
Empfohlen
Weitere ähnliche Inhalte
Was ist angesagt?
Was ist angesagt? (20)
Ähnlich wie Av canal defect
Ähnlich wie Av canal defect (20)
Mehr von drsrb
Kürzlich hochgeladen
Kürzlich hochgeladen (20)
Av canal defect
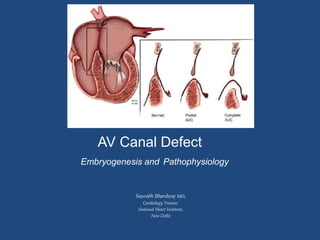
- 1. AV Canal Defect Embryogenesis and Pathophysiology Saurabh Bhardwaj MD, Cardiology Trainee, National Heart Institute, New Delhi
- 2. Introduction • Atrioventricular canal defects or Endocardial cushion defects or Atrioventricular septal defects (AVSDs) are a group of anomalies that share a defect of the atrioventricular septum and abnormalities of the atrioventricular (AV) valves. • Divided into partial and complete forms. • In Partial- primum atrial septal defect (ASD) with 2 distinct, but focally contiguous, right and left AV valve orifices. The left AV valve invariably is cleft. • In Complete- a primum ASD, but it is contiguous with a large inlet ventricular septal defect (VSD) and the common AV valve has a single orifice.
- 3. Anatomic Features Shared by All Forms of AVSD ▪AV valve leaflets insert at the same level at the cardiac crux ▪Absence of the AV septum ▪Unwedged and anterior displacement of the aortic valve ▪ Elongated LVOT ▪Counterclockwise rotation of the LV papillary muscles ▪Cleft left AV valve component, directed toward the ventricular septum
- 4. Embryogenesis • Due to faulty development of the AV endocardial cushions. • Dorsal mesenchymal protrusion that may act alone or in concert with development of the endocardial cushions to create AVSDs. • The primum atrial septal component of this defect is variable in size and can be quite large resulting in downward displacement of the anterior left AV valve leaflet to the level of the septal right AV valve leaflet. • In AVSDs, the AV valves have the same septal insertion level in contrast to the leaflet arrangement in the normal heart. The distance from the cardiac crux to the left ventricular apex is foreshortened, and the distance from the apex to the aortic valve is increased. • In AVSDs, the disproportion between the two distances causes anterior displacement of the LVOT resulting in elongation and narrowing of the LVOT producing the characteristic “gooseneck” deformity.
- 5. Partial AVSD • Incomplete fusion of the superior and inferior endocardial cushions results in a cleft in the midportion of the left AV valve anterior leaflet often associated with regurgitation. • Right and left AV valve orifices are separated by a tongue of tissue, frequently consists of a primum ASD and a cleft left AV valve anterior leaflet. • Most primum ASDs are large and located anterior and inferior to the fossa ovalis. • The defect is bordered by a crescentic rim of atrial septal tissue posterosuperiorly and by AV valve continuity anteroinferiorly. • These defects are not amenable to transcatheter device closure because of their proximity to the AV valves. • The most common associated anomalies with partial AVSD are secundum ASD, patent ductus arteriosus (PDA), and persistent left superior vena cava connecting to the coronary sinus
- 6. Partial AVSD with atrioventricular valve anatomy • Top left: Systolic apical four-chamber image demonstrating that both right and left atrioventricular valves insert onto the crest of the ventricular septum at the same level. • Top right: Corresponding diastolic frame revealing a large primum ASD. Systolic frames often understate the size of the interatrial communication. There is significant right atrium (RA) and right ventricle (RV) enlargement. Bottom panels: These are transthoracic parasternal short-axis scans focused at the alve leaflet level in the left ventricular inflow. • Left panel demonstrates the cleft in the anterior leaflet of the left atrioventricular valve (asterisk). The anterior leaflet is made of two separate components that move independently. This creates the diastolic gap in the leaflet (asterisk). • Color Doppler imaging on the right panel shows considerable regurgitation through the cleft.
- 7. Complete Atrioventricular Septal Defect • Lack of fusion between the superior and inferior cushions and, consequently, with the formation of separate anterior and posterior bridging leaflets along the subjacent ventricular septum. • Characterized by a large septal defect with interatrial and interventricular components and a common AV valve that spans the entire septal defect. • The septal defect extends to the level of the membranous ventricular septum, which is usually deficient or absent. • Two lateral leaflets correspond to the posterior tricuspid and posterior mitral leaflets in a normal heart. • The rightsided anterior leaflet, represents the normal anterior tricuspid leaflet, and the so-called anterior bridging leaflet corresponds to the superior half of the anterior mitral leaflet
- 8. Pathologic specimens of complete AVSD. A. Right anterior oblique view with right atrial and right ventricular free walls removed, demonstrating a large septal defect. B. Left posterior oblique view (same specimens as in A) with left atrial and left ventricular free walls removed, showing the same septal defect. C. Short-axis view, illustrating a type A common atrioventricular valve with five leaflets. D. Four-chamber view, showing secondary right ventricular hypertrophy and right atrial dilation. E. Short-axis view of a biventricular specimen removed during cardiac transplantation, showing an unbalanced form of AVSD with dilation of a common inlet right ventricle, leftward septal bowing, and a hypoplastic left ventricle. F. Four-chamber view of a complete AVSD associated with right atrial isomerism, mirror-image ventricles (L-loop ventricular inversion), and asplenia.
- 9. Rastelli Classification for Complete AVSD Type Anterior Bridging Leaflet and Chordae A Divided and attached to crest of ventricular septum. Multiple chordae. B Partly divided, not attached to crest of the septum. Chordae attach to papillary muscle in RV usually on septal surface. C Not divided and not attached to the crest of the septum (“free floating”). Chordae attach to papillary muscle on RV free wall.
- 10. Clinical Compendium 1. AVSDs account for 4% to 5% of congenital heart defects with an estimated occurrence of 0.19 in 1,000 live births. 2. Approximately 40% to 45% of children with Down syndrome have congenital heart disease, and among these, 45% have an AVSD. – Most patients with Down syndrome, who have congenital heart disease, have the complete form of AVSD (>75%). – Conversely, 50% of patients with AVSD have Down syndrome. 3. In the modern era, adult survival with excellent quality of life is expected for children born with AVSD. However, 15% to 20% of these patients may face reoperation in their lifetime. 4. The repair of AVSD has been one of the success stories in the field of congenital heart surgery over the last 5 decades. 5. All of these patients require lifelong surveillance for development of LVOT obstruction and left AV valve regurgitation.
- 11. Thanks “The saddest aspect of life right now is that science gathers knowledge faster than society gathers wisdom.” ― Isaac Asimov