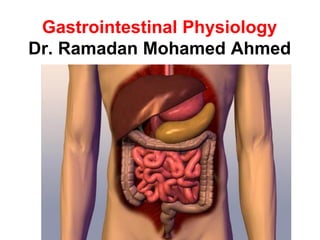
2. Gastrointestinal tract is a continuous tube that consists of the mouth, pharynx, esophagus,
stomach, small intestine, large intestine, and anus.
The lumen of this tube is continuous with the external environment.
The accessory organs are the salivary glands, exocrine glands, and biliary system (liver and
gallbladder).
pharynx
Upper
esophygeal
sphincter
Lower esophygeal
sphincter
stomach
Descending colon
duodenum
cecum
anus
rectum
liver
Salivary gland
larynx
esophagus
3. Functions of the digestive system
This system has four functions:
1. Motility is the muscular contractions that mix and move
the contents forward of the digestive tract.
2. Secretion is the transfer of digestive juices by exocrine
glands into the digestive tract.
3. Digestion is the hydrolysis of large molecules (e.g.,
carbohydrates, proteins, and fats) into their smaller
subunits.
4. Absorption is the passage of the products of digestion
from gastrointestinal lumen into the blood.
4. The wall of the digestive tract
consists of four layers;
• The mucosa lines the luminal surface. Its
inner epithelial layer has exocrine and
endocrine cells.
• The submucosa is under the mucosa This
connective tissue has large blood and lymph
vessels. It contains a submucous plexus.
• The muscularis externa is the main smooth
layer of the digestive tube. The muscularis
externa has an inner circular layer and an
outer longitudinal layer. A myenteric plexus
is between the two smooth muscle layers.
• Serosa: outer protective layer.
6. 6
Innervation of the GIT
1- Intrinsic innervation
A- The Myenteric plexus:
It controls mainly the motor function (motility) of the GIT.
B- The Submucosal plexus:
It controls mainly the secretory function of the GIT and the blood flow.
2- Extrinsic innervation:
A- Parasympathetic nervous system:
It is usually excitatory on the functions of the GIT.
B- Sympathetic nervous system:
It is usually inhibitory on the functions of the GIT.
7. Fig. 15-3, p. 471
External
influence
Local changes in
digestive tract
Receptors in digestive tract
Intrinsic
nerve plexuses
Extrinsic
automatic
nerves
Gastrointestinal
hormones
Smooth muscle
(contraction for motility)
Exocrine gland cells
(secretion of digestive juices)
Endocrine gland cells
(secretion of gastrointestinal
and pancreatic hormones)
Self-
excitable
= Short reflex
= Long reflex
= Hormonal pathway
Regulation of
GIT function.
8. Chewing
** is the first step in digestive process
** is can be voluntary or reflex (involuntary) action.
It’s functions
1. Breaks food up into smaller pieces to facilitates
swallowing
2. Mixes food with saliva
3. Stimulates taste buds by exposing them to food
11. Basic saliva components
• Water 99.5%
• Ions: Na+, K+, Ca2+, Cl–, HCO3
–
• Enzymes: salivary amylase
• Immunoglobolins: IgA
• Mucus: lubrication of food and protection of oral mucosa
• Lysozyme. (bacterial killing enzyme)
• pH of saliva is about 7.
12. Innervation of salivary glands
Excitation of parasympathetic nerve fibers causes:
- Increased watery secretion rich in enzymes
Excitation of sympathetic nerve fibers causes:
- Slight increase in viscid saliva (rich in mucus)
13. Cerebral cortex Other inputs
Salivary center
in medulla
Conditioned
reflex
Pressure receptors
and chemoreceptors
in mouth
Unconditioned reflex Autonomic nerves
Salivary glands
Salivary secretions
Control of salivary secretion.
14. Function of Saliva
1. Moistens oral mucosa .It facilitates speaking and chewing.
2. Moistens dry food, lubricates food to facilitate swallowing and cools hot
food.
3. Provides a medium for dissolved foods to stimulate the taste buds.
4. Buffers oral cavity contents. Saliva has a high concentration of
bicarbonate ions.
5. Digestion. Alpha-amylase, contained in saliva, breaks down
polysaccharides into disaccharides, while lingual lipase helps break down
fats.
6. Neutralizes any gastric acid that refluxes from stomach
into the lower esophagus.
7. Mineralization of new teeth and repair of precarious enamel lesions.
Saliva is high in calcium and phosphate.
8. Contains antibacterial compounds. Thus, problems with the salivary
glands generally result in dental caries .
15. The process of food coming into
the stomach from oral cavity .
Swallowing
1.Voluntary stage Oral cavity Pharynx
2.Pharyngeal
stage
Pharynx Esophagus
3.Esophageal
stage
Stomach
Esophagus
17. 1.Voluntary stage Oral cavity Pharynx
The pressure of the tongue upward and
backward against the palate.
