Im309 24 25 Sybron
•
3 gefällt mir•280 views

Implants,International Magazine of Oral Implantology DGZI

Empfohlen
Empfohlen
Weitere ähnliche Inhalte
Was ist angesagt?
Was ist angesagt? (20)
Andere mochten auch
Andere mochten auch (10)
Ähnlich wie Im309 24 25 Sybron
Ähnlich wie Im309 24 25 Sybron (20)
Mehr von Virgil Koszegi
Mehr von Virgil Koszegi (6)
Im309 24 25 Sybron
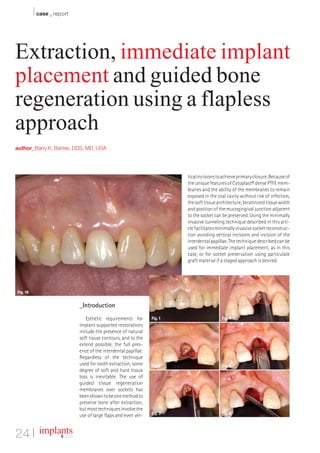
- 1. I case _ report Extraction, immediate implant placement and guided bone regeneration using a flapless approach author_Barry K. Bartee, DDS, MD, USA tical incisions to achieve primary closure. Because of the unique features of Cytoplast® dense PTFE mem- branes and the ability of the membranes to remain exposed in the oral cavity without risk of infection, the soft tissue architecture, keratinized tissue width and position of the mucogingival junction adjacent to the socket can be preserved. Using the minimally invasive tunneling technique described in this arti- cle facilitates minimally invasive socket reconstruc- tion avoiding vertical incisions and incision of the interdental papillae. The technique described can be used for immediate implant placement, as in this case, or for socket preservation using particulate graft material if a staged approach is desired. Fig. 16 _Introduction Esthetic requirements for Fig. 1 Fig. 4 implant supported restorations include the presence of natural soft tissue contours, and to the extend possible, the full pres- ence of the interdental papillae. Regardless of the technique used for tooth extraction, some Fig. 2 Fig. 5 degree of soft and hard tissue loss is inevitable. The use of guided tissue regeneration membranes over sockets has been shown to be one method to preserve bone after extraction, but most techniques involve the Fig. 3 Fig. 6 use of large flaps and even ver- 24 I implants 3_ 2009
- 2. case _ report I Fig. 7 Fig. 8 Fig. 9 Fig. 10 Fig. 11 Fig. 12 Fig. 13 Fig. 14 Fig. 15 _Case Presentation the interdental papillae, taking care to keep the edge of the material a minimum of 1.0 mm away from ad- This is a 60-year-old female who presented with jacent tooth roots (Fig. 12). A single 3-0 PTFE suture a crown-root fracture of a non-vital maxillary right is placed to further stabilize the membrane. The central incisor. The crown was temporarily stabi- membrane is intentionally left exposed, as primary lized with composite resin bonded to the adjacent closure is not required in this technique (Fig. 13). teeth (Fig. 1). Extraction of the tooth and immedi- Figure 14 shows the surgical site at three weeks. ate implant placement was planned. To minimize The exposed membrane is easily removed by grasp- soft and hard tissue recession, a flapless, minimally ing with a tissue forcep. Topical anesthesia may be invasive extraction technique was employed (Fig. used, but local anesthesia is not necessary. 2). The tooth root was extracted using only an in- The site at six weeks after implant placement trasulcular incision. A #15 blade was used to sever (three weeks after membrane removal), reveals ker- the periodontal ligament and create space for root atinized mucosa forming across the former extrac- luxation and elevation (Fig. 3). Next, a subperiosteal tion site (Fig. 15). pocket was created on the buccal and palatal aspect Figure 16 shows the clinical view following of the socket using a micro periosteal elevator (Fig. placement of the implant abutment and acrylic pro- 4). Following luxation and initial elevation of the visional restoration. root with the micro elevator, the tooth was removed with forceps (Fig. 5). The interdental papillae were _Summary carefully undermined and elevated. This can be done with a small periosteal elevator or curette (Fig. The flapless technique described provides a min- 6). All remaining soft tissue was removed from the imally invasive approach to extraction with socket interior and margins of the socket with a sharp grafting or immediate implant placement. Because curette (Fig. 7). The implant osteotomy was done in the interdental papilla remains intact, there is less the standard fashion, with the implant being placed disruption of blood supply. As a result, there is a _contact implants against the palatal wall of the socket (Fig. 8). The gap greater potential for maintenance of soft tissue vol- between the facial aspect of the implant and the ume. In addition, the use of a dense PTFE membrane buccal wall was filled with a combination of auto- Barry K. Bartee, DDS, PA improves the predictability of immediate implant genous bone chips harvested from the implant os- 3234 64th Street placement, excluding the requirement for primary teotomy combined with allograft bone (Fig. 9). A Lubbock,Texas 79413 closure and resultant disruption of soft tissue archi- textured, high-density PTFE barrier membrane is USA tecture._ placed. The membrane is trimmed, then placed into Phone: +1-806-792-0030 Fax: +1-806-792-8730 the superiosteal pocket on the palatal aspect (Fig. Cytoplast® is a registered trademark of Os- E-mail: dr2bkb@aol.com 10). The membrane is then tucked under the facial teogenics Biomedical, Inc. flap (Fig. 11). Next, the membrane is tucked under © 2008 Osteogenics Biomedical, Inc. BBFY0607 implants 3 _ 2009 I 25