Minarcik robbins 2013_ch27-nerve_musc
•Als PPT, PDF herunterladen•
1 gefällt mir•751 views


Empfohlen
Weitere ähnliche Inhalte
Was ist angesagt?
Was ist angesagt? (20)
Andere mochten auch
Ähnlich wie Minarcik robbins 2013_ch27-nerve_musc
Ähnlich wie Minarcik robbins 2013_ch27-nerve_musc (20)
Mehr von Elsa von Licy
Mehr von Elsa von Licy (20)
Kürzlich hochgeladen
Kürzlich hochgeladen (20)
Minarcik robbins 2013_ch27-nerve_musc
- 2. NEUROPATHIES, MYOPATHIES • NEUROPATHIES (7) • MYOPATHIES (9) – – – – Inflammatory Infectious Hereditary (HMSN-I) HMSN-II, HMSN-III – Acquired (Toxic/Metabolic) – Traumatic – Neoplasms –Denervation – – – – – – – – Dystrophies Ion Channel Congenital Genetic Metabolic Inflammatory Toxic NeuroMuscular Junction Neoplasms
- 22. GENERAL Reactions • NERVE – DEMYELINATION (segmental) – AXONAL DEGENERATION – NERVE REGENERATION – REINNERVATION • MUSCLE FIBER – NECROSIS – VACUOLIZATION – REGENERATION – ATROPHY – HYPERTROPHY
- 28. NEUROPATHIES, MYOPATHIES • NEUROPATHIES (7) • MYOPATHIES (9) – Inflammatory – Infectious – Hereditary (HMSN-I HMSN-II, HMSN-III) – Acquired Toxic/Metabolic – Traumatic – Neoplasms – – – – – – – – – Denervation Dystrophies Ion Channel Congenital Genetic Metabolic Inflammatory Toxic NeuroMuscular Junction Neoplasms
- 29. NEUROPATHY, Inflammatory • Guillain-Barré – Preceded by “influenza”-like illness – NO actual specific etiologic agent isolated, autoimmune disease to myelin gangliosides most likely – Inflammation of a peripheral nerve – DEMYELINATION – “ASCENDING” paralysis • Hands trunk • Feet trunk
- 30. Guillain-Barré, (AIDP), Acute Inflammatory Demyelinating Polyneuropathy
- 31. NEUROPATHY, Infectious • Leprosy • Diphtheria • V/Z (Varicella-Zoster)
- 36. NEUROPATHY, Hereditary (defective myelination) (Hereditary Motor and Sensory Neuropathy) • HMSN-I (Charcot-Marie-Tooth) • HMSN-II (Like CMT of the neurons) • HMSN-III (Palpable Nerves) (aka, Dejerine-Sottas) • …….IV, V, VI, VII
- 38. NEUROPATHY, Toxic/Metabolic Symmetric, Asymmetric Sensory, Sensorimotor Somatic, Autonomic Focal, Multifocal
- 39. NEUROPATHY, Toxic/Metabolic Diabetes Mellitus Vitamin Deficiencies (many Bs, E) Heavy Metals, Pb, As, etc. Organic Compounds CHEMO
- 40. DEMYELINATION
- 41. NEUROPATHY, Traumatic • • • • • • Laceration regeneration rate = 1mm/day or 1 in/mo. Avulsion Carpal Tunnel Traumatic (amputation) “Neuroma” “Saturday Night” Palsy (radial n.) Morton “Neuroma”
- 42. TRAUMATIC NEUROMA “Regenerating Axons and Glia (Schwann Cells), but with no direction”
- 43. MEDIAL Plantar Nerve 3rd COMMON digital branch MORTON’S NEUROMA Traumatic Compression F>M Interdigital Intermetatarsal
- 45. NEUROPATHY, Neoplastic Benign: Schwannoma Malignant: Malignant Schwannoma
- 47. Antoni A: “Palisaded” Antoni B: NON-Palisaded
- 48. QUIZ: • Why are Schwannomas the ONLY tumors of peripheral nerve?
