Hpv virus infections and oropharynx cancer
•Als PPTX, PDF herunterladen•
19 gefällt mir•25,185 views

Understanding the recent epidemic of HPV related oropharynx cancer

Empfohlen
Weitere ähnliche Inhalte
Was ist angesagt?
Was ist angesagt? (20)
Ähnlich wie Hpv virus infections and oropharynx cancer
Ähnlich wie Hpv virus infections and oropharynx cancer (20)
Mehr von Robert J Miller MD
Mehr von Robert J Miller MD (20)
Kürzlich hochgeladen
Kürzlich hochgeladen (20)
Hpv virus infections and oropharynx cancer
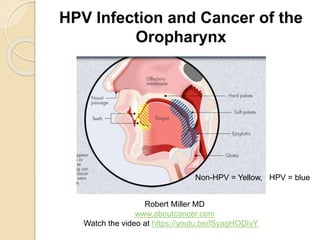
- 1. HPV Infection and Cancer of the Oropharynx Non-HPV = Yellow, HPV = blue Robert Miller MD www.aboutcancer.com Watch the video at https://youtu.be/ISyagHODIvY
- 2. HPV = Human Papillomavirus Most HPV infections don't lead to cancer but certain types of HPV infection cause cancers. More than 100 varieties of human papillomavirus (HPV) exist. HPV is a very common virus; nearly 80 million people—about one in four—are currently infected in the United States.
- 3. Dramatic Rise in HPV + Tonsil Cancer HPV Most Common Smoking Less Common
- 4. Human Papillomavirus and Rising Oropharyngeal Cancer Incidence in the United States JCO November 10, 2011 vol. 29 no. 32 4294-4301
- 5. Cancers caused by HPV • Cervix 100% • Anal 95% • Oropharynx 70% • Vaginal 65% • Vulva 50% • Penis 5% In the US , 3% of all cancers in women and 2% of all cancers in men
- 6. Estimated average annual percentage and estimated number of cancers attributable to human papillomavirus (HPV),* by anatomic site and sex — United States, 2008–2012 MMWR Weekly / July 8, 2016 / 65(26);661–666
- 7. Vaccine to Prevent HPV Since mid-2006, a licensed human papillomavirus (HPV) vaccine has been available and recommended CDC analyzed data from the 2007–2013 National Immunization Survey- Teen (NIS-Teen) and national post licensure vaccine safety data among females and males. Vaccination coverage with ≥1 dose of any HPV vaccine increased significantly from 53.8% (2012) to 57.3% (2013) among adolescent girls and from 20.8% (2012) to 34.6% (2013) among adolescent boys. MMWR July 25, 2014 / 63(29);620-4
- 9. Human papillomavirus (HPV) vaccines. Administer a 3-dose series of HPV vaccine on a schedule of 0, 1-2, and 6 months to all adolescents aged 11 through 12 years. The vaccine series may be started at age 9 years, Catch-up vaccination: Administer the at age 13 through 18 years if not previously vaccinated. Use recommended routine dosing intervals (see above) for vaccine series catch-up.
- 10. HPV Types
- 11. HPV Prevalence In the general population, the overall prevalence of HPV DNA in oral exfoliated cells was 6.9 percent, and the prevalence of HPV-16 was 1 percent. HPV prevalence was approximately three-fold more common in men compared with women (10.1 versus 3.6 percent) presence of HPV in patients with HPV associated oropharyngeal cancer and their long-term sexual partners. In the 164 patients with oropharyngeal cancer, oral HPV was detected in 65 percent of cases, and an oncogenic HPV strain was identified in 61 percent Among the 93 partners available for testing, the overall incidence of HPV infection was 4 percent, and only one had the oncogenic HPV-16. These findings suggest that most partners effectively clear any active infection to which they are exposed.
- 12. HPV + By Cancer Site Oropharynx Cancer 40.6% , 22.4% Oral Cavity Cancer 14.9%, 4.4% Larynx Cancer 13.4%, 3.5% Oropharynx = tonsil, base of tongue, pharyngeal wall, soft palate Oral Cavity = buccal mucosa, floor mouth, anterior tongue, hard palate studies from the 1990s suggested that approximately 50 percent of oropharyngeal cancers were attributable to HPV, while more recent studies suggest that HPV accounts for 70 to 80 percent of cases in North America and Europe
- 14. Oropharynx (base of tongue or tonsil)
- 15. How HPV causes cancer Human papillomavirus (HPV) is a small deoxyribonucleic acid (DNA) virus of approximately 7900 base pairs. Of the genes contained in the virus are viral oncogenes E6 and E7 which have transforming properties by their interaction with growth-regulating host cell proteins E6 interferes with the p53 protein that normally regulates growth, and E7 interferes with Rb protein which also normally regulates growth. When Rb protein is knocked out, another regulatory protein (p16) is overexpressed (i.e. increased)
- 16. Using P16 or HPV Either HPV status or p16 status can be used as a marker of HPV infection. In one multi-institutional trial Ten percent of those positive by p16 were negative for HPV, and 7 percent of those negative for p16 were positive for HPV. However, studies using p16 (tumor suppressor protein) as a surrogate marker for HPV positivity appear to have demonstrated a similar impact on survival. The p16 status, as assessed by immunohistochemistry, may provide additional information beyond HPV positivity. In a study comparing the effect of p16 expression and HPV DNA presence, cases that were HPV positive with high p16 expression had a better prognosis than those that were HPV positive but with low expression.
