

Empfohlen
Weitere ähnliche Inhalte
Was ist angesagt?
Was ist angesagt? (20)
Andere mochten auch
Andere mochten auch (20)
Ähnlich wie gingival curettage
Ähnlich wie gingival curettage (20)
Mehr von Dr.Jaffar Raza BDS
Mehr von Dr.Jaffar Raza BDS (20)
Kürzlich hochgeladen
Kürzlich hochgeladen (20)
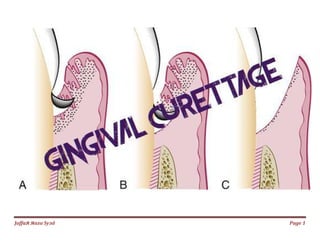
gingival curettage
- 1. Jаffaя яaza Syзd Page 1
- 2. Jаffaя яaza Syзd Page 2 Gingival Curettage scraping of gingival wall of a periodontal pocket to separate diseased soft tissue Scaling refers to removal of deposits from tooth/ root surface Root Planing smoothening the root to remove infected and necrotic tooth surface
- 3. Jаffaя яaza Syзd Page 3 TYPES I. Gingival curettage: Consists of removal of inflamed soft tissue lateral to pocket wall a. Subgingival curettage: It is a procedure that is performed apical to epithelial attachment b. Inadvertent curettage: Curettage that is done unintentionally during scaling and root planing. II. Surgical curettage, III. Chemical curettage, IV. ultrasonic curettage. V. Laser Tx
- 4. Jаffaя яaza Syзd Page 4 INDICATIONS 1. In patients whom extensive surgery is contraindicated owing to systemic disease or psychologic problems. 2. Shallow pocket depths with an adequate width and thickness of gingival tissue. 3. It can be performed as a part of new attachment attempts in moderately deep intrabony pockets located in accessible areas. 4. Curettage can be performed on recall visits as a method of maintenance treatment for areas of recurrent inflammation. 5. In suprabony pockets which do not extend beyond the mucogingival junction.
- 5. Jаffaя яaza Syзd Page 5 CONTRAINDICATIONS 1. Presence of acute infections such as necrotizing ulcerative gingivitis (NUG). 2. Fibrous enlargement of gingiva such as phenytoin hyperplasia. 3. Extension of the base of the pocket apical to the mucogingival junction. 4. If the patient is medically compromised, the benefits versus the risks of the surgical procedure should be carefully weighed before commiting the patient to the procedure. 5. Deep pockets ≥ 5mm 6. Furcation Involvement
- 6. Jаffaя яaza Syзd Page 6 PROCEDURE Curettage can be accomplished as a closed procedure with a sharp curette or as an open procedure with a gingival incision followed by root planing (ENAP). Basic Technique (With Curette)
- 7. Jаffaя яaza Syзd Page 7
- 8. Jаffaя яaza Syзd Page 8
- 9. Jаffaя яaza Syзd Page 9 Excisional New Attachment Procedure (ENAP) Indications 1. Suprabony pockets 2. Adequate keratinized tissue 3. When esthetics are unimportant Contraindictions 1. Pockets exceed mucogingival junction 2. Edematous tissue 3. Lack of keratinized tissue 4. Osseous defects must be treated 5. Hyperplastic tissue 6. Close root proximity 7. Furcation involvement 8. Probing depths of 3 mm or less
- 10. Jаffaя яaza Syзd Page 10 Advantages 1. Improved root visualization 2. Complete removal of sulcular epithelium and epithelial attachment 3. Minimal gingival trauma 4. No loss of keratinized gingiva Disadvantages 1. Difficult to determine apical extent of epithelial attachment 2. Does not result in new attachment
- 11. Jаffaя яaza Syзd Page 11
- 12. Jаffaя яaza Syзd Page 12 Ultrasonic Curettage Sound energy absorbed at tissue junctions that take the form of heat, results in coagulation. The coagulated epithelium is then removed by mechanical action of the vibrations of ultrasonic instrument. Chemical Curettage Sodium sulphide, phenol, camphor, antiformin, and sodium hypochlorite have been used for chemical curettage. Solution applied for 1 minute. Then 5% citric acid solution is introduced into the pocket for 1 minute to neutralize the sodium hypochlorite. The coagulated tissue is then removed with a curette and pocket is flushed with saline to remove the remnants of the connective tissue. The extent of chemical penetration to the tissue cannot be controlled and thus, chemical curettage is discarded.
- 13. Jаffaя яaza Syзd Page 13 Laser CO2 and Nd:YAG laser treatment HEALING AFTER CURETTAGE Gingival sulcus filled by blood clot immediately after curettage. Abundant polymorphonuclear leukocytes occupy the wound site. followed by rapid proliferation of granulation tissue. Epithelium: Sulcular epithelium is restored between 2 to 7 days junctional epithelium: as early as 5 days after curettage. Connective tissue: Immature collagen fibers appear within 21 days.
- 14. Jаffaя яaza Syзd Page 14