Myocardial infarction_ Causes, Symptoms, Diagnosis, Treatment, and Pathology
•
33 gefällt mir•10,982 views

Myocardial infarction_ Causes, Symptoms, Diagnosis, Treatment, and Pathology

Empfohlen
Weitere ähnliche Inhalte
Was ist angesagt?
Was ist angesagt? (20)
Ähnlich wie Myocardial infarction_ Causes, Symptoms, Diagnosis, Treatment, and Pathology
Ähnlich wie Myocardial infarction_ Causes, Symptoms, Diagnosis, Treatment, and Pathology (20)
Mehr von Imhotep Virtual Medical School
Mehr von Imhotep Virtual Medical School (20)
Kürzlich hochgeladen
Kürzlich hochgeladen (20)
Myocardial infarction_ Causes, Symptoms, Diagnosis, Treatment, and Pathology
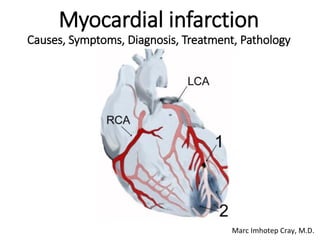
- 1. Myocardial infarction Causes, Symptoms, Diagnosis, Treatment, Pathology Marc Imhotep Cray, M.D.
- 2. Marc Imhotep Cray, M.D.. Topics Outline 2 Scientific foundations Pathology of MI A Clinical & Pathology Correlation Case Clinical Medicine Capsule (Dx & Tx)
- 3. Marc Imhotep Cray, M.D.. Scientific foundations 3
- 4. Marc Imhotep Cray, M.D.. Epidemiology Myocardial infarction is a common presentation of coronary artery disease WHO estimated in 2004, that 12.2% of worldwide deaths were from ischemic heart disease (IHD) leading cause of death in high- or middle-income countries and second only to lower respiratory infections in lower-income countries Worldwide, more than 3 million people have STEMIs and 4 million have NSTEMIs a year STEMIs occur about twice as often in men as women 4
- 5. Marc Imhotep Cray, M.D.. Diagnostic Classifications & Terminology 5 Anatomic (Pathologic) Diagnosis= Atherosclerosis (ASHD) Etiologic Diagnosis= Coronary Heart Disease (CHD, IHD, CAD) Physiologic Diagnosis= Angina Pectoris (Stable vs Unstable vs ACS ), SOB, Atrial fibrillation, MI etc. Functional Diagnosis= New York Heart Association (NYHA) functional classification Heart Failure o Pulmonary Edema/Cardiogenic Shock major acute complication of myocardial infarction (STEMI and NSTEMI )
- 6. Marc Imhotep Cray, M.D.. NYHA Functional Classification HF The classes (I-IV) are: Class I: no limitation is experienced in any activities; there are no symptoms from ordinary activities Class II: slight, mild limitation of activity pt. comfortable at rest or with mild exertion. Class III: marked limitation of any activity pt. comfortable only at rest Class IV: any physical activity brings on discomfort and Sx occur at rest Note: This score documents severity of Sx and can be used to assess response to treatment While its use is widespread, NYHA score is not very reproducible and does not reliably predict walking distance or exercise tolerance on formal testing "Limitations of the New York Heart Association functional classification system and self‐reported walking distances in chronic heart failure". Heart. 93 (4): 476–82. 6
- 7. Marc Imhotep Cray, M.D.. Coronary heart disease (CHD) Defined (Etiologic Dx) 7 Coronary heart disease (CHD) is a condition in which proper circulation of blood and oxygen are not provided to heart and surrounding tissue Result is due to a narrowing of small blood vessels, which normally supply heart with blood and oxygen Coronary heart disease, a type of cardiovascular disease leading cause of death for both men and women in United States
- 8. Marc Imhotep Cray, M.D.. Causes (Anatomic Dx) 8 Cause of CHD atherosclerosis, which takes place with plaque and fatty build up on artery walls narrowing vessels
- 9. Marc Imhotep Cray, M.D.. Arteriosclerosis 9 Arteriosclerosis is a general term for several disorders that cause thickening and loss of elasticity in arterial wall Atherosclerosis, the most common form, is also the most serious b/c it causes coronary artery disease and cerebrovascular disease Atherosclerosis is patchy intimal plaques (atheromas) in medium- sized and large arteries plaques contain lipids, inflammatory cells, smooth muscle cells, and connective tissue Atherosclerotic narrowing, microscopic Normal coronary artery, microscopic From: Webpath Cardiovascular Pathology image plates