- 49. MYOPATHIES
- 50. NEUROPATHIES, MYOPATHIES • NEUROPATHIES (7) – – – – – – – Inflammatory Infectious Hereditary (HMSN-I) HMSN-II, HMSN-III Acquired Toxic/Metabolic Traumatic Neoplasms • MYOPATHIES (9) – Denervation (SMA) – Dystrophies – Ion Channel – Congenital – Genetic Metabolic – Inflammatory – Toxic – NeuroMuscular Junction – Neoplasms
- 51. MYOPATHY, Denervation MUSCLE FIBERS CANNOT SURVIVE UNLESS THEY ARE INNERVATED PERIPHERAL NERVE PATHOLOGY ANTERIOR (ventral) HORN CELL PATHOLOGY
- 53. SPINAL MUSCULAR ATROPHY • Childhood diseases • Chromosome #5 that harbors the survival motor neuron gene (SMN1) • Anterior (ventral) Horn Cells • Often PAN-fascicular • Shoulder, hip muscles
- 55. MYOPATHY, “Dystrophic” • Jerry’s kids, no “DYSTROPHIN” • DUCHENNE (DMD), x-linked • BECKER (BMD) (less common, less severe, same chromosome) • Many others also, all of which have complex genetic patterns which have all been precisely defined • MYOTONIA is a common feature
- 56. NORMAL DMD
- 59. Limb Girdle Muscular Dystrophies Inheritance Locus Gene Clinicopathologic Features 1 A Autosomal-dominant 5q31 Myotilin Onset in adult life with slow progression of limb weakness, but sparing of facial muscles; dysarthric speech 1 B Autosomal-dominant 1q21 Lamin A/C Onset before the age of 20 years in lower limbs, progression during many years with cardiac involvement 1 C Autosomal-dominant 3p25 Caveolin-3 (Mcaveolin) Onset before the age of 20, clinically similar to type 1B 1 D Autosomal-dominant 7p Unknown Limb girdle muscle weakness, adult onset 2 A Autosomal-recessive 15q15.1-21.1 Calpain 3 Onset in late childhood to middle age; slow progression during 20–30 years 2 B Autosomal-recessive 2p13.3-q13.1 Dysferlin Mild clinical course with onset in early adulthood 2 C Autosomal-recessive 13q12 γ-Sarcoglycan Severe weakness during childhood, rapid progression; dystrophic myopathy on muscle biopsy 2 D Autosomal-recessive 17q21 α-Sarcoglycan (adhalin) Severe weakness during childhood, rapid progression; dystrophic myopathy on muscle biopsy 2 E Autosomal-recessive 4q12 β-Sarcoglycan Onset in early childhood, with Duchenne-like clinical course 2 F Autosomal-recessive 5q33 δ-Sarcoglycan Early onset and severe myopathy; dystrophic myopathy on muscle biopsy 2 G Autosomal-recessive 17q11-q12 Telethonin Distal weakness with limb-girdle weakness in late childhood to adulthood; rimmed vacuoles in muscle cells 2 H Autosomal-recessive 9q31-q34.1 Tripartite motifcontaining protein 32 (TRIM32) Limb-girdle and facial weakness with onset in childhood, mild, slowly progressive course
- 60. MYOPATHY, Ion Channel “Channelopathies” • MYOTONIA/HYPOTONIC PARALYSIS • FAMILIAL, (genetic) DISEASES • TRIGGERED BY: – Exercise – Cold – Carb Intake • Classified by K+, ↑K+, ↓K+ • MALIGNANT HYPERTHERMIA can be triggered off by anesthetic halogenated inhalation agents in some of these patients!!!
