
Empfohlen
Weitere ähnliche Inhalte
Was ist angesagt?
Was ist angesagt? (20)
Ähnlich wie bronchiectasis Presentation1.pptx
Ähnlich wie bronchiectasis Presentation1.pptx (20)
Mehr von devanshi92
Mehr von devanshi92 (14)
Kürzlich hochgeladen
Kürzlich hochgeladen (20)
bronchiectasis Presentation1.pptx
- 1. ETIOPATHOGENESIS OF BRONCHIECTASIS By Dr.Amal Thankachan
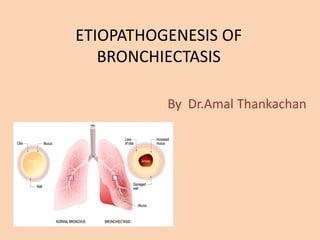
- 2. What is bronchiectasis ? • Bronchiectasis is derived from the Greek words: Bronckos – airway Ectasis – widening • It is a chronic lung condition defined as the abnormal irreversible dilatation of the bronchi,where the elastic and muscular tissue is destroyed by acute or chronic inflammation and infection.
- 3. • Bronchiectasis represents the end stage of a variety of pathologic processes that cause destruction of the bronchial wall and its surrounding supporting tissues. • Etiologies include prior lung infection, systemic inflammatory disorders, and genetic disorders of host defense’ • However, bronchiectasis is considered to be idiopathic in up to half of the affected individuals.
- 4. Pathophysiology • As bronchiectasis is an acquired disorder, its pathophysiology is commonly described as distinct phases of infection and chronic inflammation. • The interaction between these phases establishes a vicious circle in which the end result is the destruction of the bronchi and the accompanying clinical symptoms.
- 5. • Various mechanisms operate to produce permanent, pathologic dilation and damage of the airways. • They may be in of in terms of traction, pulsion, and weakened tensile strength of the airways. • In most cases the pathogenesis becomes invariably linked with and propelled by the destructive effects of chronic infection.
- 6. • As the lung undergoes fibrotic changes consequent to disorders such as sarcoidosis, interstitial lung disorders or infections such as tuberculosis, local retractile forces result in fixed dilation of the airways, or “traction” bronchiectasis. • The prototypic “pulsion” bronchiectasis permanent airway dilatation as a result of intense inflammation originating in the lumen
- 7. • The first stage in the development of bronchiectasis -is an initial infective insult to the airways, which triggers a mucociliary response. • Micro-organisms trigger the release of toxins and an inflammatory response within the airways. • This inflammatory response includes the release of neutrophils, lymphocytes and macrophages within the bronchial lumen.
- 8. • Neutrophils also alter the function of the cilial epithelium, leading to changes in cilial beat frequency and mucous gland hypersecretion. Both processes compromise mucociliary clearance. • Weakness of the airways-eg postinfectious bronchiectasis
- 10. MICROBILOGY “vicious circle” phase of bronchiectasis is dominated by the influx of neutrophils. Neutrophils enter the airway lumina through gaps between epithelial cells ,Neutrophils are attracted by the release of chemokines such as in IL-8 and leukotriene B4 (LTB4) from macrophages, and IL-17 from Th17 cells ,
- 11. • When Initial defenses are unable to contain the infection Robust immune response by airway epithelial cells and phagocytes by Release of inflammatory cytokines and chemokines that include macrophage inflammatory protein-2, IL-8, and TNF-α.