- 10. Marc Imhotep Cray, M.D.. Pathobiology of Atherosclerosis 10 When excess cholesterol deposits on cells and on inside walls of blood vessels it forms an atherosclerotic plaque First step of atherosclerosis is injury to endothelium (See slide # 5) which results in atherosclerotic lesion formation When plaque ruptures blood clots form which lead to ↓ blood flow, resulting in cardiovascular events (ACS) Coronary artery, severe atherosclerosis, gross Coronary artery, mild atherosclerosis, gross From: Webpath Cardiovascular Pathology image plates
- 11. Marc Imhotep Cray, M.D.. Pathobiology of Atherosclerosis cont’d. 11 Symptoms develop when growth or rupture of plaque reduces or obstructs blood flow Diagnosis is clinical and confirmed by angiography, ultrasonography, or other imaging tests Treatment includes risk factor and dietary , modification, physical activity, antiplatelet drugs, and antiatherogenic drugs Image plate description: Heart and LAD coronary artery with recent thrombus, gross Anterior surface of heart demonstrates an opened left anterior descending coronary artery Within lumen of coronary can be seen a dark red recent coronary thrombosis Dull red color to myocardium as seen below glistening epicardium to lower right of thrombus is consistent with underlying MI From: Webpath Cardiovascular Pathology image plates
- 12. Marc Imhotep Cray, M.D.. Risk Factors for Atherosclerosis 12 Risk factors atherosclerosis include: Dyslipidemia (hypercholesterolemia/LDL-C) diabetes cigarette smoking family history sedentary lifestyle obesity hypertension
- 13. Marc Imhotep Cray, M.D.. CAD Risk Factors 13 1. Age (particularly 40+) 2. Diabetes 3. Genetics (heredity) 4. High blood pressure 5. High bad cholesterol (LDL) 6. Increased levels of C- reactive protein, fibrinogen, or homocysteine 7. Lack of sufficient physical activity 8. Low good cholesterol (HDL) 9. Menopause 10. Obesity 11. Smoking Certain conditions are considered to put an individual at greater risk for coronary heart disease Following are some risk factors: (same as for atherosclerosis in general)
- 14. Marc Imhotep Cray, M.D.. Symptoms OF CHD 14 Some more frequent symptoms of coronary heart disease include: 1. Angina (ischemic pain) 2. Myocardial Infarction 3. Shortness of breath 4. Atrial fibrillation
- 15. Marc Imhotep Cray, M.D.. Diagnosis 15 Diagnosis of CHD may be accomplished by a variety of means: 1. Coronary angiography 2. Coronary arteriography 3. Coronary CT angiography 4. Echocardiogram 5. Electrocardiogram (ECG) 6. Electron-beam CT (EBCT) 7. Exercise stress test 8. Magnetic resonance angiography 9. Nuclear scan
- 16. Marc Imhotep Cray, M.D.. Remember: A MI occurs when an atherosclerotic plaque slowly builds up in inner lining of a coronary artery and then suddenly ruptures, causing catastrophic thrombus formation, totally occluding artery and preventing blood flow downstream. 16 Online version
- 17. Marc Imhotep Cray, M.D.. Areas where pain is experienced in myocardial infarction, showing common (dark red) and less common (light red) areas on the chest and back. 17
- 18. Marc Imhotep Cray, M.D.. Criteria for Diagnosis of acute myocardial infarction (AMI) Criteria An AMI, according to current consensus, is defined by an elevated cardiac biomarker and at least one of the following: Symptoms relating to ischemia Changes on an electrocardiogram (ECG), such as ST segment changes, new left bundle branch block, or Q waves Changes in motion of heart wall on imaging Demonstration of a thrombus on angiogram or at autopsy 18
- 19. Marc Imhotep Cray, M.D.. Types (classification) of MI Types MIs are generally clinically classified into ST elevation MI (STEMI) and non-ST elevation MI (NSTEMI) These are based on changes to an ECG STEMIs make up about 25 - 40% of MIs 19
- 20. Marc Imhotep Cray, M.D.. Types (classification) of MI cont’d. A more explicit classification system, based on international consensus in 2012, also exists classifies MIs into five types: 1. Spontaneous MI related to plaque erosion and/or rupture, fissuring, or dissection 2. MI related to ischemia, such as from increased oxygen demand or decreased supply, e.g. coronary artery spasm, coronary embolism, anemia, arrhythmias, high blood pressure or low blood pressure 20
