
Empfohlen
Weitere ähnliche Inhalte
Was ist angesagt?
Was ist angesagt? (20)
Andere mochten auch
Andere mochten auch (20)
Ähnlich wie Trichotillomania
Ähnlich wie Trichotillomania (17)
Mehr von discoverccs-org
Mehr von discoverccs-org (15)
Kürzlich hochgeladen
Kürzlich hochgeladen (20)
Trichotillomania
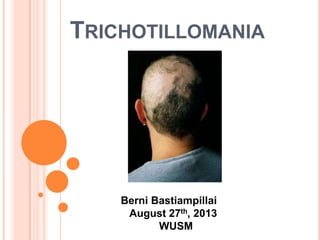
- 1. TRICHOTILLOMANIA Berni Bastiampillai August 27th, 2013 WUSM
- 2. DEFINITION Is the compulsive urge to pull out (and in some cases, eat) one's own hair leading to noticeable hair loss, distress, and social or functional impairment. It is classified as an impulse control disorder by DSM-IV and is often chronic and difficult to treat.
- 3. HISTORY Hair pulling was first described in the literature in 1885, and the term trichotillomania was coined by the French dermatologist François Henri Hallopeau in 1889. It was not until 1987 that trichotillomania was recognized in the Diagnostic and Statistical Manual of the American Psychiatric Association, third edition-revised (DSM-III-R).
- 4. INCIDENCE AND PREVALENCE Trichotillomania’s peak age of onset is from 9 to 13 years of age. It may be triggered by depression or stress. Owing to social implications the disorder is often unreported and it is difficult to accurately predict its prevalence. However, the lifetime prevalence is estimated to be as high as 1.5% (in males) to 3.4% (in females).
- 5. DIFFICULTIES OF DIAGNOSIS Trichotillomania includes the criteria of an increasing sense of tension before pulling the hair and gratification or relief when pulling the hair. However, some people with trichotillomania do not endorse the inclusion of "rising tension and subsequent pleasure, gratification, or relief" as part of the criteria because many individuals with trichotillomania may not realize they are pulling their hair. Patients presenting for diagnosis may deny the criteria for tension prior to hair pulling or a sense of gratification after hair is pulled.
- 6. CLASSIFICATIONS: AUTOMATIC VS. FOCUSED Trichotillomania is often not a focused act, but rather hair pulling occurs in a "trance-like" state. Hence, trichotillomania is subdivided into "automatic" versus "focused" hair pulling. Children are more often in the automatic, or unconscious, subtype and may not consciously remember pulling their hair. Other individuals may have focused, or conscious, rituals associated with hair pulling, including seeking specific types of hairs to pull, pulling until the hair feels "just right", or pulling in response to a specific sensation. Knowledge of the subtype is helpful in determining treatment strategies.
- 7. SIGNS AND SYMPTOMS People who suffer from trichotillomania often pull only one hair at a time and these hair pull episodes can last for hours at a time. Trichotillomania can go into relapse-like states where the individual may not experience the urge to "pull" for days, weeks, months, and even years. Individuals with trichotillomania exhibit hair of differing lengths. Some are broken hairs with blunt ends, some new growth with tapered ends, some broken mid-shaft, or some uneven stubble. Scaling on the scalp is not present, overall hair density is normal, and a hair pull test is negative (the hair does not pull out easily). Individuals with trichotillomania may be secretive or shameful of the hair pulling behavior.
- 8. STRESS AND HEALTH Low self-esteem, often associated with being shunned by peers and the fear of socializing due to appearance and negative attention they may receive. Some people with trichotillomania wear hats, wigs, false eyelashes, eyebrow pencil, or style their hair in an effort to avoid such attention. There seems to be a strong stress component. In low-stress environments, some exhibit no symptoms (known as "pulling") whatsoever. This "pulling" often resumes upon leaving this environment. Other medical complications include infection, permanent loss of hair, and gastrointestinal obstruction as a result of trichophagia. In trichophagia, people with trichotillomania ingest the hair that they pull and in extreme and rare cases, this can lead to a hair ball (bezoar). Rapunzal’s Syndrome, an extreme form of trichobezoar in which the "tail" of the hair ball extends into the intestines, this can be fatal if misdiagnosed.