18. 2.Pharyngeal stage Pharynx Esophagus
Receptors (pharynx)
Brain stem
Series of automatic pharyngeal muscle contractions
19. Pharyngeal stage
Impulses coming from swallowing center to pharynx and
esophagus to finish stage 2 and 3 of the swallowing
act. In pharyngeal stage, the following events
occur:
1. pushing the soft palate upward to prevent reflux of
food to nasal cavity.
2. to prevent passage of food into trachea. This done by
a. The vocal cords are tightly closed
b. larynx is elevated
c. Epiglottis swing back over the opening of larynx.
3. Relaxation of upper esophageal sphincter
4. Pharyngeal muscle contraction starts (peristalsis) from
upper parts and spreading down ward
20. trachea
(windpipe)
glottis
During breathing, the
larynx is lowered and
the glottis is open.
pharynx
oesophagus
larynx
(voice-box)
air
What Happens During Breathing
and Swallowing?
Normally, air passes into
the trachea (windpipe)
while food passes into
the oesophagus.
21. 21
During swallowing, the
larynx is raised and the
glottis is covered by the
epiglottis. This prevents
food particles from
entering the trachea.
pharynx
trachea
(windpipe)
oesophagus
glottis
epiglottis
food
particles
larynx
(voice-box)
What Happens During Breathing
and Swallowing?
22. (3) Esophageal stage
• Movement of bolus through esophagus is
through peristalsists:
• Primary peristalsis is continuation of
pharyngeal peristalsis which takes 5-9 second
to travel along the esophagus. This peristalsis is
capable to push the bolus down ward.
• Secondary peristalsis starts if primary
peristalsis fails to push the bolus downward and
will continue until the esophagus is empty. This
peristalsis is initiated by distention of the
esophagus by retained food. It is due to
stimulation of the myentric plexus in the wall of
esophagus.
23. VOMITING
The sudden and forceful expulsion of gastric and upper
intestinal contents
* It is controlled by neurons in medulla (the ‘vomiting
centre’)
*It is triggered by one or more of the following stimuli:
- excessive gastric or duodenal distension
- noxious substances in stomach
- certain smells or sights
- emotional factors
- touch receptors at back of throat
- reflexes involving semi-circular canals (‘motion
sickness’)
- stimulation of the ‘chemoreceptor trigger zone’ by
circulating ‘emetics’
24. THE VOMITING REFLEX
SEQUENCE OF EVENTS
• It starts by salivation and sensation of nausea
• Deep inspiration
• Closure of glottis (to prevent passage of vomit into airways)
• Elevation of uvula (to prevent passage of vomit into nasal cavity).
• Relaxation of lower esophageal sphincter
• Contraction of diaphragm and abdominal muscles causes increased
intra-abdominal pressure.
• Rapid rise in intra-gastric pressure causes reverse expulsion of
gastric and upper parts of small intestine contents
*** Vomiting of gastric content alone for prolonged time leads to
metabolic alkalosis
26. Functions of the stomach
1- Storage of food: stomach can store large amount of food to be
stored during the day.
2- Evacuation: evacuation of food into the intestine occur slowly
over a long time to allow intestinal digestion and absorption.
3- Digestion: partial digestion of proteins and fats.
4- Antibacterial action: by the high acidity to kill most of
microorganisms
5- Secretion of intrinsic factor: which is essential for vit. B12
absorption.
6- Absorption: of small amount of water and alcohol.
7- Iron absorption: is facilitated by HCl.
28. 28
Functions of HCl
• Kills many bacteria.
• Helps protein digestion by conversion of pepsinogen to
pepsin.
• Helps absorption of Ca++and iron.
29.
30. Pepsinogen:
It is inactive enzyme, activated by HCl in gastric lumen into active
form Pepsin. It initiate protein digestion.
Mucous: It serves as a protective barrier.
1- Lubricating properties: it protects the gastric mucosa against
mechanical injury
2- It protects the stomach wall from self-digestion because
pepsin is inhibited when it comes in contact with the mucous
layer coating the stomach.
3- Being alkaline, protecting against acid in injury by neutralizing
HCI in the vicinity of gastric lining.
31. 31
Gastric Mucosal Barrier (GMB)
[1] Luminal membrane impermeable to HCL.
[2] Tight junctions between cells.
Ulcer
Peptic ulcer in oesophagus, stomach or duodenum
Weakness in GMB.
Increased acidity leads to increased histamine leading
to increased acidity and a vicious cycle
Helicobacter Pylori 90% of peptic ulcers
32. 32
Control of gastric secretion
• Gastric secretions in response to a meal are divided into 3 phases:
1-Cephalic phase: Represent 30% of the response.
