Occulo motor nerve dnm
•Als PPTX, PDF herunterladen•
3 gefällt mir•494 views

for study purpose

Empfohlen
Weitere ähnliche Inhalte
Was ist angesagt?
Was ist angesagt? (20)
Ähnlich wie Occulo motor nerve dnm
Ähnlich wie Occulo motor nerve dnm (20)
Kürzlich hochgeladen
Kürzlich hochgeladen (20)
Occulo motor nerve dnm
- 2. The cranial nerves 12 in number. Are part of the peripheral nervous system. The craniocaudal sequence of cranial nerves is as follows • 1- Olfactory • 2- Optic • 3- Oculomotor • 4- Trochlear • 5- Trigeminal • 6- Abducent • 7- Facial • 8- Vestibulocochlear • 9- Glossopharyngeal • 10- Vagus • 11- Accessory • 12- Hypoglossal All exit the cranial cavity through foramina or fissures. All originate from the brain. Contain sensory, motor or both components
- 4. MOTOR (EFFERENT) PARTS OF CRANIAL NERVES: • Arise within brain from group of nerve cells, which constitute their nuclei of origin. • They are connected with cerebral cortex by corticonuclear fibres, these arise from cells of motor areas of the cortex, descend chiefly in genicular part of internal capsule to brainstem,
- 5. SENSORY (AFFERENT) CRANIAL NERVES: •Arise from nerve cells outside brain, these nerve cells may be grouped to form ganglia on trunks of the nerves, or may be situated in peripheral sensory organs such as the nose, eye & ear. •The centrally directed processes of the cells run into brain & there end around nerve cells, which are grouped to form their nuclei of termination. • Fibres arise from cells of these nuclei and, usually after crossing to opposite side, run up to connect the nuclei indirectly with cerebral cortex.
- 6. The nuclei of the cranial nerves. Sensory nuclei are illustrated on the left Motor nuclei on the right.
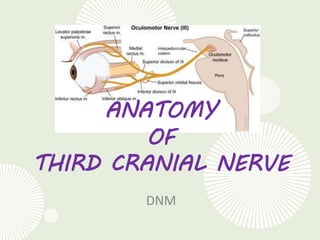
- 8. • Third cranial nerve. • It is the largest of the ocular motor nerves. • It contains some 15,000 axons, including motor fibers and parasympathetic motor fibers. • Entirely motor in function. • Supplies LPS and all extra ocular muscles except lateral rectus and superior oblique. • Also supplies the intraocular muscles namely sphincter pupillae and ciliary muscle
- 11. FUNCTIONAL COMPONENTS • Somatic efferent component is concerned with the movements of the eyeball – motor supply to muscles derived from head myotomes-LPS, SR,MR,IR and IO. • General visceral efferent (parasympathetic) component of the nerve is meant for accommodation and contraction of the pupil – motor supply to ciliaris and sphincter pupillae. • General somatic afferant component of the nerve is associated with proprioceptive impulses from the extraocular muscles supplied by the somatic efferent component of this nerve.
- 12. OCULOMOTOR NUCLEAR COMPLEX • Located in midbrain at the level of superior colliculus, in the ventromedial part of the central grey matter that surrounds the cerebral aqueduct.
- 13. • It is a longitudinal column of about 10mm length. RELATIONS: • Dorsomedial: central grey zone surrounding aqueduct. • Ventrolateral: medial longitudinal bundle. • Superior: approaches floor of third ventricle. • Inferior: continuous with trochlear nucleus
- 16. • The nucleus of the third cranial nerve is located in the inferior periaqueductal gray matter of the mesencephalon. • It is a complex of both paired and midline motor cells. • These cells are found from the posterior commissure superiorly to the pontomesencephalic junction caudally in the dorsal midbrain.
