1. P E R I O D O N T I CPSE R I O D O N T I C S
Periodontal Splinting in General
Dental Practice
SOPHIE J. WATKINS AND KENNETH W. HEMMINGS
(drifting) of periodontally involved
Abstract: Splinting periodontally involved teeth is a technique that has been in use for teeth.
centuries. This article gives a brief history and review of the literature concerning periodontal
splinting and outlines the rationale and indications for the correct application of periodontal
splinting in modern dental practice. The common types of splint and clinical techniques A variety of factors can contribute to
involved are described, addressing some of the clinical problems. tooth mobility, including trauma;
periapical or periodontal inflammation,
Dent Update 2000; 27: 278-285 decreased periodontal support and
pathologically increased occlusal load.
Clinical Relevance: Although periodontal splinting can be a useful tool in specific These clinical entities have been
situations, it can be inappropriately applied and may create some technical difficulties in
clinical management. It is therefore important that the clinician is well aware of the potential
described as primary or secondary
hazards involved in carrying out this type of treatment. The importance of careful periodontal occlusal trauma (Table 1).3 Most
monitoring and maintenance following splinting cannot be overstressed, because ongoing commonly, mobility of teeth is caused
disease can be masked and access for hygiene compromised around periodontally involved by loss of support as a result of
teeth. periodontal disease, although it is
important to be aware that more than
one factor may be involved (Figure 1).
Diagnosis and clinical management
D ental splinting involves joining the
crowns of two or more teeth by
more or less rigid means; so that their
indicated that the appliance had been
placed on a living patient and is thus
one of the earliest known dental
should take this into account.
When patients present with
periodontal disease and mobile teeth,
relative movement is restricted and the prostheses, dated at around 2500 BC. efforts should be directed at resolving
forces applied to one of the splinted Tooth transplantation has been the periodontal disease before
teeth are transmitted to the root systems described as early as the ninth century considering occlusal management if the
of all the linked teeth.1 This article will AD, and ligatures of silk, gold and silver teeth are to be preserved. In the absence
concentrate on the use of splints in were used in the tenth and eleventh of periodontal disease the most likely
periodontal disease. centuries by the Spanish physician cause of tooth mobility is primary
Splinting has been used as a form of Albucasis. Splinting loose teeth occlusal trauma and therefore
dental treatment for centuries, and is one remained a popular treatment for periodontal treatment would be
of the earliest known examples of mobility well into the twentieth century, inappropriate. Rare causes of tooth
dentistry: excavations of Egyptian and was used as an integral part of mobility – such as abnormal root
remains at Gizeh in the early 1900s periodontal treatment planning by many morphology, iatrogenically shortened
included a wire ligature around the clinicians.2 roots following apical surgery, excessive
cervical margins of lower left second Splinting is still used in a wide variety loading during orthodontic movement,
and third molar teeth, the roots of the of clinical situations: root resorption or intrabony pathology –
third molar having been resorbed. should not be forgotten.
Calculus around both the teeth and wire q traumatic injuries to teeth; In the past it has been thought that
q TMJ dysfunction; mobility adversely affects periodontal
q prevention of toothwear; destruction and healing. Fleszar, as
Sophie J.Watkins, BDS, FDS (Rest Dent) RCPS,
q permanent post-orthodontic recently as 1980,4 found that decreased
MSc, Senior Registrar in Restorative Dentistry, retention; mobility did in fact improve the
and Kenneth W. Hemmings, BDS, MSc, MRD q pre-restorative treatment response of affected teeth to periodontal
RCS, FDS RCS, Consultant in Restorative (identification of retruded contact therapy. The temptation has been in the
Dentistry, Department of Conservative Dentistry, position, RCP); past to ‘treat’ periodontally involved
Eastman Dental Hospital, London.
q excessive movement or migration teeth by early splinting. However, the
278 Dental Update – July/August 2000
2. P E R I O D O N T I C S
Definition The lesion that develops in the periodontium as a result of excessive occlusal teeth to less mobile teeth by splinting
forces during functional and parafunctional activities. lies in the fact that this results in a more
favourable distribution of the forces
Primary The effect of abnormal occlusal forces on periodontal tissues in the absence of
inflammation. A physiological adaptation of the periodontium results in acting on the teeth concerned, thus
mobility with no periodontal pocketing and radiographically a widened protecting those with reduced
periodontal ligament. periodontal support.