- 61. MYOPATHY, Congenital “Floppy Babies” • HYPOTONIC • FAMILIAL, (genetic) DISEASES • MANY TYPES, in most of which the precise genetic defects have been identified
- 62. MYOPATHY, Metabolic (genetic also) • LIPID – Mitoch. Enz. Def. LIPID ACCUMULATION • MITOCHONDRIAL – “PARKING LOT” mitochondria
- 65. MYOPATHY, Inflammatory • DERMATOMYOSITIS • POLYMYOSITIS • INCLUSION BODY MYOSITIS • ALL HAVE UNCLEAR ETIOLOGIES
- 68. INCLUSION BODY MYOSITIS (IBM) , “rimmed” vacuoles
- 69. MYOPATHY, Toxic • THYROTOXICOSIS • ETHANOL • DRUGS (steroids, chloroquine) • DRUGS (MANY MANY others)
- 70. MYOPATHY, NeuroMuscular Junction • Myasthenia Gravis – – – – – – Associated with thymomas Thymectomies often useful Rx: AUTOIMMUNE DISEASE, CLEARLY Ab’s to ANTI-CHOLINESTERASE RECEPTORS Anticholinesterase test is very diagnostic (edrophonium) YOUNG WOMEN WITH EYE MUSCLE SYMPTOMS: • Ptosis • Diplopia • General Weakness • Lambert-Eaton Syndrome (paraneoplastic), 60% have malignancies, auto-antibodies against NMJx
- 71. MYOPATHY, Neoplastic • Benign –Rhabdomyoma • Malignant –Rhabdomyosarcoma
Hinweis der Redaktion
- Very simple format, 7 common neuropathies, 9 common myopathies. Our original day 1 design of three types of diseases for everything is modified a bit! Notice the LARGE print. Note how they, sorta, fit into the 3 disease types.
- LONGITUDINAL H&E section of a peripheral myelinated nerve. Does the word “wavy” come to mind? Wavy Wavy Wavy Wavy Wavy Wavy Wavy Wavy Wavy Wavy Wavy Wavy Wavy Wavy Wavy Wavy Wavy Wavy Wavy Wavy Wavy Wavy Wavy Wavy Wavy Wavy Wavy Wavy Wavy Wavy Wavy Wavy Wavy Wavy Wavy Wavy Wavy Wavy Wavy Wavy Wavy Wavy Wavy Wavy Wavy Wavy Wavy Wavy Wavy Wavy Wavy Wavy Wavy Wavy Wavy Wavy Wavy Wavy Wavy Wavy Wavy Wavy Wavy Wavy Wavy Wavy Wavy Wavy Wavy Wavy Wavy Wavy Wavy Wavy Wavy Wavy Wavy Wavy Wavy Wavy Wavy Wavy Wavy Wavy Wavy Wavy Wavy Wavy Wavy Wavy Wavy Wavy Wavy Wavy Wavy Wavy Wavy Wavy Wavy Wavy Wavy Wavy Wavy Wavy Wavy Wavy Wavy Wavy Wavy Wavy
- TRANSVERSE H&E section of a peripheral myelinated nerve. Is this the same “wavy” thing now cut transversely? Ans: Yes What are all the bullseyes? (axons) What are the clear areas around the bullseyes? (fatty myelin, washed out)
- SILVER STAIN showing black axons surrounded by washed out fat (myelin)
- MYELIN stain showing the REVERSE of the previous slide. If you flip back and forth between this pic and the previous one, it will be like overlaying the negative of a film over the positive.
- Medium sized nerve, transverse section, showing a finite number of myelinated axons and schwann cells
- How many axons are in this nerve section? Perhaps around 20? Ans: YES
- Classical neurovascular “triad”: Artery, Vein, Nerve
- Smaller neurovascular triad, or “bundle”. How many axons are in this small nerve? Perhaps 5-8?
- The more longitudinally a nerve happens to be sectioned, the more “wavy” it appears.
- Electron microscope section, peripheral nerve. How many axons are myelinated? Perhaps about 7? Are the rest UN-myelinated? YES
- Please differentiate between microtubules (small circles) and neurofilaments (dots). Find the schwann cell nucleus, find an UNmyelinated axon, find a mitochondrion.
- Note that the myelin “layering” has to start (INNER mesaxon) and end (OUTER mesaxon) somewhere!
- It looks like one micrometer (micron) would span about 60 layers of myelin? True or false? Ans: TRUE
- Slam dunk classical appearance of skeletal muscle. Why is skeletal muscle or voluntary striated muscle a better name for this than just striated muscle? Ans: Because cardiac muscle also has striations. Logs on a fireplace may overlap with each other, even diagonally a bit, but they do NOT fuse.
- Is the peripheral nature of skeletal muscle nuclei more apparent from cross or longitudinal sections? Ans: Cross Why? Ans: Simple geometry! Are striations better seen on cross or longitudinal sections? Ans: Longitudinal Why? Ans: Simple geometry again!