- 17. Human Papillomavirus (HPV) infection of epithelial cells. HPVs infect basal cells of squamous epithelia through sites of mechanical trauma. Infections with high-risk HPVs can lead to dysplasia and carcinoma in situ and to invasive squamous cell carcinoma. Progression is a rare and slow process and many lesions regress spontaneously.
- 18. HPV and Oropharyngeal Cancer Latency from infection: Cervix (29 years) peak infection (20y) to cancer (49y) HPV (10-30y) peak infection (25-30 and 55-60) and cancer 58y HPV Vaccine impact expected by 2050
- 19. Latency from Infection to Cancer
- 20. Site Male Female Tongue 11,700 4,400 Mouth 7,600 5,310 Pharynx 13,350 3,070 Oral (other) 2,130 770 New Cancer Cases in the US in 2016
- 21. Age: 10 y younger on one study median age 57 (versus 61 for HPV -) Gender: 76% male Smaller primary: T1/T2 64% (versus 44% for HPV -) More Neck Nodes: N2/N3 in 69% (versus 51% for HPV -) Less likely to have a second primary: 6% versus 13%
- 22. Most Common in White Men
- 23. Median Age for Women is 62
- 24. Median Age for Men is 59
- 25. Typical smoking related oropharynx cancer, presented with months of throat pain radiating into ear
- 26. In HPV + cancers the primary may be small and hard to see Squamous Cell Carcinoma. This human papillomavirus-positive tumor presented as a diffuse erythroplakia of the left soft palate and tonsillar region.
- 27. Oropharynx Symptoms Based on HPV Status HPV + HPV – Neck mass (51%) Sore Throat (53%) Sore Throat (28%) Dysphagia (41%) Dysphagia (10%) Neck Mass (18%)
- 28. 50 yo non-smoker, white male present with a lump in his left neck and the PET scan as noted
- 29. Typical Imaging for HPV Oropharynx Cancer CT = large cystic node metastases PET = large neck mass with small primary in tonsil
- 30. CT Scan Typical HPV + Patient Large, Lobulated neck mass of lymph nodes with no obvious primary source Neck biopsy = squamous
- 31. Ultrasound Typical HPV + Patient Large, Lobulated neck mass of lymph nodes with no obvious primary source
- 32. PET Scan Typical HPV + Patient Large lymph node metastases in the neck with no obvious primary source
- 33. Small cancer in left base of tongue Large, necrotic lymph node mass Stage IVA Squamous Cancer Left Base of Tongue, HPV +
- 34. HPV Oropharynx Cancer 50 yo man, non-smoker presented with cystic neck nodes and occult primary in the base of tongue
- 35. HPV Oropharynx Cancer 53 yo man with large cystic neck node and occult primary in base of tongue
- 36. HPV Tonsil Cancer 63 yo non- smoker man presents with neck mass and small lesion in tonsil He was non- smoker Bx = squamous ISH = high risk HPV IVA (T1N2b)
- 38. 53 yo non-smoker presents with a painless lump in the neck and no symptoms inside his throat. On exam 3-4 cm right cervical node and right tonsil ? firm
- 39. PET-CT = hot, cystic neck node and small lesion in tonsil Path = squamous cancer, HPV +
- 40. Survival for Tonsil Cancer HPV + HPV -
- 41. Long-term prognosis and risk factors among patients with HPV-associated oropharyngeal squamous cell carcinoma Cancer Volume 119, Issue 19, pages 3462–3471, 1 October 2013 patients with human papillomavirus (HPV)-associated oropharyngeal squamous cell carcinoma (HPV-OSCC) HPV-OSCC who received treatment at the Johns Hopkins Hospital between 1997 and 2008 and who had tissue available for HPV testing
- 42. Long-term prognosis and risk factors among patients with HPV-associated oropharyngeal squamous cell carcinoma Cancer Volume 119, Issue 19, pages 3462–3471, 1 October 2013 In total, 157 of 176 patients (90%) with OSCC had HPV-associated disease (HPV- OSCC). In the patients with HPV-OSCC, the 3- year and 5-year OS rates were 93% and 89% respectively.
