. New York, WH Freeman, 1986, p. 13.)
- EPIDEMIOLOGY of cancer
- A proto-oncogene is a normal gene that can become an oncogene due to mutations or increased expression. Proto-oncogenes code for proteins that help to regulate cell growth and differentiation.
- The various aspects of “malignant transformation”. Just like cancer itself is a progression of increasingly disturbing processes, so is malignant transformation. These are not necessarily exactly linear events, but close. Look at these as being factors in growth regulation.
- This is a BEAUTIFUL chart! Another way of understanding the development of malignancy in a logical way!
- Cyclins are a family of proteins that control the progression of cells through the cell cycle by activating Cyclin Dependent Kinase (cdk) enzymes CDK’s (kinases) are enzymes which PHOSPHORYLATE proteins in preparation for the next phase of the cycle. G1SG2M is regulated by Cyclins DEAB, respectively, and CDKs 4221, respectively.
- Signal transduction is a generic term which refers to any process by which a cell converts one kind of signal or stimulus into another.
- Note, in every case, there is a NORMAL gene (proto-oncogene) MUTATED to become an ONCOGENE, ultimately resulting in the expression of as tumor.
- Note, in every case, there is a NORMAL gene (proto-oncogene) MUTATED to become an ONCOGENE, ultimately resulting in the expression of as tumor.
- Note, in every case, there is a NORMAL gene (proto-oncogene) MUTATED to become an ONCOGENE, ultimately resulting in the expression of as tumor.
- Note, in every case, there is a NORMAL gene (proto-oncogene) MUTATED to become an ONCOGENE, ultimately resulting in the expression of as tumor.
- Myc (cMyc) codes for a protein that binds to the DNA of other genes. When Myc is mutated, or overexpressed, the protein doesn't bind correctly, and often is a big step in the ultimate production of cancer.
- These are the TWO other most important and widely studied genes in cancer. P53 seems to have a variety of functions, and mutations of this gene have a carcinogenic effect at several levels.
- A RAS protein
- It would be a good idea to have a familiarity with these genes, recognizing that mutations of them result in cancers. NOTE: Problems of GROWTH SUPPRESSION, result in GROWTH being UN-regulated. THESE ARE ALL GROWTH SUPPRESSOR GENES WHICH, WHEN MUTATED, LOSE THEIR NORMAL ABILITY TO SUPPRESS cell crowth!!!
- Mutations of genes resulting in EVASION of APOPTOSIS would also be a factor in carcinogenesis, wouldn’t it?
- Telomeres are a sequence of repetitive bases at the ends of linear chromosomes that prevent adjacent chromosomes from attaching to each other. Think about this? If a telomere is interfered with, perhaps by telomerase, it LOSES its ability to limit mitoses!
- Think about this too: A tumor could NEVER be more than 1-2 mm, if it did not have the ability to generate blood vessels to feed it? Right? Ans: YES
- Another AWESOME diagram! Most important diagrammatic explanation of malignancy I have ever seen. LinearLinearLinearLinearLinearLinearLinearLinearLinearLinearLinearLinear
- FOUR orderly steps of “INVASION” (aka, INFILTRATION, or INVASIVENESS)
- Detachment, 2) attachment, 3) degradation, 4) migration Google hits: “invasive carcinoma” = 300K “invading carcinoma” = 3K “infiltrating carcinoma” = 30K “infiltrative carcinoma” = 3K
- It would be wise to remember that these THREE genes are often discussed in the ability of tumors to METASTASIZE. They are metastatic SUPRESSOR genes. So once again, metastasis, like carcinogenesis, is a LOSS of regulation.
- Often the term “gene rearrangement” has been used.
- Many/Most leukemias/lymphomas have fairly predictable chromosome translocations. God help you if you try to memorize this.
- There is NO ONE SINGLE UNIFORM explanation as to what causes cancer. I hope you were not expecting to find it here?
- The Initiation/Promotion concept is what we have always know about the cause of cancer. You need TWO things: 2) carcinogens (i.e., initiators) and 2) proliferation (i,.e., promotors)
- The concept of initiation and promotion is NOT a new concept. We always knew you needed two things to cause cancer: Carcinogens, mutators Factors which normally cause hyperplasia, such as steroid hormones, replicators
- You know the drill by now!
- Direct carcinogens initiators cause mutations DIRECTLY. “Pro”-carcinogens initiators are metabolized into substances which are more direct. A glancing familiarity with all these compounds is a good thing to have. Having a vague recognition of these substances as being carcinogens would be a good idea. An initiator might cause the necessary mutations in growth regulating genes, but does not have an effect on cell proliferation. β-Propiolactone is a disinfectant, DMSO is an awesome solvent, Diepoxybutane is a preservative/textile-linking agent.
- As you might suspect, promotors are NOT carcinogenic by themselves, but often are agents of hyperplasia, e.g., steroid hormones. A “promotor” might cause hyperplasia in cells even without the effect of a carcinogen. You can think of a promotor as a “hyperplastic agent”. A woman may as: “Will estrogens increase my risk of cancer?”. Estrogens and steroid hormones in general are “promotors”.
- ALL THREE common types of skin cancer are related to UV radiation.
- The FIVE common viruses associated with cancers should also be in your recollection.
- CYTOTOXIC CD8+ T-CELLS are the main eliminators of tumor cells
- T cells require two signals to become fully activated. A first signal, which is antigen-specific, is provided through the T cell receptor which interacts with peptide-MHC molecules on the membrane of antigen presenting cells (APC). A second signal, the CO-STIMULATORY signal, is antigen nonspecific and is provided by the interaction between co-stimulatory molecules expressed on the membrane of APC and the T cell.
- Was the original name for TNF “cachexin”? Ans: Yes. Would you suspect PIF would be increased in cancer patients who have experienced weight loss?
- So if your patient presents with any of these conditions, should you always suspect an underlying malignancy? Ans: Yes.
- Often, the term paraneoplastic syndrome is used synonymously with ectopic endocrine hormone production. These words could not be seen in a real classroom, but they can be seen in a virtual one!
- Which one of these two is more important? This is a CRUCIALLY important question!
- The main question in grading is: HOW WELL do the tumor cells look like the NORMAL cells from which they arose? If they look A LOT like “normal” cells, it is a LOW grade with a GOOD prognosis, but perhaps a TUFF diagnosis. If they look NOT like “normal” cells, it is a HIGH grade with a BAD prognosis, but perhaps an EASY diagnosis.
- Immunohistochemistry (IHC) has become the “magic bullet” of diagnostic surgical pathology, based on the theory that even if you do NOT know what kind of tumor cell you are looking at, if you can identify specific antigens by staining for them, then, you can feel sure you know the cell of origin. IHC does NOT identify antigens which differentiate benign from malignant, but identify antigens common to certain types of cells!
- Yesterday: H&E, blue and red Today: Immunochemistry, brown Tomorrow: Arrays, yellow, green, red