Secondary The effect of occlusal forces on teeth where the periodontium is already Indications for splinting are:
weakened by inflammation, giving rise to more complex breakdown of the
periodontal structures. q drifting;
Table 1. Occlusal trauma.3 q improving comfort and function;
q enhancing periodontal healing.
lack of correlation between mobility or stable jaw relationships with stable Drifting
occlusal trauma and periodontal disease/ simultaneous multiple interocclusal Drifting teeth are a common problem in
healing has been demonstrated by many contacts and smooth excursive patients with periodontally diseased
authors.5-10 It is now widely accepted movements unimpaired by occlusal teeth, and may result from normal forces
that the resolution of inflammation is the interferences’, and is described in detail acting on teeth with compromised
most important factor in the treatment of by Wise.14 It may involve the adjustment periodontal support which can no longer
chronic periodontitis. Although trauma of multiple tooth surfaces to achieve an withstand these forces.15 If the patient is
from occlusion may modify the ‘ideal occlusion’ and is therefore a concerned about appearance following
progression of existing periodontitis,11 it significant undertaking and is not drifting, after the disease has been
does not initiate or aggravate recommended to the inexperienced controlled the teeth can be repositioned
gingivitis.12 Kantor, Polson and Zander13 practitioner. A trial adjustment on study orthodontically. The result is, however,
showed that alveolar bone is regenerated casts may confirm that the procedure is inherently unstable and splinting is
after removal of both inflammation and not excessively destructive of tooth generally advisable to prevent relapse.
traumatic factors. tissue and the aims of the adjustment are Indeed, the position of drifted teeth that
attainable (Figure 2). are not treated orthodontically can be
prevented from worsening by the
CLINICAL MANAGEMENT provision of a splint.
The options for the clinical management Extraction Similarly, adverse tooth movements
of mobile teeth include: It is important to be able to recognize such as over-eruption or tilting can be
whether a tooth is conservable or not prevented by splinting.16 Splinting in
q no treatment; and to consider whether retaining a this situation can be provided by a fixed
q occlusal adjustment; certain tooth may be harmful to or removable prosthesis and, although
q extraction; neighbouring teeth. If this is the case, this may not be the primary function of
q splinting. extraction is the best course of action. the prosthesis, it should be taken into
account whilst designing the appliance.
It is important to stress that, if a fixed
SPLINTING splint or a removable appliance is
No Treatment The scientific basis for joining mobile provided, this may have an adverse
If the clinician considers the situation
unlikely to deteriorate, this option may
be acceptable to many patients. a b
However, regular review is
recommended.
Occlusal Adjustment
If an occlusal aetiological factor has
been positively identified, occlusal
adjustment may be indicated. Localized
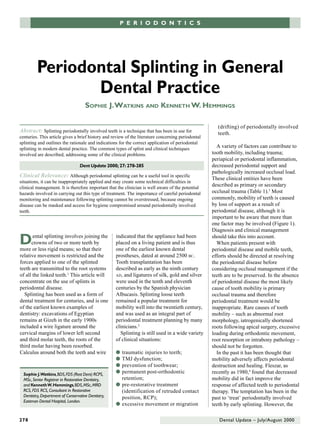
adjustment to a few teeth is relatively Figure 1. Radiographs demonstrating occlusal trauma. (a) Root treated upper first molar
straightforward. Occlusal equilibration bridge abutment presented with distal and furcation pocketing of 6–7 mm. There was also
has been described as ‘planned distal caries. (b) Following root resection the pocketing was reduced to 4 mm, but mobility
alteration of occlusal surfaces to provide increased with widening of the periodontal ligament on the remaining (mesial) root.
Dental Update – July/August 2000 279
3. P E R I O D O N T I C S
but increase accumulation of plaque
a b around the abutment teeth. Fixed splints
may compromise the ability of patients
to use interdental cleaning aids.