- 17. • Classically, this complex has been described with four paired subnuclei supplying innervation to the inferior, medial, and superior rectus muscles and to the inferior oblique muscle. • LPS has bilateral supply while All other EOM get ipsilateral supply • Innervation of the extraocular muscle from the paired nuclei is ipsilateral for the inferior and medial rectus muscles and the inferior oblique muscle. • However, innervation of the superior rectus is contralateral. Hence bilateral superior rectus palsy • The motor fibers to the superior rectus decussate within the third nerve nucleus and join the fascicle of the contralateral oculomotor nerve.
- 18. • In addition to the extraocular muscle motor fibers, the Edinger-Westphal nuclei supply the parasympathetic preganglionic neurons that project to the ciliary ganglion. • These nuclei are positioned dorsal and medial to the muscle motor nuclei. • They are composed of two cell groups, a medial unpaired column and a lateral paired column. • All evidence suggests that these fibers project ipsilaterally.
- 20. OCULOMOTOR NERVE NUCLEI: Include two motor nuclei: Main Motor Nucleus: Site : ventral part of central grey matter "surrounding the cerebral aqueduct", of midbrain, at the level ofsuperior colliculus, close to median plane. Supply : all extrinsic muscles of the eye except superior oblique & lateral rectus. The levator palpebrae superioris muscles of both sides are supplied by single central group of cells "central caudal nucleus". The superior rectus muscle is supplied by contralateral oculomotor nucleus. The remaining muscles are innervated by ipsilateral oculomotor nucleus.
- 21. • It is composed of subnuclei supplying individual extraocular muscles as follows : 1. Dorsolateral Nucleus : Ipsilateral Inferior Rectus 2. Intermedial Nucleus : Ipsilateral Inferior Oblique 3. Ventromedial Nucleus : Ipsilateral Medial Rectus 4. Paramedial (Scattered) Nucleus : Contralateral Superior Rectus 5. Caudal Central Nucleus : Bilateral Levator Palpebrae Superioris
- 22. Warwick's arrangement of the III cranial nerve subnuclei, illustrating the pattern of motor cells in the brain stem that sends fibers to each of the extraocular muscles in the oculomotor nuclei
- 24. Accessory parasympathetic (EDINGERWESTPHAL) nucleus: Site : it lies dorsal to the main motor nucleus. Supply : the axons, which are preganglionic accompany other oculomotor fibres to relay within ciliary ganglion in orbit and supply sphincter pupillae & ciliary muscles via short ciliary nerves. It consists of a median and two lateral components. The cranial half of the nucleus is concerned with light reflexes and the caudal half with accommodation.
- 26. FASCICLE • The fascicular portion of the oculomotor nerve descends as its moves ventrally and laterally through the mesencephalon. • The fascicles pass through the medial longitudinal fasciculus, the red nucleus, and the medial portion of the cerebral peduncle. • During the passage through the ventral midbrain, there appears to be topographic organization of the fascicles so that a divisional paresis is possible even with intrinsic lesions. • The oculomotor nerve exits the brain stem into the interpeduncular fossa as a horizontal arrangement of multiple fiber bundles that rapidly coalesce to form the subarachnoid portion of the third cranial nerve.
- 27. Cross-sections of the brain stem. (A) Through superior colliculus, showing cranial nerve III nuclei with intramedullary fibers.
- 28. CONNECTIONS 1. Cerebral cortex • Motor cortex (precentral gyrus) of both sides through corticonuclear tracts. • Visual cortex through the superior colliculus and the tactobulbar tract. • Frontal eye field. 2. Nuclei of 4th, 6th and 8th cranial nerves through the medial longitudinal bundle. 3. Pretectal nucleus of both sides (for light reflex) 4. Vertical and torsional gaze centers through the medial longitudinal bundle. 5. Cerebellum through the vestibular nuclei.
- 29. DEEP ORIGIN : • The oculomotor fibres run forwards from nuclear complex passing through MLF, tegmentum, red nucleus & medial part of substantia nigra, forming series of curves with lateral convexity. • They emerge from sulcus oculomotor on medial side of cerebral peduncle.
