paediatric gastroenteritis : emergency medicine
•
6 gefällt mir•970 views

paediatric gastroenteritis : emergency medicine

Empfohlen
Empfohlen
Weitere ähnliche Inhalte
Was ist angesagt?
Was ist angesagt? (20)
Ähnlich wie paediatric gastroenteritis : emergency medicine
Ähnlich wie paediatric gastroenteritis : emergency medicine (20)
Mehr von Medvizz institute of medical education
Mehr von Medvizz institute of medical education (20)
Kürzlich hochgeladen
Kürzlich hochgeladen (20)
paediatric gastroenteritis : emergency medicine
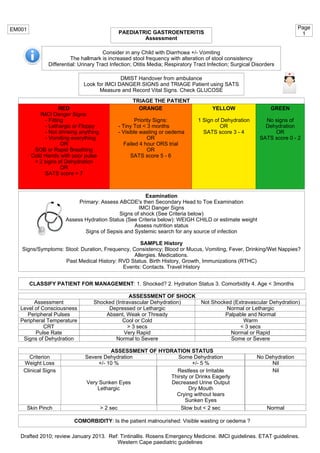
- 1. PAEDIATRIC GASTROENTERITIS Assessment EM001 Consider in any Child with Diarrhoea +/- Vomiting The hallmark is increased stool frequency with alteration of stool consistency Differential: Urinary Tract Infection; Otitis Media; Respiratory Tract Infection; Surgical Disorders DMIST Handover from ambulance Look for IMCI DANGER SIGNS and TRIAGE Patient using SATS Measure and Record Vital Signs. Check GLUCOSE RED IMCI Danger Signs: - Fitting - Lethargic or Floppy - Not drinking anything - Vomiting everything OR SOB or Rapid Breathing Cold Hands with poor pulse > 2 signs of Dehydration OR SATS score > 7 Examination Primary: Assess ABCDE's then Secondary Head to Toe Examination IMCI Danger Signs Signs of shock (See Criteria below) Assess Hydration Status (See Criteria below): WEIGH CHILD or estimate weight Assess nutrition status Signs of Sepsis and Systemic search for any source of infection SAMPLE History Signs/Symptoms: Stool: Duration, Frequency, Consistency; Blood or Mucus, Vomiting, Fever, Drinking/Wet Nappies? Allergies. Medications. Past Medical History: RVD Status. Birth History, Growth, Immunizations (RTHC) Events: Contacts. Travel History ORANGE Priority Signs: - Tiny Tot < 3 months - Visible wasting or oedema OR Failed 4 hour ORS trial OR SATS score 5 - 6 GREEN No signs of Dehydration OR SATS score 0 - 2 YELLOW 1 Sign of Dehydration OR SATS score 3 - 4 ASSESSMENT OF SHOCK Assessment Level of Consciousness Peripheral Pulses Peripheral Temperature CRT Shocked (Intravascular Dehydration) Not Shocked (Extravascular Dehydration) Depressed or Lethargic Absent, Weak or Thready Cool or Cold > 3 secs Normal or Lethargic Palpable and Normal Warm < 3 secs Drafted 2010; review January 2013. Ref: Tintinallis. Rosens Emergency Medicine. IMCI guidelines. ETAT guidelines. Western Cape paediatric guidelines ASSESSMENT OF HYDRATION STATUS Criterion No DehydrationSevere Dehydration Some Dehydration Weight Loss Nil+/- 5 %+/- 10 % Clinical Signs Nil Skin Pinch NormalSlow but < 2 sec> 2 sec Restless or Irritable Thirsty or Drinks Eagerly Decreased Urine Output Dry Mouth Crying without tears Sunken Eyes Very Sunken Eyes Lethargic Page 1 Pulse Rate Signs of Dehydration Very Rapid Normal or Rapid Normal to Severe Some or Severe TRIAGE THE PATIENT CLASSIFY PATIENT FOR MANAGEMENT: 1. Shocked? 2. Hydration Status 3. Comorbidity 4. Age < 3months COMORBIDITY: Is the patient malnourished: Visible wasting or oedema ?