Therefore, care must be taken in
designing and making splints with good
physiological contour to allow easy
patient maintenance. Patients need
regular instruction on oral hygiene and
Figure 2. Trial occlusal adjustment on study casts. (a) The casts mounted in the retruded axis encouragement to maintain high levels
position demonstrate a large non-working side interference between /7 and /8 in right lateral of plaque control.
excursion (arrowed). (b) Trial adjustment of the casts. The occlusal surfaces of the casts are
painted before performing the trial adjustment. In this way it is possible to assess the necessary Periodontal Monitoring
removal of tooth tissue, allowing the operator to assess how destructive this would be before
carrying out the procedure clinically. In this case, extensive tooth reduction would be required to Fixed splinting of teeth prevents clinical
eliminate the interference, making it too destructive to carry out clinically without recourse to assessment and reduces patient
crowns or onlays. awareness of increasing tooth mobility.
Occasionally, if patients are lost from
regular review, they may perceive a
problem only when gross periodontal
effect on the patient’s ability to maintain periodontal ligament (rigid splinting of destruction has occurred and the whole
good oral hygiene. Unless excellent root or alveolar fractures is still splint is mobile. These potential
plaque control is maintained, the recommended17). Rarely, mobile teeth complications should be stressed to
periodontal condition may not be stable undergoing periodontal surgery require patients. Effective recall systems should
and could result in breakdown. temporary splinting until initial healing be in place and regular clinical and
Furthermore, a fixed splint may mask is complete. However, questions should radiographic review carried out.
this deterioration: an added danger of be raised concerning the prognosis of
which the operator must be aware. such teeth and the advisability of Dental Caries
Meticulous monitoring and maintenance surgery. The advantages of splinting If plaque control is inadequate in
is therefore essential. have been contested; Renggli et al.18–20 combination with dietary factors, fixed
showed no difference in mobility before or removable splints may encourage
and after wearing a splint. Indeed, many dental caries in a susceptible patient.
Comfort and Function authors have found that increased Cementation failure of fixed splints
Mobile teeth can be very distressing to mobility/occlusal trauma may not be may go unnoticed until gross dental
the patient and may often be the detrimental to the health of the caries is observed. Prevention in the form
presenting complaint. Extreme mobility remaining supporting tissues.19,20 of fluoride supplements, diet counselling
can interfere with speaking and eating. It and regular prophylaxis are therefore
must be stressed that active disease important, as well as regular review with
should be controlled as far as possible Disadvantages of Splinting careful inspection of margins allowing
and the patient capable of maintaining a early maintenance if required.
good standard of oral hygiene before Plaque Control
further treatment is considered. Removable splints allow the patient to Maintenance of Splints
Although a reduction in inflammation practise normal plaque control measures Biological failure of splints is usually
may result in a decrease in mobility to
acceptable levels, in the presence of
severe periodontal involvement this may
not be complete and mobility may still a b
constitute a significant problem. In such
cases, splinting may be the only way of
resolving the situation.
Periodontal Healing
Post-trauma splinting of luxated or
subluxated teeth, allowing some
physiological loading of the teeth, is Figure 3. (a) Deep overbite causing trauma to the labial gingivae of the lower incisors. (b) A
soft splint fitted over the maxillary teeth protects the gingivae.
beneficial to the healing of the
280 Dental Update – July/August 2000
4. P E R I O D O N T I C S
Hard Acrylic Occlusal Splint: Occlusal
a b splints can be useful in the diagnosis of
occlusal trauma in periodontal patients
and for retention of drifting teeth
(Figure 4).