- 30. SUPERFICIAL ORIGIN: • The nerve emerges as 10-15 rootlets at sulcus oculomotorius close to upper border of pons, near termination of basilar artery. • As it emerges from brain it is invested by piamater & lies in the subarachnoid space. • It passes between superior cerebellar & posterior cerebral arteries. • Between the two nerves is the posterior perforated substance (fig. N4).
- 33. The Fascicular part : • Fasciculus consists of efferent fibres which pass from the third nerve nucleus through the red nucleus and the medial aspect of the cerebral peduncle • They then emerge from the midbrain and pass into the interpedencular space
- 36. The Basilar part : • Starts as a series of 15-20 rootlets in the interpeduncular fossa. • These coalase to form a large medial and a small lateral root, which unite to form a flattened nerve, which gets twisted bringing the inferior fibres superiorly and superior fibers inferiorly; and thus the nerve becomes a rounded cord. • The nerve then passes b/w the posterior cerebral artery and the superior cerebellar artery and runs forward in the interpeduncular cistern ( running lateral to & parallel with the posterior communicating artery) to reach the cavernous sinus.
- 38. The Intracavernous part : • The nerve enters the cavernous sinus by piercing the posterior part of its roof on the lateral side of the posterior clinoid process. • It then descends to the lateral wall of the sinus, where it lies above the trochlear nerve. • In the anterior part of the cavernous sinus, the nerve divides into superior and inferior divisions which enter the orbit through the middle part of the superior orbital fissure within the annulus of Zinn. • In the fissure, the nasociliary nerve lies in b/w the two divisions, while the abducent nerve lies inferolateral to them.
- 40. lntracavernous course of the ocular motor nerves. CN IIIand CN IV run in the lateral wall of the cavernous sinus along with CN V divisions VI and v2. CN VI runs in close approximation to the carotid artery within the cavernous sinus itself. As the nerves course toward the anterior aspect of the cavernous sinus and the superior orbital fissure, V1 (ophthalmic) divides into 3 branches: the lacrimal, fron tal, and nasociliary nerves. The lacrimal and frontal nerves cross over the top of CN III and CN IV. CN III divides into superior and infe rior divisions, which cross under CN IV to enter the orbital apex through the annulus of Zinn.
- 43. The Intraorbital part : • In the orbit, the smaller superior division ascends on the lateral side of optic nerve & supplies the superior rectus and the LPS . • The larger, inferior division divides into three branches : 1. Nerve To The Medial Rectus passes inferior to the optic nerve. 2. Nerve To Inferior Rectus passes downward and enters the muscle on its upper aspect, and 3. Nerve To Inferior Oblique (longest of the three branches) passes in b/w the IR & LR and supplies the IO from its posterior border. It gives off the motor root to the ciliary ganglion.
- 46. CILIARY GANGLION • Description : Peripheral parasympathetic ganglion and its constituent cells are multipolar. • Size : Small, about the size of pins head. • Shape & color : Flat & reddish-grey. • Site : Near orbital apex in some loose fat between optic nerve & lateral rectus, lying usually on lateral side of ophthalmic artery.
- 47. Roots : recieves posteriorly three roots or rami Parasympathetic (motor) root Sympathetic root Sensory root
- 49. Parasympathetic (Motor) Root: • Carries preganglionic parasympathetic fibres which arise from cells of Edinger-Westphal nucleus and run through oculomotor nerve & its branch to inferior oblique to reach the ganglion. • These fibres are relayed in the ganglion and postganglionic fibres travel in the short ciliary nerves.
- 51. Sympathetic Root : • Is branch from internal carotid plexus which enter the orbit through SOF and reach the ganglion by either: (a) joining it directly, (b) joining the sensory root, or (c) travel via ophthalmic nerve & its nasociliary branch. • It consists of postganglionic fibres from the SCO which traverse the ciliary ganglion without relayto emerge through short ciliaries.