- 2. PAEDIATRIC GASTROENTERITIS Management SHOCKED SOME DEHYDRATION SEVERE DEHYDRATION NO DEHYDRATION RESUSCITATE IV/IO bolus N/S 20 ml/kg as fast as possible (10 ml/kg if wasted/oedematous) Unable to site IV/IO - Insert NGT: Start ORS at 30 ml/kg/hr (10 ml/kg/hr if wasted/oedematous) Able to take PO Urine Dipstix if Pyrexial - Supply ORS and cup - Calculate Volume (table below) - Give Small Volumes: 20-50mls every 15min - If child vomits: Give smaller Volume at a time - If child has loose stools: Give Extra 10ml/kg - Continue breast feeding as usual Caregiver to alert nurse if child repeatedly vomits or refuses to drink Record on Chart Reassess at 2 hours or sooner if required Check ABC; Watch for Danger Signs; Weigh the child Reclassify: Assess Hydration, Vomiting and Willingness to Drink Amount of ORS over 4 Hours Age Weight Mls 4-12 months 1-2 years 2-5 years 6-10 kg 10-12 kg 12-19 kg 400-700 mls 700-900 mls 900 - 1400 mls IF NEEDS TRANSFER CONSULT PAEDIATRIC FLYING SQUAD CRITERIA DISCHARGE Record Visit on RTHC Provide ORS Educate caregiver: - How to give ORS and feed the child - Danger signs to look out for Zinc x 10 days <1yr 10 mg/d >1yr 20 mg/d Drafted 2010; review January 2013. Ref: Tintinallis. Rosens Emergency Medicine. IMCI guidelines. ETAT guidelines. Western Cape paediatric guidelines EM001 Page 2 Assess Nutrition Status Wasted Oedematous Severe Malnutrition Well Nourished Insert NGT Infuse ORS @ 10 ml/kg/hr Site IV to Take Bloods BC; FBC; U&E; Protein; Albumin; Venous Gas Set up IV Commence 1/2DD IV @ 20 ml/kg/hr FOR UP TO 4 HRS (NGT if unable - Infuse ORS 20ml/ kg/hr) Take Bloods: U&E Assess and Manage ABC's Administer OXYGEN Check Sugar: Treat if < 3mmol/l (5ml/kg 10% dextrose IV) Site IV (preferred) or IO Line Call for help: EM Consultant or Paediatric Registrar STILL SHOCKED REASSESS PATIENT NO LONGER SHOCKED - Assess hydration - Use appropriate protocolRepeat IV/IO bolus as above Do ABG; Blood Culture; Na; K; Cl; Urea; Creat; FBC Ceftriaxone 50 mg/kg IV stat Give 1/2 DD IV @ 20 ml/kg/hr (10 ml/kg/hr if wasted/oedematous) Review Regularly Admit Level 3 Paediatrics Assess and Manage ABC's Administer OXYGEN Check Sugar: Treat if < 3mmol/l (5ml/kg 10% dextrose IV) Admit Level 2 Paediatrics Admit Level 2 Paediatrics START ORS TRIAL Vomiting everything or taking nothing Some Dehydration. Failed Trial of ORS Continue ORS trial Reassess 2 hours later NOTE STARTING TIME ON CHART Encourage mother to breastfeed Otherwise withhold oral feeds Failed Trial of ORS Not Dehydrated ORS retained Increased weight Child still drinking Record on Chart - Reassess at 2 then 4 hours Check ABC; Watch for Danger Signs; Weigh the child Reclassify: Assess Hydration, Vomiting and Willingness to Drink Not Dehydrated ORS retained Increased weight Child drinking Shocked or Severe Dehydration Follow protocols Some Dehydration No Increased Weight Not Drinking Admit Paediatrics Stop NGT Try OralVomits Retained If still SHOCKED consider Intubation and Inotropes REASSESS PATIENT Admit Level 2 Paediatrics NO LONGER SHOCKED - Assess hydration - Use appropriate protocol Admit Paediatrics (Consider Level 2) STILL SHOCKED REASSESS PATIENT NO LONGER SHOCKED - Assess hydration - Use appropriate protocolRepeat IV/IO bolus as above Admit Level 2 Paediatrics Well Nourished Malnourished OR <3 mths Insert Size 8 NGT: Attach NGT Drip set and 200 mls bottle of ORS Start ORS via NGT FOR UP TO 4 HRS NOTE STARTING TIME ON CHART Encourage mother to breastfeed Otherwise withhold oral feeds Admit Level 2 Paediatrics ORS @ 20ml/kg/hr ORS @ 10ml/kg/hr Increase Infusion to 30ml/kg/hr