- 21. Marc Imhotep Cray, M.D.. Types (classification) of MI cont’d. 3. Sudden unexpected cardiac death, including cardiac arrest, where symptoms may suggest MI, an ECG may be taken with suggestive changes, or a blood clot is found in a coronary artery by angiography and/or at autopsy but where blood samples could not be obtained, or at a time before the appearance of cardiac biomarkers in the blood 4. Associated w coronary angioplasty or stents Assoc. w percutaneous coronary intervention (PCI) Assoc. w stent thrombosis as documented by angiography or at autopsy 5. Associated w CABG 21
- 22. Marc Imhotep Cray, M.D.. Diagnosis of MI cont’d.: Cardiac biomarkers There are a number of different biomarkers used to determine presence of cardiac muscle damage Troponins (bld), are considered best, and preferred b/c they have greater sensitivity and specificity for measuring injury to heart muscle than other tests A rise in troponin occurs within 2–3 hours of injury to heart muscle, and peaks within 1–2 days o Gross value, as well as a change over time, useful in measuring and diagnosing or excluding MI o One high-sensitivity cardiac troponin is able to rule out MI as long as ECG is normal 22
- 23. Marc Imhotep Cray, M.D.. Diagnosis of MI cont’d.: ECGs Electrocardiograms (ECGs) are a series of leads placed on a person's chest that measure electrical activity assoc. w contraction of heart muscle Taking of an ECG is an important part in workup of an AMI, and ECGs are often not just taken once, but may be repeated over minutes to hours, or in response to changes in Sn or Sx In addition to a rise in biomarkers, a rise in ST segment, changes in shape or flipping of T waves, new Q waves, or a new LBBB can be used to Dx an AMI 23
- 24. Marc Imhotep Cray, M.D.. ECG cont’d. In addition, ST elevation can be used to Dx an ST segment myocardial infarction (STEMI) A rise must be new, in two adjacent ECG leads [greater than 2 mm (0.2 mV) for males] and [greater than 1.5 mm (0.15 mV) in females ] in all leads except for V2 and V3, where it must be greater than 1 mm (0.1 mV) ST elevation is assoc. w infarction, and may be preceded by changes indicating ischemia such as ST depression or inversion of T waves Abnormalities can help localize location of an infarct, based on leads that are affected by changes Early STEMIs may be preceded by peaked T waves Other ECG abnormalities relating to complications of AMI may also be evident such as atrial or ventricular fibrillation 24
- 25. Marc Imhotep Cray, M.D.. A 12-lead ECG showing a STEMI Elevation of ST segment can be seen in some leads(II, III, aVF) 25
- 26. Marc Imhotep Cray, M.D.. Poor movement of heart due to an MI as seen on ultrasound 26 Online version
- 27. Marc Imhotep Cray, M.D.. Pulmonary edema due to an MI as seen on ultrasound 27 Online Version
- 28. Marc Imhotep Cray, M.D.. Differential diagnosis There are many causes of chest pain, which can originate from the heart, lungs, gastrointestinal tract, aorta, and other muscles, bones and nerves surrounding the chest In addition to MI, other causes of CP include Angina, insufficient blood supply (ischemia) to the heart muscles without evidence of cell death Gastroesophageal reflux disease (GERD) Pulmonary embolism (PE) Tumors of the lungs Pneumonia Rib fracture Costochondritis and other musculoskeletal injuries 28
- 29. Marc Imhotep Cray, M.D.. DDx cont’d. Rarer severe DDx includes Aortic dissection Esophageal rupture Tension pneumothorax, and Pericardial effusion causing cardiac tamponade Chest pain in an MI may mimic heartburn Causes of sudden-onset breathlessness generally involve lungs or heart, including Pulmonary edema Pneumonia Allergic reactions and asthma, and Pulmonary embolus, acute respiratory distress syndrome (ARDS) and metabolic acidosis 29
- 30. Marc Imhotep Cray, M.D.. Treatment 30 Coronary heart disease treatment methods may include: (depends on presenting Physiologic Dx) 1. Angioplasty with stenting 2. Coronary artery bypass surgery (CABG) 3. Medication (Thrombolytic agents) 4. Minimally invasive heart surgery 5. Proper diet and exercise 6. Quitting smoking 7. Treatment of other comorbidities, HTN, DM, Obesity