There are many descriptions of
occlusal splints in the literature. The
term covers full coverage, partial
coverage and repositioning appliances,
Figure 4. Hard maxillary occlusal splint. (a) Facial view. (b) Palatal view, showing the occlusal and are used in diagnostic and
scheme adjusted to provide even contacts around the arch in the retruded axis position (black therapeutic procedures as outlined
marks) and anterior guidance with immediate posterior disclusion in excursions (red marks). below:
q TMJ dysfunction;
q prevention of toothwear;
the result of dental caries, progressive progressive drifting despite treatment. q to facilitate restorative procedures
periodontal disease or endodontic In borderline cases, where the by establishing a stable retruded
complications. All restorations have a outcome of treatment cannot be contact position;
finite lifespan and will eventually wear predicted, a provisional splint may be q assessment of patient tolerance to
out unless more significant mechanical provided. an increase in occlusal vertical
failure occurs first. The very nature of Describing appliances as ‘permanent’ dimension;
splinting means that splints are large is a relative term because it must be q stabilization of tooth position.
and expensive prostheses. If prompt remembered that all restorations will fail
attention is not given to a mechanical in time. It is a term that can be Partial-coverage splints are not
failure there is a significant risk of misunderstood by patients and should be recommended for long-term use. There
mobile teeth drifting away from the used with caution. is a significant risk of over-eruption of
splint. Repositioning or replacement of unopposed teeth, which leads to
such teeth will complicate maintenance. Removable Splints disruption of the occlusal plane in one or
A biological and financial cost/benefit The use of removable splints is simple, both arches and is difficult to rectify.
analysis of splinting teeth should be reversible and inexpensive. The We therefore favour a full-coverage
carried out and compared with other splinting of teeth may be less rigid in maxillary hard acrylic occlusal splint
treatment options before confirming the removable splinting than using fixed providing even contacts in the retruded
most appropriate treatment. alternatives, but they have the axis position, and anterior guidance in
advantage of facilitating oral hygiene.19 protrusive and lateral excursions. In
They are usually the most appropriate patients with Angles class III occlusal
Types of Splint splints for use in emergencies and relationship, it is often easier to
Splints used in clinical practice can be diagnostic procedures. construct one for the mandibular arch.
categorized as either removable or fixed. Vacuum-formed Splints: These This type of appliance is more time-
The descriptive terms temporary or appliances are temporary or provisional consuming to construct than the vacuum-
provisional refer to the durability of the in nature. They are most useful in formed acrylic splint as mounted study
appliance or the intended use. reducing the symptoms in traumatic casts are required for laboratory
occlusions when incisal edges of
Temporary/Permanent/Provisional anterior teeth occlude directly on the
Temporary splints can be defined as a gingivae or palate (Figure 3). These
splint intended for short or medium-term splints are also useful in the diagnosis of
use, which may or may not be replaced TMJ dysfunction, when symptoms are
by a permanent appliance. They may be usually alleviated by the use of a splint.
used to stabilize the mobile teeth during In parafunctional patients the splints
surgery. Examples of temporary splints will show early deterioration and will
include acrylic and wire splints21 and often perforate on the occlusal surface.
vacuum-formed splints, which are The splint is usually best tolerated in
described later. the upper arch. The alginate impression
Permanent splints, such as linked is cast in the laboratory and a vacuum-
Figure 5. Removable orthodontic retainer with
restorations, may be used for teeth that formed polythene splint of 2–3 mm in acrylic on the labial bow, adapted to the labial
cannot maintain stability after treatment, thickness is made. Minimal adjustments surfaces of the teeth. This improves control over
or teeth with increasing mobility or are made for patient comfort. the tooth position during the retention phase.
282 Dental Update – July/August 2000
5. P E R I O D O N T I C S
advantageous (Figure 6). A new
a b technique, using flexible ceramic
bonding fibre ribbon or cords such as
GlasSpan or Ribbond (Sigma Dental
Systems, Heideland 22, Germany)
instead of wire to reinforce the
composite resin gives a more aesthetic
and useful alternative (Figure 6). Where
a palatal appliance is provided, it is of
obvious importance to ensure that the
c Figure 6. (a) Twistflex® (Wildcat® Wire bulk of the splint does not interfere with
GAC International Inc. Central Islip, NY inter-occlusal contacts or with guidance.
