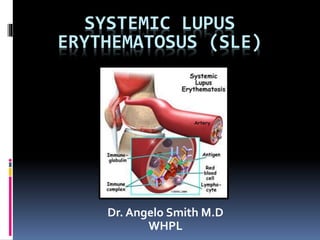
Systemic lupus erythematosus (SLE) is an autoimmune disease that can affect multiple organ systems. It is more prevalent in women and African Americans. Common initial symptoms include fatigue, fever, and weight loss. SLE can cause skin rashes, arthritis, serositis, renal disease, and neurological or hematological abnormalities. Treatment involves managing symptoms with NSAIDs, antimalarials, corticosteroids, and immunosuppressive drugs. Prognosis depends on organ involvement, with renal disease and CNS involvement carrying the worst outcomes.
2. Autoimmune disease that affects
multisystems
1.5 million cases of lupus
Prevalence of 17 to 48 per 100,000
population
Women > Men - 9:1 ratio
90% cases are women
African Americans >Whites
Onset usually between ages of 15 and
45 years, but
Can occur in childhood or later in life
3. Clinical Manifestations
Ranges from a relatively mild
disorder to rapidly progressing,
affecting many body systems.
Chronic with relapsing and remitting
course.
Most commonly affects the skin /
muscles, lining of lungs, heart,
nervous tissue, and kidneys
4.
5. Etiology
Etiology is unknown
Most probable causes
Genetic influence
Hormones
Environmental factors
Certain medications
15. General symptoms
The most common symptoms listed as
initial complaints are fatigue, fever, and
weight loss.
Fever: fever secondary to active disease
was recorded from 50% to 86%. No fever
curve or pattern is characteristic. It can be
difficult, but very important to distinguish
the fever of SLE from that caused by
complicating infections.
16. Clinical Manifestations
Infection
Increased susceptibility to
infections
Fever should be considered
serious
Infections such as pneumonia
are a common cause of death
17. Fatigue is common in patients
with SLE, especially during
periods of disease activity. It is
also often the only symptom that
remains after treatment of acute
flares.
Low grade fever, anemia, or any
source of inflammation can result
in fatigue.
28. Raynaud’s phenomenon is commonly found in
lupus. It lack specificity.
(a triphasic reaction of distal digits to cold or emotion, in
which the skin colour changes from white to blue to red)
34. Pulmonary manifestations
Pleurisy
it is the most common manifestation of
pulmonary involvement of SLE. The volume
of pleural effusions usually is small to
moderate and maybe unilateral or bilateral.
Large pleural effusion are uncommon. It
usually exudative in character.
Pleural effusions may also occur in SLE patients
with nephrotic syndrome, infection, cardiac failure.
35. Lung
1) acute lupus pneumonitis: fever, dyspnea,
cough with scanty sputum, hemoptysis,
tachypnea and pleuritic chest pain.
2) pulmonary hemorrhage
3) chronic diffuse interstitial lung disease.
the diagnosis should not be made until
infectious processes such as viral pneumonia,
tuberculosis, and other bacterial, fungal and
pneumocystis carinii infection have been
completely excluded.
36. Cardiovascular manifestations
Pericarditis is the most common cardiac
manifestation of SLE.
Myocarditis (the clinical features of lupus
myocarditis resembles that of viral
myocarditis)
Libman-Sacks endocarditis and valvular
disease
Hypertension, cardiac failure
37. SLE can be associated
with endocarditis.
Shown here is
Libman-Sacks
endocarditis in which
there are many flat,
reddish-tan
vegetations spreading
over the mitral valve
and chordae.
38. Clinical Manifestations
Renal
Lupus nephritis
Ranging from mild proteinuria
to glomerulonephritis
Primary goal in treatment is
slowing the progression
41. Lupus nephritis
Class I Minimal mesangial Normal light microscopy; abnormal
electron microscopy
Class II Mesangial
proliferative
Hypercellular on light microscopy
Class III Focal proliferative <50% glomeruli involved
Class IV Diffuse proliferative >50% glomeruli involved;
segmental/global
Class V Membranous Predominantly nephrotic disease
Class VI Advanced sclerosing Chronic lesions and sclerosis
42.