- 12. • Airway infiltration by predominantly neutrophils, macrophages and lymphocytes causes damage to the airway epithelium Through the release of various proteolytic enzymes such as neutrophil elastase and metalloproteinases • Erosion of mucosal barriers, creating microabscesses that can harbor bacteria
- 14. Predisposing or Associated Conditions • POSTINFECTIOUS CONDITIONS • Childhood lower respiratory tract infections • Granulomatous infections • Necrotizing pneumonias in adults Other respiratory infections
- 15. HERITABLE STRUCTURAL ABNORMALITIES • Primary ciliary dyskinesia • Williams-Campbell syndrome • Mounier-Kuhn syndrome • Marfan syndrome
- 16. IDIOPATHIC INFLAMMATORY DISORDERS • Sarcoidosis • Rheumatoid arthritis • Ankylosing spondylitis • Systemic lupus erythematosus • Sjögren syndrome • Inflammatory bowel disease • Relapsing polychondritis
- 17. INHALATION AND OBSTRUCTION • Gastroesophageal reflux/aspiration • Pneumonia • Toxic inhalation/thermal injury • Postobstruction accident • Foreign body • Allergic bronchopulmonary aspergillosis/mycosis • Tumors, benign and malignant • Extrinsic airway compression
- 18. MISCELLANEOUS • HIV infection/AIDS • Yellow nail syndrome • Radiation injury • Lung fibrosis
- 19. CYSTIC FIBROSIS(mucoviscidosis) • CF is caused by a mutation in chromosome 7 q -CFTR gene. • It is the most common autosomal recessive disorder among whites • The CFTR protein produced by this gene regulates the movement of chloride and sodium ions across epithelial cell membranes
- 20. • Cl ion help to lyse mucus • Pt wil hv recurrent pneumonia • Mcc-staphylococcus aureus • Psueudomonas aeroginosa – with the help of biofilm formation • Burkholderia cepacia –pneumonia mc associated with increased mortality • CF and CF variants are one of the most common causes of bronchiectasis
- 22. Youngs syndrome It is seen only in males ,the genetic basis for Young syndrome is not know- Possible mechanism is ciliary dysfunction clinical features of Youngs syndrome • Bronchiectasis and recurrent LRTI • sinusitis • Infertility-obstructive azoospermia
- 23. DISORDERS OF IMMUNITY • Primary diseases that result in immunodeficiency may devolve from mutations that impair B or T lymphocytes and cause abnormal humoral immunity,cellular immunity, or both • Common variable immunodeficiency, or acquired hypogammaglobulinemia is the most frequent syndrome recognized in this group of diseases.
- 24. Acquired Hypogammaglobulinemia • Although there are normal numbers of circulating B lymphocytes, they fail to differentiate into antibodyproducing cells. • This results in particular vulnerability to infections with encapsulated bacteria such • S. pneumoniae, • H. influenzae, • S. aureus, and P. aeruginosa.
- 25. • Other disorders of immunity include • Hyper-IgM or hyper-IgE(Job syndrome) • Impaired production of cytokines secreted by type 1 helper T cells such as interferon-γ (IFN- γ) and TNF-α, cytokines • They are known to be important in controlling such infections. • Increase the susceptibility of individuals to pyogenic bacteria and NTM organisms
- 26. Thymic hypoplasia resulting in abnormal cellular immunity (DiGeorge syndrome) severe combined immunodeficiency syndrome, “bare lymphocyte” syndrome, Wiskott-Aldrich syndrome (an X-linked recessive illness associated with small platelets and eczema) Ataxia-telangiectasia syndrome
- 28. • Each ciliated epithelial cell possesses approximately 200 cilia. The direction of ciliary beating is determined by the orientation of the central pair of microtubules. • Dysfunction of the ciliary apparatus may involve a variety of structural abnormalities in the cilia or disorganization of the ciliary axes.
- 29. • A variety of abnormalities have been described • Including the complete or partial absence of outer or inner dynein arms • A lack of radial spokes • Disordered microtubule arrangements,ciliary disorientation etc
- 30. • PCD (primary ciliary dyskinasia )with situs inversus universalis is known as Kartagener syndrome • The patients have a marked tendency toward colonization and infection with H. influenzae.
- 31. 1 • Ineffective beating of the ciliated cells 2 • Stagnation and accumulation of mucus 3 • early-onset refractory or recurrent infectionsof the upper and lower respiratory tract Bronchiectasis is a common sequela of PCD and it typically involve the dependent zones, including the lower lobes, right middle lobe, and/or the lingular segment of the left upper lobe
- 32. Bronchiectasis: Kartagener syndrome.- CXR-shows dextrocardia with basal predominant linear opacities -bronchial wall thickening and bronchiectasis. Axial chest CT shows dextrocardia and severe, cystic bronchiectasis
- 33. BRONCHIAL CARTILAGE OR ELASTIC FIBER DEFECTS • Mounier-Kuhn syndrome, or congenitaltracheobronchomegaly • It is a rare disorder associated with gross enlargementor dilation of the trachea and segmental bronchi • The underlying defect is atrophy and even absence of elastic fibers and smooth muscle tissues of the large airways. • In addition, primary or secondary atrophy of the connective tissue between the rings may result in outpouchings or diverticula, potentially serving as reservoirs for recurrent infections
- 34. Congenital tracheobronchomegaly (Mounier-Kuhn syndrome) with bronchiectasis. This 73-year-old woman has had recurring respiratory infections throughout her adult life • B-The dilated trachea with prominent cartilaginous rings is confirmed on a CT scan (between arrows). • C, Not only is the trachea Enlarged, but the main-stem bronchi are dilated (between arrows).