- 9. ENVIRONMENT Environment is a large factor which affects hair pulling. Sedentary activities such as being in a relaxed environment are conducive to hair pulling. An extreme example of automatic trichotillomania is found when some patients have been observed to pull their hair out while asleep. This is called sleep- isolated trichotillomania.
- 10. DIFFERENTIAL DIAGNOSIS Anxiety, depression and obsessive–compulsive disorder are more frequently encountered in people with trichotillomania. Trichotillomania has a high overlap with post traumatic stress disorder. Differential diagnosis must be pursued before a dianogsis of trichotillomania can be made with certainty. The differential diagnosis will include evaluation for alopecia areata, tinea capitis, traction alopecia, and loose anagen syndrome.
- 11. PROGNOSIS When it occurs in early childhood (before five years of age), the condition is typically self-limiting and intervention is not required. In adults, the onset of trichotillomania may be secondary to underlying psychiatric disturbances and symptoms are generally more long-term. Secondary infections may occur due to picking and scratching, but other complications are rare. Individuals with trichotillomania often find that support groups are helpful in living with and overcoming the disorder.
- 12. TREATMENT Establishing the diagnosis and raising awareness of the condition is an important reassurance for the family and patient. Non-pharmacological interventions, including behavior modification programs, may be considered. Referrals to psychologists or psychiatrists are considered when other interventions fail. The hair pulling may resolve when attributable conditions are treated.
- 13. PSYCHOTHERAPY Habit reversal training (HRT) has the highest rate of success in treating trichotillomania. HRT has been shown to be a successful adjunct to medication as a way to treat trichotillomania. With HRT, the individual is trained to learn to recognize their impulse to pull and also teach them to redirect this impulse. In comparisons of behavioral versus pharmacologic treatment, cognitive behavioral therapy (including HRT) have shown significant improvement over medication alone. It has also proven effective in treating children.
- 14. MEDICATIONS Clomipramine, a tricyclic antidepressant, was shown to significantly improve symptoms. Fluoxetine (Prozac) and other selective serotonin reuptake inhibitors (SSRIs) have limited usefulness in treating trichotillomania, and can often have significant side effects. Behavioral therapy has proven more effective when compared to fluoxetine or control groups. Dual treatment (behavioral therapy and medication) may provide an advantage in some cases. Acetylcysteine treatment stemmed from an understanding of glutamate's role in regulation of impulse control. HOWEVER, Many medications, depending on individuality, may actually increase hair pulling, so be aware of potential side effects!
- 15. CITATIONS: 1) Hemmings SM, Kinnear CJ, Lochner C, et al. (2006). "Genetic correlates in trichotillomania--A case-control association study in the South African Caucasian population". Isr J Psychiatry Relat Sci 43 (2): 93–101. PMID 16910371. Greer JM, 2) Capecchi MR (January 2002). "Hoxb8 is required for normal grooming behavior in mice". Neuron 33 (1): 23–34. doi:10.1016/S0896-6273(01)00564-5. PMID 11779477. James, William; Berger, 3) Timothy; Elston, Dirk (2005). Andrews' Diseases of the Skin: Clinical Dermatology (10th ed.). Saunders. p. 63. ISBN 0-7216- 2921-0. 4) Grant, J. E.; Odlaug, B. L.; Won Kim, S. (2009). "N- Acetylcysteine, a Glutamate Modulator, in the Treatment of Trichotillomania: A Double-blind, Placebo-Controlled Study". Archives of General Psychiatry 66 (7): 756–63. 5) Swedo SE, Leonard HL, Rapoport JL, Lenane MC, Goldberger EL, Cheslow DL (1989). "A double-blind comparison of clomipramine and desipramine in the treatment of trichotillomania (hair pulling)". N. Engl. J. Med. 321 (8): 497– 501
- 16. THANK YOU!