• Conditioned: Sight, smell, sound and even thinking of food lead to
secretions of HCL, pepsin and mucous.
• Unconditioned: Stimulation of taste, touch & thermal receptors in the
mouth.
2- Gastric phase: 60% of acid secretions:
• The presence of food in the stomach increases gastric secretions. it is through
gastrin hormone and stimulation of intrinsic nerve plexuses.
3- Intestinal phase:
• Accounts only for 10% of secretions, protein digestion products stimulate acid
secretion.
33. 33
The Pancreatic Secretion
▪ The pancreatic secretion is about 1200-
1500ml/day. Its PH is alkaline (7.6-8.2).
Composition of pancreatic juice:
The pancreatic juice is composed of pancreatic
enzymes secreted by the acinar cells and
bicarbonate solution secreted by the duct cells.
1- Pancreatic enzymes:
Pancreatic juice contains enzymes for digestion of
all types of food. These enzymes are secreted by
the acini of the pancreatic glands.
34. 34
1- Pancreatic Enzymes
The pancreatic enzymes include:
A- Enzymes for protein digestion:
1- Trypsin and chymotrypsin
2- Carboxypeptidases:
3- Ribonuclease and deoxyribonuclease:
These enzymes digest RNA and DNA.
B- Enzymes for fat digestion:
1- Pancreatic lipase which digest fats.
2- Cholesterol esterase and Phospholipase.
C- Enzymes for carbohydrate digestion:
Pancreatic amylase
35. 35
2- Bicarbonate Secretion
The pancreatic juice contains high bicarbonate content that
neutralizes the acidic chyme that reaches the duodenum thus
regulates the PH of the upper small intestine. Bicarbonate is
secreted by the epithelial cells of pancreatic ducts.
37. Regulation of Pancreatic Secretion
The pancreatic secretion is regulated by hormonal
and nervous regulation.
A- Hormonal regulation:
1- Cholecystokinin hormone (CCK):
It stimulates pancreatic secretion rich in enzymes.
2- Secretin hormone:
It stimulates pancreatic secretion rich in bicarbonates.
B- Nervous regulation:
Vagal stimulation stimulates enzyme secretion by cells and
increases the action of secretin on bicarbonate secretion.
38. 38
Regulation Of Pancreatic Secretions
Pancreatic enzymes released
Acinar cells stimulated
Cholecystokinin secreted
Protein/Fat/Carb
Sodium bicarbonate released
Duct cells in pancreas stimulated
Secretin secreted
Acid
Chyme Enters Duodenum
39. 39
Gastrointestinal hormones
Hormone Secreted by: Actions
1- Gastrin
2.Cholecystokinin
(CCK)
3- Secretin
G-cells of the gastric
antrum and duodenum
the upper part of the
small intestine
the upper part of the
small intestine.
1- Stimulates HCL secretion.
2- Stimulates gastric motility.
3- Tropic to gastric mucosa.
1- stimulate pancreatic enzymatic
secretion
2- Stimulates the contraction of gall
bladder.
1-Stimulates pancreatic secretion rich
in alkalie
2- stimulate bile secretion from the
liver
42. 42
Functions of the Liver
1. Regulation of blood glucose concentration
– 70-90mg of glucose / 100cm3 of blood (normal conditions)
2. Production of bile
– Liver produces bile which is stored in the gall bladder
43. Functions of the liver
3. Iron storage
– Red blood cells are destroyed in the spleen and
their haemoglobin is sent to the liver to be broken
down. The iron released is then stored in the liver.
4. Protein synthesis
– Liver synthesizes proteins found in blood plasma,
e.g. albumins, globulins, fibrinogen
44. Functions of the liver
5. Detoxification
– Liver cells contain alcohol dehydrogenase to
break down alcohol.
– Prolonged alcohol abuse may lead to liver
cirrhosis.
6- Protective role: removal of bacteria, due to the
presence of Kupffer cells or macrophages.
7- Excretion of cholesterol and bilirubin.
8- Activation of vitamin D.
45. 45
Bile Salts
Functions of bile salts:
1- Emulsification of fats:
Bile salts reduce surface tension and
emulsify fats into small droplets preparatory
to their digestion by pancreatic lipase.
2- Absorption of fats:
Bile salts are amphipathic i.e. one surface is
hydrophilic and the other is hydrophobic.
Thus bile salts tend to form cylindrical discs
called micelles, with the hydrophilic surface
facing out and a hydrophobic center
containing fats. Thus, micelles keep fats in
solution and transport them to the brush
border of small intestine (?) where they are
absorbed.
3- Help absorption of fat soluble vitamins:
Vitamin A, D, E and K.
4- Stimulate intestinal motility.
46. 46
The Bile
Pigments
• Bilirubin is a greenish yellow pigment formed as an end
product of hemoglobin metabolism.