- 35. CT images show multifocal, thin-walled cystic bronchiectasis associated with dilated trachea and central bronchi
- 36. • Mounier-Kuhn patients may present in their early years or as late as the fourth decade with recurring lower respiratory infections • In advanced stages, airway collapsibility may result in severe airflow obstruction.
- 37. Williams-Campbell syndrome • Williams-Campbell syndrome or congenital bronchial cartilage deficiency syndrome-It is another rare disorder that tends to present early in life with recurring infection and bronchiectasis. • The absence of cartilage from the segmental to the first few generations of the subsegmental airways is the typical finding in Williams-Campbell syndrome
- 38. Williams-Campbell syndrome This 50-year-old man had a lifelong history of recurring respiratory infections and productive cough. The airways are massively dilated with collections of respiratory secretion spooling in some of the cystic spaces.
- 39. CONNECTIVE TISSUE ABNORMALITIES • Marfan syndrome- due to mutation/defect in the genes that produce fibrillin 1 (FBN1) gene. • Morphologic anomalies seen with Marfan syndrome have been traced to increased localized production of TGF-β, a cytokine that increases susceptibility to mycobacteria. • Marfan syndrome has been linked to middle lobe hypoplasia because the right middle lobe is the most commonly affected lobe in NTM-associated bronchiectasis.
- 40. IDIOPATHIC INFLAMMATORY DISORDERS • Mcc- Sarcoidosis • Mechanisms -diffuse parenchymal scarring resulting in traction and airway distortion, endobronchial granulomatous inflammation including stricture with poststenotic infection, or compression secondary to hypertrophic peribronchial lymphadenopathy. • Bronchiectasis has been seen in 20% to 35% of RA patients undergoing HRCT scanning • Potential causal mechanisms include increased propensity for infections,either intrinsic to RA or secondary to steroid or cytotoxictherapy
- 41. Axial chest CT through the upper lobes in a patient with sarcoidosis shows biapical bronchiectasis with architectural distortion.
- 42. Sjögren syndrome Lymphocytic inflammation impaired function of mucous glands decreased volumes and increased viscosity of mucus poor clearance chronic infection.
- 43. Inflammatory bowel disease & Bronchiectasis common epithelial targets of autoimmunity -inhaled or ingested. cryptogenic infection that incites both airway and intestinal inflammation ulcerative colitis- develop after therapeutic colectomy
- 44. Relapsing polychondritis – It is identified essentially as progressive inflammation, weakness, and deformity of cartilaginous structures, including the ears, nose, larynx, and tracheobronchial tree.Respiratory involvement is a common. And is a major cause of mortality. Bronchiectasis in such patients may bedue to primary bronchial damage and/or recurrent infection. Bronchial cartilage inflammation Airway collapse Airflow limitation
- 45. Relapsing polychondritis. A, Axial inspiratory chest CT shows thickening of the anterior two thirds of the trachea (arrowheads). B, Axial chest CT performed following a forced vital capacity maneuver shows excessive trachea collapse
- 46. ASPIRATION 1. Direct spillage of secretions from the oropharynx, containing a plethora of microorganisms, including microaerophilic and anaerobic bacteria 2.Materials refluxed from the esophagus and/or stomach-contain food particles, hydrochloric acid Biliary or pancreatic secretions, and microbes indigenous to the gut, including Helicobacter pylori.
- 47. When Laryngeal protective functions are imperfect, “microaspiration” MCC is GERD , others including (1) Depressed sensorium (2) Altered brain-stem function (3) Altered laryngeal structure/ Function (4) Esophageal disorders -dysmotility, obstruction by tumors or strictures, muscular dystrophy, achalasia, tracheoesophageal fistulas, or lower esophageal sphincter incompetence . (5) Gastric dysfunction (dysmotility or outlet obstruction).
- 48. • Also chronic coughing, which stresses and dilates the diaphragmatic ring, might disrupt the lower esophageal sphincter and subject the esophagus to distending forces • An additional factor that could contribute to gastroesophageal reflux disease is the medications employed for pulmonary disorders, including anticholinergics, β2-agonists, theophylline, and corticosteroids, all of which impair lower esophageal sphincter function and broadspectrum antibiotics, which alter gastroesophageal flora.
- 49. Toxic inhalation / Thermal injury • Acute and chronic inflammation of the tracheobronchial tree, bronchiolitis, bronchiolitis obliterans, and diffuse alveolar damage may be a consequence of exposure to toxic metal fumes- Aluminum,cadmium,chromium, nickel • Toxic gases like ammonia, chlorine, phosgene, sulfur dioxide • Bronchiectasis may ensue because of either infectious complications of the exposure, denuding of the ciliated epithelium, or progressive fibrosis. • chronic airway damage and bronchiectasis may evolve following thermal or smoke injury.