- 31. Marc Imhotep Cray, M.D.. 31 Myocardial Infarction Pathology Drawing of heart showing anterior left ventricle wall infarction
- 32. Marc Imhotep Cray, M.D.. Heart, left ventricle, acute myocardial infarction, gross 32 • This is left ventricular wall which has been sectioned lengthwise to reveal a large recent MI • Center of infarct contains necrotic muscle that appears yellow-tan • Surrounding this is a zone of red hyperemia • Remaining viable myocardium is reddish- brown Webpath Cardiovascular Pathology image plates
- 33. Marc Imhotep Cray, M.D.. Heart, left ventricle and septum, MI, gross 33 • This cross section through heart demonstrates LV on left • Extending from anterior portion & into septum is a large recent MI • Center is tan with surrounding hyperemia • Infarction is "transmural" in that it extends through full thickness of wall Webpath Cardiovascular Pathology image plates
- 34. Marc Imhotep Cray, M.D.. Heart, transmural MI with rupture and hemopericardium, gross 34 One complication of a transmural MI is rupture of myocardium • most likely to occur in first week between 3 to 5 days following initial event, when myocardium is softest White arrow marks point of rupture in this anterior-inferior MI of left ventricular free wall and septum Note dark red blood clot forming hemopericardium • hemopericardium can lead to tamponade Webpath Cardiovascular Pathology image plates
- 35. Marc Imhotep Cray, M.D.. Heart, left ventricular aneurysm, gross 35 A cross section through heart reveals a ventricular aneurysm with a very thin wall at arrow • Note how aneurysm bulges out • Stasis in this aneurysm allows mural thrombus, which is present here, to form within aneurysm Webpath Cardiovascular Pathology image plates
- 36. Marc Imhotep Cray, M.D.. Putting it All Together_ A Clinical & Pathology Correlation Case (Read: MI Case Scenario with annotations. pdf) Source: Stevens A, Lowe J, Scott I. Core Pathology, 3rd Ed. St. Louis: Mosby-Elsevier, 2009; 1-3. A. History of chest pain which improved on rest must mean that coronary arteries are severely narrowed by atheroma, causing partial blockage of lumen. Diagnosis A Diagnostic process requires an understanding of pathology Reduction in blood supply to heart muscle will have produced symptoms of chest pain only on exertion, when heart is working hard and has high blood and oxygen requirements. It is characteristic that this type of pain (angina of effort) disappears on resting. Relevant pathology A 36
- 37. Marc Imhotep Cray, M.D.. Clinical & Pathology Correlation Case cont’d. B. The constant chest pain must mean that pt. now has a true MI, and that coronary artery is completely blocked, perhaps by a thrombus. Relevant pathology B Diagnosis B There will now be an area of dead heart muscle in wall of left ventricle, and patient's life is at risk. Thoughts in doctor’s mind “I must look out for symptoms and signs of immediate complications of MI. It will take about 8 weeks for infarcted heart muscle to heal by scarring; until then he is at risk.” 37
- 38. Marc Imhotep Cray, M.D.. Clinical & Pathology Correlation Case cont’d. C. This patient's immediate complications are failure of left ventricle, leading to reduced cardiac output (responsible for his cold, clammy skin and his low blood pressure). Also, his damaged left ventricle is unable to empty completely at systole, so there will be increased back pressure in the left atrium and pulmonary veins and capillaries. Fluid will pass from pulmonary capillary blood into his alveoli, making him very breathless (pulmonary edema). The breathlessness and shock must mean that the patient has a failing left ventricle. Thoughts in doctor’s mind “I had better begin treatment immediately to improve output and strength of damaged left ventricular muscle. I will give him strong analgesia for pain and distress, and consider thrombolysis therapy to break down thrombus occluding his coronary artery.” Diagnosis BRelevant pathology C 38