- 52. Sensory Root : • contains sensory fibres from the eyeball, which reach the ganglia via short ciliary nerves and pass through it without interruption. • It leaves the ganglion backwards to join nasociliary nerve near the point where that nerve enters the orbit.
- 54. Branches: • These are the short ciliary nerves, 8-10 delicate filaments which emerge from the ganglion. • They run forwards in wavy course in company with short ciliary arteries, above and below the optic nerve. • They subdivide into 15-20 branches which pierce sclera around optic nerve and pass forwards in delicate grooves on inner surface of sclera.
- 55. • They carry: 1. Parasympathetic fibres: supply sphincter pupillae & ciliary muscles (more than 95% of these fibres are distributed to ciliary muscle which is much larger in volume). 2. Sympathetic fibres: distributed to blood vessels of eyeball and may include the fibres which supply the dilator pupillae when these fibres do not follow their usual course in the ophthalmic, nasociliary and long ciliary nerves. 3. Sensory fibres: supply cornea, iris & choroid.
- 56. BLOOD SUPPLY • The blood supply to the medial aspect of the brainstem is from vessels directly off the Basilar artery. • Small perforators off circumflex arteries (posterior cerebral, superior cerebellar artery) may also supply the fascicular portion of the third nerve as it courses through the ventral midbrain. • The vascular supply of 3rd nerve in subarachnoid space is via vascular twigs from the post. Cerebral A., the sup. Cerebellar A., and the tentorial and dorsal meningeal branches of the meningohypophyseal trunk of the ICA. • In the cavernous sinus, the tentorial, dorsal meningeal, and inferior hypophyseal branches of the meningohypophyseal trunk supply the nerve along with branches from the ophthalmic artery.
- 59. ANATOMICAL BASIS OF CLINICAL FEATURES OF THIRD NERVE PALSY • A complete & a total third nerve palsy is of common occurrence. • May be congenital or acquired. • Clinical features of complete third nerve palsy include :
- 60. (b) complete left ptosis; (a)after manual elevation of upper left eyelid, we can observe left exotropia and hypotropia, and mid-dilated pupil.
- 61. 1. Ptosis - paralysis of LPS muscle. 2. Deviation – out, down and intorted – unopposed action of LR and SO. 3. Ocular movements : • Adduction – MR • Elevation – SR and IO • Depression – IR • Extorsion – IR and IO 4. Pupil is fixed and dilated – paralysis of sphincter pupillae muscle. 5. Accommodation is completely lost – paralysis of ciliary muscle.
- 64. 6. Crossed diplopia – paralytic divergent squint. 7. Head posture – if the pupillary area is uncovered, head takes a posture consistent with the directions of actions of the paralysed muscles, i.e., head is turned on the opposite side, tilted towards the same side and chin is slightly raised.