11722-1402, USA) orthodontic retainer, Resin-Bonded Splints: Laboratory-
passively adapted to the palatal surfaces and fabricated splints may offer a more
bonded to the teeth using composite resin.
long-term solution to the chairside-
(b) GlasSpan® (Exton, PA, USA) flexible
ceramic fibre can be used as an alternative prepared splints described above. They
to wire for reinforcing the composite resin are less bulky and can be placed in most
splint (c) Finished result. situations, allowing greater occlusal
control. Rochette originally described a
perforated resin-bonded splint (Figure
7) in 1973.26 The technique was adapted
construction. The use of a facebow Orthodontic Retainer: Drifted and refined for tooth replacement. The
recording and a semi-adjustable periodontally involved teeth can be basic laboratory and chairside
articulator considerably reduces repositioned orthodontically. Long-term procedures are now commonly used and
chairside adjustment of the splint.3 If retention is necessary to prevent relapse. well known.27–29
this is not possible, the RCP jaw Removable orthodontic retainers (Figure Today, a non-perforated framework
registration must be at the correct 5) can be used in long-term retention, (Figure 8) is recommended for use with
occlusal vertical dimension (2–3 mm but are associated with periodontal modern Bis-GMA (e.g. Panavia 21) or
increase) and adjustment of the splint inflammation unless plaque control is 4-META cements (e.g. Superbond
in excursions will be necessary. exemplary. They are unaesthetic, but C&B ). Retention should be optimized
A well made splint can be retained by may be acceptable for night wear. by providing maximum coverage of the
a friction fit. Additional retention can available enamel, but tooth preparation
be provided by ball-ended clasps or Fixed Splints should be kept to a minimum. Parallel
Adams cribs as direct retainers, usually Composite/Acrylic and Wire: This guide planes also allow accurate
on the first molars. Long-term occlusal temporary or semi-permanent splint is insertion and increase the bonding area
stability of the splint requires several fabricated using a chairside, or direct, by removing undercut areas – and as a
adjustments as mandibular technique. It is reversible, and relatively result can increase retention. Proximal
repositioning occurs. Good service strong, stable and aesthetic. The grooves and parallel walls do involve
would be considered to be 2–3 years of operative technique for making this type extensive tooth preparation (which is
use. In a bruxist patient, more frequent of splint has been widely described21–24 not usually necessary in most situations
replacement will be required as a result and there are many variations. The in the authors’ opinion). In the
of wear or fracture of the acrylic. technique involves adapting a wire, periodontal patient with anterior
mesh or other former to the teeth to be
splinted and covering it with composite
resin etched to the enamel. The wire
may be twisted around the teeth as a
ligature or adapted to the palatal
surfaces of the teeth, as long as it is
passive in order to avoid orthodontic
movement. Rosenberg described a
variation using orthodontic grid material
and acrylic.25 Using composite resin
alone to link the teeth is likely to lead to
early failure at contact points, as the
Figure 7. Perforated resin-bonded splint, as material is brittle.23 A linking wire Figure 8. Resin-retained splint with a non-
described by Rochette.26 provides flexibility and is therefore perforated framework.
Dental Update – July/August 2000 283
6. P E R I O D O N T I C S
for resin-bonded splinting also apply to
a b conventional crown and bridgework. In
addition, it is often difficult to obtain
perfect impressions of multiple tooth
preparations within a single impression.
The use of a pick-up procedure allows
the dies of multiple abutment teeth to
be located on a single working cast,
and allows the opportunity to overcome
Figure 9. (a) Periodontally involved teeth may cause problems during impression taking due to the problems of excessive tooth
their mobility and the large embrasure spaces, which may cause difficulty in removing the mobility if transfer copings (e.g. acrylic
impression. (b) A temporary splint made of pink acrylic resin Triad visible light cure reline bonnets) are linked passively before
material (Dentsply International Inc., York, PA, USA) is adapted to the labial surfaces of the taking a locating impression (Figure
teeth to stabilize them, and soft wax is placed in the embrasure spaces and undercuts to
prevent the impression material engaging deep undercuts. 11).