- 39. Marc Imhotep Cray, M.D.. Clinical Medicine Capsule (Dx & Tx) 39
- 40. Marc Imhotep Cray, M.D.. Acute Coronary Syndromes (ACS) ACS is a spectrum of clinical syndromes caused by plaque disruption or vasospasm leads to acute myocardial ischemia Unstable angina (UA) is defined as chest pain that is (1) new onset, is (2) accelerating (ie, occurs with less exertion, lasts longer, or is less responsive to medications), or (3) occurs at rest distinguished from stable angina pectoris by patient history UA signals presence of possible impending infarction based on plaque instability In contrast, NSTEMI indicates myocardial necrosis marked by elevations in troponin I and creatine kinase–MB isoenzyme (CK-MB) without ST-segment elevations seen on ECG 40
- 41. Marc Imhotep Cray, M.D.. ACS: UA vs NSTEMI cont’d. 41 Diagnosis Patients should be risk stratified according to Thrombolysis in Myocardial Infarction (TIMI) study criteria UA is not assoc. w elevated cardiac markers, but ST changes may be seen on ECG NSTEMI is Dx by serial cardiac enzymes and ECG
- 42. Marc Imhotep Cray, M.D.. Thrombolysis in Myocardial Infarction (TIMI) Risk Score for UA/NSTEMI 42 Characteristics Point History Age ≥ 65 years Three or more CAD risk factors (premature family history, DM, smoking, HTN, ↑ cholesterol) Known CAD (stenosis > 50%) ASA use in past 7 days Presentation Severe angina (2 or more episodes within 24 hours) ST deviation ≥ 0.5 mm + cardiac marker Risk score—total points* (0–7) 1 1 1 1 1 1 1 *Patients at higher risk (risk score ≥ 3) benefit more from enoxaparin (vs unfractionated heparin), glycoprotein IIb/IIIa inhibitors, and early angiography. Le T, Bhushan V, Vincent L. Chen VL, King MR. First Aid for the USMLE Step 2 CK ,9th Ed. New York, NY: McGraw-Hill Education, 2016.
- 43. Marc Imhotep Cray, M.D.. ACS: UA vs NSTEMI cont’d. 43 Treatment Treat acute symptoms with ASA, O2, IV nitroglycerin, and IV morphine, and consider β-blockers as hemodynamics allow Admit to hospital, and monitor until acute MI has been ruled out by serial cardiac enzymes Pts. w CP refractory to medical therapy, a TIMI score of ≥ 3, a troponin elevation, or ST changes > 1 mm should be given IV heparin and scheduled for angiography and possible revascularization (percutaneous coronary intervention [PCI] or coronary artery bypass graft [CABG]) MNEMONIC: When your patient is MOANing from an MI, remember— MOAN Morphine Oxygen (to maintain saturations) ASA Nitrogen
- 44. Marc Imhotep Cray, M.D.. ST-Elevation Myocardial Infarction (STEMI) 44 STEMI=ST-segment elevations and cardiac enzyme release 2° to prolonged cardiac ischemia and necrosis History/Physical examination Presentation: Acute-onset substernal chest pain, commonly described as a pressure or tightness that can radiate to left arm, neck, or jaw Assoc. Sx: Diaphoresis, SOB, lightheadedness, anxiety, N/V, and syncope PE: May reveal arrhythmias, hypotension (cardiogenic shock), and evidence of new CHF NB: The best predictor of survival is left ventricular ejection fraction (EF)
- 45. Marc Imhotep Cray, M.D.. STEMI cont’d. 45 Diagnosis ECG will show ST-segment elevations or new LBBB o ST-segment depressions and dominant R waves in leads V1–V2 can also be reciprocal change indicating posterior wall infarct Sequence of ECG changes: Peaked T waves →ST-segment elevation →Q waves →T-wave inversion→ ST-segment normalization →T-wave normalization over several hours to days Cardiac enzymes: o Troponin I is most sensitive and specific cardiac enzyme o CK-MB and CK-MB/total CK ratio (CK index) are also regularly checked o Both troponin I and CK-MB can take up to 6 hours to rise following onset of chest pain
- 46. Marc Imhotep Cray, M.D.. Typical pattern of serum marker elevation after an acute MI CK-MB = creatine kinase, MB isoenzyme; cTnI = cardiac troponin I; cTnT = cardiac troponin T; LD1 = lactate dehydrogenase isoenzyme 1; MLC = myosin light chain. 46 Tintinalli JE et al. Tintinalli’s Emergency Medicine: A Comprehensive Study Guide, 6th ed. New York, NY: McGraw-Hill; 2004.)