- 43. Trials of Oropharynx Cancer Improved Survival with HPV + Author Survival HPV + HPV – Ang 82%/3y 57%/3y Ang 86%/3y 60% Gillison 49%/5y 19.6% Posner 82%/5y 35% Rischin 91%/2y 74% Cancer Control July 2016, Vo.23, No 3
- 44. Effect of HPV-Associated p16INK4AExpression on Response to Radiotherapy in Squamous Cell Carcinoma of the Head and Neck JCO April 20, 2009 vol. 27 no. 12 1992-1998 Local Control
- 45. JCO April 20, 2009 vol. 27 no. 12 1992-1998 Overall Survival
- 46. Better Survival Out To 10 Years JCO June 10, 2012 vol. 30 no. 17 2102-2111 Non-smokers smokers SURVIVAL Years
- 47. www.NCCN.org
- 49. As of 2016 the NCCN guidelines do not recommend treating HPV + patients with less intense therapy
- 50. parotid parotid cancer in tonsil cancer in nodes Radiation zone brain Typical Radiation Field for Cancer in Right Oropharynx Part of the radiation includes the obvious cancer and other lymph node sites in the next but tries to spare normal structures like the parotid and brain
- 51. Quick Response to Radiation combined with chemotherapy, Tonsil cancer gone by 2 ½ weeks Squamous Tonsil Cancer 2.5 weeks after chemoradiation
- 53. Chemoradiation JCO September 20, 2010 vol. 28 no. 27 4142-4148 HPV + HPV -
- 54. Local Control Very High with Erbitux + XRT in HPV + Patients
- 55. Survival Very High with Erbitux + XRT in HPV + Patients
- 56. Standard Stage System (AJCC 7th)
- 57. Standard Stage System (AJCC 7th)
- 58. Standard Stage System (AJCC 7th)
- 59. Standard Stage System (AJCC 7th) Single node and stage III
- 60. Standard Stage System (AJCC 7th) Nodes and Stage IVa
- 61. Superior Cure Rates if HPV + JCO March 10, 2015 836-845 5 Year Survival HPV + HPV -
- 62. Survival with Oropharynx Cancer if HPV + JCO March 10, 2015 836-845
- 63. JCO March 10, 2015 836-845 Survival with Oropharynx Cancer if HPV -
- 64. 5 Year Survival in 1907 patients with HPV+ oropharyngeal cancer Stage I: 88% II: 82% , III: 84%, and IVA: 81%, IVB: 60% 5-year overall survival did not differ among N0 (80%) N1– N2a (87%), and N2b (83%) subsets, but was significantly lower for those with N3 disease (59% ) So need to change the staging system (only deeply invasive T4b or huge nodes (N3 > 6cm) do poorly Lancet Oncology Volume 17, No. 4, p440–451, April 2016
- 65. Survival Related to HPV, Stage and Smoking
- 66. Survival if HPV + based on smoking (PY = pack years) age and stage JCO March 10, 2015 836-845
- 67. Survival for HPV + Using Nasopharyngeal Node Categories for Staging. Series of 661 from MD Anderson, stage I disease into two groups: stage IA, defined as T1, N0-N2; and stage IB, defined as T2, N0-N2. Stage II would be defined as T1-T2, N3 or T3, N0-N3; stage III would be defined as T4 regardless of nodal involvement, and stage IV would be all M1 tumors Dahlstrom JCO 2016;34:183 Overall Survival Months
- 68. New ICON-S staging system was proposed for patients with HPV positive oropharyngeal cancer Stage TNM 5 Year Survival Stage I T1-2N0-1 85-88% Stage II T3 or N2 78-81% Stage III T4 or N3 53-65%
- 69. Short Term Side Effects of Radiation to the Throat and Neck 1. Skin irritation 2. Dry Mouth and changes in taste and possible problems with teeth 3. Sore throat and problems with swallowing and dehydration and possible need for a feeding tube 4. Pain management problems 5. Laryngitis 6. Fatigue
- 70. Long Term Side Effects of Radiation to the Throat and Neck 1. The dryness may be permanent, depending on the amount of saliva glands in the field 2. Teeth may be vulnerable to decay, and caution is need with future dental care to avoid jaw bone problems (osteonecrosis) 3. Problems with swallowing 4. Persistent hoarseness 5. Small risk of low thyroid 6. Carotid stenosis
- 71. Because of the favorable outcome for HPV patients and the severity of side effects of standard chemoradiation, there are numerous research trials on going to see if less intensive treatment will be effective using a lower dose of chemotherapy or radiation Toxicity from High Dose Chemo-Radiation Large Tonsil cancer Last Day of Treatment
- 73. De-Escalation Trials for HPV…Can we use less chemotherapy or lower dose radiation and get the same result with less toxicity?
- 74. Cancer Control July 2016, Vo.23, No 3
- 75. Cancer Control July 2016, Vo.23, No 3
- 76. Cancer Control July 2016, Vo.23, No 3
- 78. Cancer Control July 2016, Vo.23, No 3
- 79. Projected Numbers of New Cases in the Future Oropharynx (all) Oropharynx (men) Cervix) Oropharynx (women)
- 80. Projected Numbers of New Cases in the Future Oropharynx Oral Cavity Larynx Other pharynx Calendar Year
- 81. HPV Infection and Cancer of the Oropharynx 1.Prevention: get kids vaccinated 2.Diagnosis: younger white men with a lump in the neck 3.Treatment: very high cure rates with modern chemo-radiation and perhaps with less intense therapy in the future.