• In the plasma bilirubin combines with albumin to form free
bilirubin (?).
• Free bilirubin is not excreted in urine (why?).
• Free bilirubin enters the liver cells where it is conjugated with
glucuronic acid forming conjugated bilirubin.
• Conjugated bilirubin is excreted by the liver cells in bile to
reach the intestine.
• In the intestine conjugated bilirubin is converted by bacterial
action to urobilinogen which is changed to stercobilinogen and
excreted in feces where it is oxidized to stercobilin.
48. Jaundice:
It is the yellowish tint of the skin and mucous membrane as a result of
increased levels of free or conjugated bilirubin (normal level?).
Types of Jaundice:
1- Hemolytic jaundice: It is due to excessive hemolysis of RBCs
and increased production of free bilirubin. Thus plasma levels of free
bilirubin increase.
2- Hepatocellular jaundice: It is due to inability of the liver cells to
conjugate all free bilirubin and to excrete all the conjugated bilirulin.
Thus free and conjugated bilirubin increase in plasma.
3- Obstructive jaundice: It is due to obstruction of bile flow. Thus the
level of conjugated bilirubin increases in plasma.
49. The Gall Bladder
Functions:
1- Storage of bile.
2- Concentration of bile
3- Acidification of bile.
Control of gall bladder evacuation:
1- CCK: The most important stimulus for gall bladder evacuation.
2- Vagal stimulation.
51. Small Intestinal Motility
Types of small intestinal motility:
A- Segmentation movement:
1- They are ring like contractions that appear at
regular intervals along the gut and then disappear
and are replaced by another set of ring contractions
in the segments between the previous contractions.
2- They move the food to and fro and increase its
exposure to mucosal surface.
3- These to an fro movements cause mixing of food
without any net forward movements.
B- Peristalsis:
1- circular contraction behind the bolus of food and an
area of relaxation in front of it.
2- The wave of contraction then moves in a forward
direction propelling the contents of the lumen
forward through the small intestine toward the large
intestine.
53. 53
Small Intestinal secretion
1- Mucus:
• a- secreted by bruners glands and goblet cells.
• b- Functions:
• - Protection of duodenal mucosa against acidic gastric juice .
• - Lubrication and facilitation of passage of food along intestine .
2- Alkaline fluid:
• - An isotonic alkaline fluid (ph 7.5) containing mainaly NaHCO3 but no
digestive enzymes .
• - After secretion it is rapidly reabsorbed by the villi, thus it dissolves the
chime and act as a watery vehicle for absorption of various substances from
the small intestine.
3- Sloughed mucosa containing digestive enzymes (cellular enzymes):
• Large number of mucosal cells (cotaining digestive enzymes) is
continuously sloughed (sheded) into the intestinal lumen and gets mixed
with intestinal secretion.
54. Absorption
Adaptations of the small intestine
• Small intestine is very long (~5 m)
• Internal surface of the small intestine has
many folds.
• On these folds, there are many finger-like
projections called villi
• These 3 adaptations increase surface
area for absorption
56. 56
Lacteal – fatty acids
and glycerol recombine
in the epithelium to
form fat which then
enters the lacteal as
fine fat droplets
Blood capillaries –
transport sugars
and amino acids
away from the
small
intestine
One cell thick epithelium –
for efficient absorption of
food particles
This continual transport of digested food substances
maintains the concentration gradient for the absorption
of digested food substances.
57. What happens to amino acids and glucose
after absorption?
Products released from liver into general
blood circulation
Molecules pass into the epithelial cells
Through walls of capillaries in the villus and into bloodstream
The capillaries join up to form veins
Veins unite to form 1 large vein: Hepatic Portal Vein
Hepatic portal vein carries blood to liver
Liver stores or alters products of digestion
58. What happens to fatty acids and glycerol
after absorption?
Molecules pass into the epithelial cells
Recombine into fats again in the epithelial cells
Fats enter the lacteals
Lymph (fluid in lacteals) + fat = chyle
Lymphatic vessels discharge chyle into
bloodstream
60. Function of large intestine
• Absorption of H2O and electrolytes from chime by proximal colon
(absorbing colon).
• The large intestine can absorb a maximum of 5 to 8 liters of fluid and
electrolytes each day.
• Storage of feces by distal colon (storage colon)
• Defection by rectum and anal canal: Defection is the act of emptying the
colon contents through the anal canal.
• Secretion (Mucus Secretion).
• Bicarbonate neutralizes acids: produced by local bacteria fermentation.
62. Defecation
Haustral contractions = slow =allow bacteria to brow in large intestine
Ascending and transverse colon contract simultaneously to drive faeces to
descending colon.
Once faeces reaches the rectum, it stretches and sphincters relax
External sphincter is skeletal voluntary muscle
Abdominal muscles contract and the individual breaths a sigh of relief.