- 47. Marc Imhotep Cray, M.D.. ST-segment abnormalities 47 Inferior MI (involving the RCA/PDA): ST-segment elevation in leads II, III, and aVF Obtain a right-sided ECG to look for ST elevations in right ventricle Anterior MI (involving LAD and diagonal branches): ST-segment elevation in leads V1–V4 Lateral MI (involving LCA): ST-segment elevation in leads I, aVL, and V5–V6 Posterior MI: ST-segment depression in leads V1–V2 (anterior leads) can be indicative Obtain posterior ECG leads V7–V9 to assess for ST segment elevations
- 48. Marc Imhotep Cray, M.D.. Inferior wall myocardial infarction. In this patient with acute chest pain, ECG demonstrated acute ST-segment elevation in leads II, III, and aVF with reciprocal ST-segment depression and T-wave flattening in leads I, aVL, and V4–V6 48 Le T, Bhushan V, Vincent L. Chen VL, King MR. First Aid for the USMLE Step 2 CK ,9th Ed. New York, NY: McGraw-Hill Education, 2016.
- 49. Marc Imhotep Cray, M.D.. Anterior wall myocardial infarction. This patient presented with acute chest pain. The ECG showed acute ST-segment elevation in leads aVL and V1–V6, and hyperacute T waves. 49 Le T, Bhushan V, Vincent L. Chen VL, King MR. First Aid for the USMLE Step 2 CK ,9th Ed. New York, NY: McGraw-Hill Education, 2016.
- 50. Marc Imhotep Cray, M.D.. STEMI Treatment 50 Initial treatment: Key medications: ASA, β-blockers, clopidogrel, morphine, nitrates, and O2 If pt. is in heart failure or in cardiogenic shock, do not give β-blockers instead, give ACEIs provided that pt. is not hypotensive In inferior wall MI avoid nitrates due to risk of severe hypotension
- 51. Marc Imhotep Cray, M.D.. STEMI Treatment cont’d. 51 Interventions: Emergent angiography and PCI should be performed if possible o If PCI cannot be performed within 90 minutes, and there are no contraindications to thrombolysis (eg, a history of hemorrhagic stroke or recent ischemic stroke, severe heart failure, or cardiogenic shock), and patient presents within 3 hours of chest pain onset, thrombolysis with tPA, reteplase, or streptokinase should be performed instead of PCI Long-term treatment includes ASA, ACEIs, β-blockers, high- dose statins (goal LDL < 100 mg/dL), and clopidogrel (if PCI was performed) Modify risk factors with dietary changes, exercise, and tobacco cessation
- 52. Marc Imhotep Cray, M.D.. Complications 52 Arrhythmia is most common complication and most common cause of death following acute MI Less common complications include reinfarction, left ventricular wall rupture, VSD, pericarditis, papillary muscle rupture (with mitral regurgitation), left ventricular aneurysm or pseudoaneurysm, and mural thrombi A timeline of common post-MI complications: o First day: Heart failure o 2–4 days: Arrhythmia, pericarditis o 5–10 days: Left ventricular wall rupture (acute pericardial tamponade causing electrical alternans, pulseless electrical activity), papillary muscle rupture (severe mitral regurgitation) o Weeks to months: Ventricular aneurysm (CHF, arrhythmia, persistent ST- segment elevation, mitral regurgitation, thrombus formation) Dressler syndrome, an autoimmune process occurring 2–10 weeks post-MI, presents with fever, pericarditis, pleural effusion, leukocytosis, and ↑ ESR
- 53. Marc Imhotep Cray, M.D.. See next slide for links to tools and resources for further study. THE END 53
- 54. Marc Imhotep Cray, M.D.. Further study Putting it All Together_ A Clinical & Pathology Correlation Case .pdf Downloads Autonomic and Cardiovascular Pharmacology (ACVP) Clinical Correlate Articles. pdf_from e-Medicine 54