It is wise to verify the accuracy of the
working casts before committing your
technician to extensive laboratory
localized or generalized recession, it consuming to prepare and therefore work. This can be simply achieved by
can be difficult to mask interproximal costly in chairside and laboratory time. using a bite fork lined with compound
metal connectors. For splint rigidity, it Parallel and non-undercut preparations and refined with temporary cement.
is rarely wise to reduce connector of multiple teeth are demanding and are The indentations created by the teeth
height below 3 mm. Composite resin destructive of tooth tissue, and should correspond to those on the
additions can be used to cover movement of the abutments during working cast (Figure 12).
unsightly metal. cementation can lead to poorly fitting In common with any extensive
Practical points: margins and failure (Figure 10a). restorative dentistry, maintenance is of
Telescopic crowns, or the use of paramount importance. It must be
q Impression taking and cementation copings and a superstructure, can remembered that splinting teeth can
of restorations can be problematic provide a useful alternative (Figure often delay the presentation of
when teeth are mobile. Temporary 10b,c). Maintenance and tooth loss can mechanical and biological failures.
splinting of teeth and the use of a more easily be accommodated than Late diagnosis of dental caries,
low-viscosity impression material with conventional splinting, but cementation failure and further
can be useful in overcoming some aesthetics and periodontal health can periodontal breakdown may result in
of these problems. Composite be compromised due to increased bulk difficult maintenance, if not
resin, acrylic (Figure 9a) or of the superstructure. catastrophic failure. Patients require
impression compound can be The practical points mentioned above effective recall, careful review and
useful temporary splinting
materials.
q Interdental spacing often needs
blocking out with soft wax to a b
prevent impression material
engaging deep undercuts. This
facilitates removal of the
impression, and not the teeth
(Figure 9b)!
q All luting cements perform best in
thin section, thereby increasing the
longevity of the restoration. Great
care must be exercised to ensure c
teeth are held intimately in contact Figure 10. Linked crowns (a) can be
with the splint during cementation. difficult to cement due to independent
movement of the abutment teeth leading to
Splinted Conventional Crown and poor marginal fit and failure. Gold copings
(b) with telescopic crowns (c) facilitate
Bridgework access for maintenance of abutment teeth
Splinted crowns still have a place when splinted crowns are used.
where the teeth are heavily restored.
However, these splints are time-
284 Dental Update – July/August 2000
7. P E R I O D O N T I C S
crown and bridge procedures. Holland: Dental equilibrium between forces acting on a tooth
Center for Postgraduate Courses, 1985; p.25. and the resistance of the supporting tissues).
4. Fleszar TJ, Knowles JW, Morrison EC, Burgett Angle Orthod 1978; 48: 175–186.
FG, Nissle RR, Ramfjord SP. Tooth mobility and 16. Love WD, Adams RL. Tooth movement into
periodontal therapy. J Clin Periodontol 1980; 7: edentulous areas. J Prosthet Dent 1971; 25: 271–
495–505. 278.
5. Ericsson I, Lindhe J. Lack of significance of 17. Andreasen JO, Andreasen FM. Textbook and
increased tooth mobility in experimental Colour Atlas of Traumatic Injuries to the Teeth, 3rd
periodontitis. J Periodontol 1984; 55: 447–452. ed. Copenhagen: Munksgaard, 1994; pp.297, 347–
6. Bhaskar SN, Orban B. Experimental occlusal 348, 439.
trauma. J Periodontol 1955; 26: 270–284 18. Renggli HH. Splinting of teeth – An objective
7. Glickman I. Inflammation and trauma from assessment. Helv Odont Acta 1971; 15: 129.
Figure 11. Acrylic resin Duralay® (Reliance occlusion, co-destructive factors in chronic 19. Renggli HH, Schweizer H. Splinting of teeth with
Dental Mfg. Co., Worth, Illinois, USA) bonnets periodontal disease. J Periodontol 1963; 34: 5– removable bridges. Biological effects. J Clin
are placed over the teeth and passively linked 10. Periodontol 1974; 1: 43–46.
with wire to prevent them from moving relative 8. Glickman I, Smulow JB, Vogel G, Passamoti G. 20. Renggli HH, Allet B, Spanauf AJ. Splinting of teeth
to one another during impression taking. (Slide The effect of occlusal forces on healing with fixed bridges: biological effect. J Oral Rehabil
courtesy of Mr Alex Gow, Specialist Registrar in following mucogingival surgery. J Periodontol 1984; 11: 535–537.