43. Clinical Manifestations
Nervous system
Generalized/focal seizures
Peripheral neuropathy
Cognitive dysfunction
Disorientation
Memory and reasoning deficits
Psychiatric symptoms – severe
depression / psychosis
44.
45. Clinical Manifestations
Red blood cells
a normochromic, normocytic anemia is
frequently found in SLE. They appears to be
related to chronic inflammation, drug-related
haemorrhage.
haemolytic anemia as detected by the Coombs’
test is the feature of SLE.
on rare occasion, a serum antibody may be
produced which impairs red cell production.
47. White blood cell
leucopenia (<4.0*109/L), its cause is probably
a combination of destruction of white cells
by autoantibodies, decreased marrow
production, increased or marginal splenic
pooling, and complement activation.
it should also noted that the
immunosuppressive drugs used in the
treatment of SLE may cause a marked
leucopenia.
48. Gastrointestinal and hepatic
manifestation
Esophagitis, dysphagia, nausea,
vomiting: (drug related in most cases)
Chronic intestinal pseudo-obstruction,
mesenteric vasculitis, protein-losing
enteropathy
Pancreatitis
Lupus hepatitis
49. Diagnostic Studies
No specific test
SLE is diagnosed primarily on
criteria relating to
patient history,
physical examination, and
laboratory findings
51. Diagnostic Studies
Antinuclear antibodies
ANA and other antibodies indicate
autoimmune disease
Anti-DNA and anti-Smith antibody tests most
specific for SLE
LE prep can be positive with other rheumatoid
diseases
ESR & CRP are indicative of inflammatory
activity
52. Radiological studies
Joint x-rays: no erosions, periarticular osteopenia
+ soft tissue swelling
CXR/CT chest: interstitial lung disease,
pneumonitis, pulmonary emboli, alveolar
hemorrhage
CTBrain or Brain MRI ± angiography: lupus white
matter changes, vasculitis or stroke
Echo: pericardial effusion, pulmonary
hypertension or Libman-Sacks endocarditis
53. Additional work-up
- Serum cr. and albumin
- CBC w/ diff
- U/A
- ESR
- Complement levels
- Renal profile if warranted
58. Treatment
Treatment plans are based on patient age, sex,
health, symptoms, and lifestyle and on disease
severity
Fever, skin, musculoskeletal and serositis = milder
disease
CNS and renal involvement – aggressive Rx
Goals of treatment are to:
-prevent flares
-treat flares when they occur
-minimize organ damage and complications
59. Collaborative Care
Drug therapy
NSAIDs
Antimalarial drugs
Steroid-sparing drugs
Corticosteroids
Immunosuppressive drugs
60. Conservative management
For those w/out major organ involvement.
NSAIDs: to control pain, swelling, and fever
Caution w/ NSAIDS though. SLE pts are at
increased risk for aseptic meningitis
Antimalarials: Generally to treat fatigue joint
pain, skin rashes, and inflammation of the
lungs
Commonly used: Hydroxycholorquine
Used alone or in combination with other
drugs
61. Corticosteroids (Mainstay of SLE
treatment)
To rapidly suppress inflammation
Usually start with high-dose IV pulse
and convert to PO steroids with goal of
tapering and converting to something
else.
Commonly used: prednisone,
hydrocortisone, methylprednisolone,
and dexamethasone
62. Immunosuppressives
Primarily for CNS/renal involvement
Mycophenolate mofetil (cellcept)
Azathioprine (imuran): requires several months
to be effective, effective in smaller percentage of
patients
MTX: for treatment of dermatitis and arthritis,
not life-threatening disease
Cyclosporine: used in steroid-resistant SLE, risk
of nephrotoxicity
Cyclophosphamide (cytoxan) Almost all trials
performed on patients with nephritis
63. Differential diagnosis
Drug induced lupus erythematosis
Vasculitis
Leukemia
HIV
Multiple sclerosis
Parvovirus or other viral infections
64.
65. Prognosis
Benign to rapidly progressive
Better for isolated skin + musculoskeletal disease vs renal
and CNS
Death rate 3X age-comparable general population
Mortality
Nephritis (most within 5 yrs of symptoms)
Infectious (active SLE + Rx – most common)
CVS disease (50X more MI than other woman)
Malignancy (chronic inflammation + Rx)