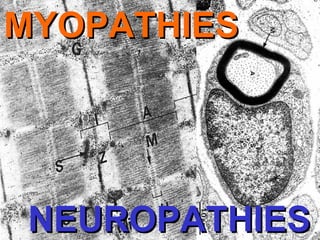
- EM, skeletal muscle, the sarcomere, like America, extends from “Z” to shining “Z”! Find glycogen. Find Mitochondria.
- H gets smaller with contraction!
- Find the sarcoplasmic reticulum, which is the endoplasmic reticulum of skeletal muscle. Find MYOSIN filaments, find ACTIN.
- These are NON-SPECIFIC reactions of nerve and skeletal muscle to injury. NON-specific, NON-specific, NON-specific. Much of it is realated to the concepts we talked about in chapter 1.
- Extremely important concepts of nerve demyelinization, axonal damage, and regeneration
- Just about anything which stains FAT will be ABSENT in areas of DE-myelinization.
- Muscle fiber necrosis
- Muscle fiber vacuolization
- Muscle fiber hypertrophy/atrophy. Certain fibers hypertrophy to make up for the loss of atrophic fibers
- Can you still appreciate the “waviness”?
- Why is auto-amputation common in severe leprosy? Ans: Nerve destructioon
- Why a dermatomal distribution?
- CMT is a very HETEROGENEOUS group of hereditary diseases involved with defective myelination, e.g., CMT1, CMT2, CMT3, CMT4, X-linked CMT. Often, but not exactly correctly, the HMSNs are used interchangeably with the term CMT. Duplication of a large region in chromosome 17p12 that includes the gene PMP22, is seen in 80% of CMT cases.
- 1) Peroneal muscle atrophy and 2) HIGH arching (pes cavum) is common in CMT, including 3) “claw” toe.
- BOTH demyelination/ischemia AND a direct TOXIC effect to peripheral nerves are seen in diabetes, which is the MOST COMMON cause of neuropathy, not to mention the severe ischemia.
- Do you think the word “neuroma” is in quotes because it is NOT a true clonal proliferative neoplasm? Ans: YES
- Morton’s Neuromas most commonly occur in the 3rd common digital branch of the MEDIAL plantar nerve, i.e., 3rd and 4th toe at the distal metatarsal level. They were NOT discovered by Morton, and they are not truly “neuromas”, in the true neoplastic sense of the word.
- Schwannoma But really, could this be ANY soft tissue tumor?
- Antoni A: Palisading, “Verocay” bodies Antoni B: Edema, “myxoid”
- Because SCHWANN cells are the ONLY nucleated cells found IN a nerve, dummy!
- A myopathy is ANY primary disease of muscle, generally striated muscle.
- The differential diagnoses of the various myopathies does not seem to follow the classical three divisions at all.
- Hypertrophy/Atrophy scenario. Are some fibers thicker to make up for the thinning (atrophy) of other fibers? Yes!
- What is myotonia? Ans: tonic muscle spasm or muscular rigidity
- Dystrophin, an intracellular protein, forms an interface between the cytoskeletal proteins and a group of transmembrane proteins
- Hypertrophy, atrophy, inflammation.
- Note again the atrophy/hypertrophy scenario
- MDA is not just DMD and BMD
- http://en.wikipedia.org/wiki/Channelopathy
- Floppy baby is not a disrespectful term.
- Metabolic myopathies are related to MITOCHONDRIA
- Do you thing the DARK lipid looks this way because it is stained with a lipophilic dye rather than having it’s usual washed out appearance?
- Does an “unclear” inflammatory etiology usually suggest autoimmune” Ans: YES
- Half of dermatomyositis patients also have cancer, many are young adults and therefore there is a juvenile variant. Note the eyelid appearance and eyelid edema.
- No skin changes, only in adults, no big association with cancer, and the inflammation is ENDOMYSEAL rather than PERIVASCULAR.
- Very obscure disease, but said to be the most common acquired myopathy in people over the age of 50. Quads and wrist flexors, asymmetrically, is the rule.
- Edrophonium is a acetylcholinesterase inhibitor, thereby relieving the symptoms temporarily.
- Exceedingly RARE tumors, you may see, possibly ONE rhabdomyosarcoma in your life, perhaps. When you do, you will know 50X more about it than I am going to describe now. This was also discussed in the domain of “soft tissue” tumors.