Restorative Dentistry, Eastman Dental Hospital.) 1966; 37: 319–325. 21. Clark JW, Weatherford TW, Mand WV. Wire
9. Lindhe J, Ericsson I. The influence of trauma ligature – Acrylic splint. J Periodontol 1969; 40:
from occlusion on reduced but healthy 371–375.
periodontal tissues in dogs. J Clin Periodontol 22. Klassman B, Zucker HW. Combination wire-
prompt intervention to preserve what 1976; 3: 110–122. composite resin intracoronal splinting: Rationale
remains. 10. Nyman S, Lindhe J. Persistent tooth and technique. J Periodontol 1976; 47(8): 481–486.
hypermobility following completion of 23. Polson AM, Billen J. Temporary splinting using
periodontal treatment. J Clin Periodontol 1976; ultraviolet-light-polymerised bonding materials. J
CONCLUSIONS 3(2): 81–93. Am Dent Assoc 1974; 89: 1137–1141.
11. Nyman S, Lindhe J, Ericsson I. The effect of 24. Saravanamuttu R. Post-orthodontic splinting of
The value of splints in periodontal progressive tooth mobility on destructive periodontally involved teeth. Br J Orthodont 1990;
therapy has been called into question in periodontitis in the dog. J Clin Periodontol 1978; 17: 29–32.
5: 213–225. 25. Rosenberg S. A new method for stabilization of
the last decade, but may be indicated in 12. Svanberg G. Influence of trauma from the periodontally involved teeth. J Periodontol 1980;
some circumstances. It is important to occlusion on the periodontium of dogs with 51: 469–473.
remember that splinting rarely normal or inflamed gingiva. Odont Revy 1974; 25: 26. Rochette AL. Attachment of a splint to enamel
improves periodontal health and may 165–178. of lower anterior teeth. J Prosthet Dent 1973; 30:
13. Kantor M, Polson AM, Zander HA. Alveolar bone 418–423.
serve only to mask a problem. regeneration after removal of inflammation and 27. Simonsen R, Thompson V, Barrack G. Etched Cast
Therefore, the decision to splint teeth traumatic factors. J Periodontol 1976; 47: 687–695. Restorations. Clinical and Laboratory Techniques.
should not be taken lightly and should 14. Wise MD. Occlusal adjustment and equilibration. Chicago: Quintessence, 1983.
be considered only following In: Failure in the Restorative Dentition; Management 28. Tay WM. Classification and assessment of
and Treatment. London: Quintessence, 1995; composite retained bridges. Restor Dent 1986; 2:
appropriate periodontal management, pp.225–235. 15–18.
with thorough maintenance following 15. Proffitt W. Equilibrium theory revisited. Factors 29. Tay WM. Resin bonded bridges. 1. Materials and
splinting. In this context, it is important influencing the position of teeth (i.e. methods. Dent Update 1988; 15: 10–14.
to ensure that the patient is aware of
the potential pitfalls in order to
safeguard compliance with continued
monitoring and maintenance. a b
The indications for splinting are
usually limited to improving patient
comfort and controlling tooth
movement in teeth with periodontal
health but reduced support. Clinical
techniques have been developed to help
the practitioner provide such treatment
or consider referral to a specialist.
c
Figure 12. A facebow bitefork, refined with
REFERENCES Temp Bond® cement (Kerr UK Ltd.,
1. Smith BJ, Setchell D. In: Rowe, AHR, ed. Peterborough, PE3 8YP) (a) is adapted to fit
Companion to Dental Studies Vol.3: Clinical Dentistry. the preparations (b) and used to verify the
Oxford: Blackwell Scientific Publications, 1986; accuracy of the master cast (c).
pp.519–529.
2. Weinberger BW. An Introduction to the History of
Dentistry, Vol.1. St. Louis: C.V. Mosby, 1948; p.75.
3. Pameijer HN. Periodontal and occlusal factors in
Dental Update – July/August 2000 285