- 65. FEATURES AND CAUSES OF THIRD NERVE LESIONS AT VARIOUS LEVELS 1. Supranuclear lesions • Lesions of the cerebral cortex and supranuclear pathway produce conjugate paresis which affect both eyes equally. • In supranuclear lesions although position and movements of the eyes are abnormal, they maintain their relative co-ordination and produce no diplopia
- 66. 2. Nuclear lesions • Lesions involving purely the third nerve nucleus are relatively uncommon. • Common causes include ; vascular diseases, demyelination, primary tumors and metastasis • Lesions involving entire nucleus cause an ipsilateral third nerve palsy with ipsilateral sparing and contralateral weakness of elevation. • Lesions involving paired medial rectus subnuclei (ventromedial nucleus) cause a wall-eyed bilateral internuclear ophthalmoplegia ( WEBINO ) characterised by defective convergence and adduction
- 67. 3. Fascicular lesions • Causes are similar to nuclear lesions. Benedikt syndrome involves the fasciculus as it passes through the red nucleus and is characterised by ipsilateral 3rd nerve palsy and contralateral extrapyramidal signs such as hemitremor. Weber syndrome involves the fasciculus as it passes through the cerebral peduncle and is characterised by ipsilateral 3rd nerve palsy and contralateral hemiparesis. Nothangel syndrome involves the fasciculus and the superior cerebellar peduncle and is characterised by ipsilateral 3rd nerve palsy and cerebellar ataxia. Claude syndrome is a combination of Benedikt and Nothangel syndromes
- 68. Lesion in cerebral peduncle , Weber Syndrome (B) Lesion in red nucleus , Benedikt Syndrome (C)
- 70. 4. Lesions involving basilar part of the nerve • As the nerve runs in the subarachnoid space at the base of skull unaccompanied by any other cranial nerve, isolated third nerve palsies are frequently basilar. • Causes : 1. Aneurysms at the posterior communicating artery cause isolated third nerve palsy with involvement of pupil. 2. Extradural hematomas which may cause tentorial pressure cone with downward herniation of the temporal lobe. This compresses the third nerve as it passes over the tentorial edge. Initially there occurs fixed, dilated pupil, which is followed by a total third nerve palsy. 3. Diabetes causes isolated 3rd nerve palsy with sparing of the pupillary reflexes.
- 73. 5. Lesions involving intracavernous part of the nerve • Because of its close proximity to other cranial nerves, intracavernous 3rd nerve palsies are usually assoc. with inv. of the 4th and 6th nerves, and the 1st division of trigeminal nerve. • In intracavernous 3rd nerve palsy, pupil is spared. Sometimes, pupil may be constricted owing to inv of sympathetics.
- 74. • Causes : 1. Diabetes may cause vascular palsy. 2. Pituitary apoplexy – may cause a third nerve palsy as a result of hemorrhagic infarction of a pituitary adenoma (after child birth), with lateral extension into cavernous sinus. 3. Intracavernous lesions – aneurysms, meningiomas, carotid-cavernous fistulae and Tolosa-Hunt syndrome (granulomatous inflammation)
- 75. 6. Lesions of the intraorbital part of the nerve • May cause isolated extraocular muscle palsies or may involve either superior division or inferior division or both. • Causes : orbital tumors, pseudotumors, trauma and vascular diseases.
- 76. 7. Lesions of pupillomotor fibres • B/w the brainstem and the cavernous sinus, pupillomotor fibres are located superficially in the superior median quadrant of the nerve. • They derive the blood supply from the pial blood vessels whereas the main trunk of the 3rd nerve is supplied by vasa nervorum.
- 77. • Surgical lesions such as aneurysms, trauma and uncal herniation characteristically inv the pupil by compressing the pial blood vessels and the superficially located pupillary fibres. • Medical lesions such as diabetes and hypertension usually spare the pupil. This is because the microangiopathy assoc. with these diseases involves the vasa nervorum, causing infarction of the main trunk, but sparing the superficial pupillary fibres.
- 78. CAUSES OF ISOLATED THIRD NERVE PALSY 1. Idiopathic - In about 25% cases 2. Vascular diseases – diabetes and HTN, is the most common cause of pupil-sparing 3rd nerve palsy. In most cases spontaneous recovery occurs within 3 months. Diabetic 3rd nerve palsy is often assoc. with periorbital pain and may occasionally be the presenting feature of diabetes. The presence of pain is therefore not helpful in differentiating b/w aneurysmal and diabetic 3rd nerve palsy.
- 79. 3. Aneurysm of the PCA at its jn with the ICA is very imp cause of isolated painful 3rd nerve palsy with involvement of pupil. 4. Trauma, both direct and secondary to subdural hematoma with uncal herniation, is also a common cause. 5. Miscellaneous. Other rare causes include tumors, vasculitis assoc. with collagen vascular disorders, syphilis and Tb.