- 50. POSTOBSTRUCTIVE DISORDERS Foreign bodies/Tumors Airway obstruction Poor drainage Recurrent/chronic infection Bronchiectasis. The more common tumor types include bronchogenic carcinomas particularly the squamous cell variety,carcinoid tumors
- 51. • Extrinsic airway compression due most often to hypertrophic lymphadenitis from granulomatous diseases such as sarcoidosis or infections, including tuberculosis or histoplasmosis, may severely narrow or even occlude large airways • Focal bronchiectasis is seen particularly those with disease limited to only one region/ one segment/ one lobe or even one lung
- 52. Postobstructive bronchiectasis. A–C, Axial chest CT shows severe narrowing of the left lower lobe bronchus (arrow), due to carcinoid tumor. Multifocal bronchiectatic consolidation (arrowheads) is present throughout the left lower lobe
- 53. ALLERGIC BRONCHOPULMONARY ASPERGILLOSIS • Allergic bronchopulmonary aspergillosis • inhaled Aspergillus -lodged in the airways. • proliferating fungi form large mucoid Mucoid plugs • medium-sized bronchi inflammation and distention • thin-walled bronchiectasis of the central airways characteristic of ABPA
- 54. • In ABPA there are intense, immunologically • mediated reactions to inhaled Aspergillus that has • lodged in the airways. The onglomerates that fill the central airways; a • sequela of this airway inflammatory process and mucoid • impaction is bronchiectasis
- 55. • Also in long-standing, inadequately controlled ABPA/M. In such cases, extensive fibrosis and airway distortion may evolve because of uncontrolled inflammation. In these cases the patients may acquire secondary airway pathogens including P. aeruginosa or other gram-negative bacilli as well as NTM. In these “burned-out” cases, the patients may notdemonstrate asthma, eosinophilia,or elevated levels of I
- 56. Bronchiectasis: allergic bronchopulmonary aspergillosis. Above are Axial chest CT shows central bronchiectasis typical of allergic bronchopulmonary aspergillosis.
- 58. IDIOPATHIC BRONCHIECTASIS • Idiopathic is estimated to account for 25% to 50% of cases • It often has a characteristic phenotype of bilateral lower lobe bronchiectasis and chronic rhinosinusitis • Genotyping studies of class I and class IImajor histocompatibility complex molecules indicated that allelic polymorphism for HLA-B (HLA-B5 and HLA-B52), HLA-C (HLA-Cw*03 and and HLA- DR/DQ (HLA-DR1/DQ5) are associated with idiopathic bronchiectasis.
- 59. MISCELLANEOUS • AIDS bronchiectasis has been identifiedin a significant proportion of those undergoing CT scans, including children • Probable pathogenesis involves severe, chronic, and recurrent infections with a variety of opportunistic pathogens • Also oxidative damage associated with infection
- 60. • Yellow nail syndrome is an uncommon disorder marked by the triad of: yellow, thick, dystrophic nails; chronic lymphedema of the face, hands, and lower extremities and pleural effusions. • Recurrent sinusitis and lower respiratory tract infections are common • Abnormal lymphatic structure, increased vascular permeability, deficient immunoglobulin production, and/or ciliary dysfunction.
- 61. • Radiation therapy- typically delivered for carcinoma of the breast or mediastinal tumors including lymphomas may result in profound damage to the central airways. • Focal damage to the cartilage and mucosa of the airways leading to patulous distention and irregularities of the major bronchi in the field of irradiation
- 62. . • Result in profound damage to the central airways. . • Focal damage to the cartilage and mucosa of the airways . • patulous distention and irregularities of the major bronchi in the field of irradiation Radiation therapy
- 63. CT scan shows dense fibrosis and bronchiectasis in the radiation field non–small cell carcinoma of the lung. Pt had received radiation therapy to the right hilar region approximately 18 months previously
- 64. • Cylindrical bronchiectasis is described as failure of the involved airways to taper progressively in their distal course. • Usually, in this condition the bronchial walls are smooth or regular
- 65. • ALPHA1-ANTITRYPSIN ANOMALIES • COPD
- 66. CLASSIFICATION • Varicoid bronchiectasis is an allusion to varicose veins and is marked by irregular dilation, narrowing and outpouching of the airways • Saccular bronchiectasis- also known as cystic bronchiectasis, includes focal or cystic distortion of the distal airways
- 67. • It may be isolated or may be more confluent,producing the appearance of bronchiectatic consolidation and volume loss • Cylindrical bronchiectasis is described as failure of the • involved airways to taper progressively in their distal course
- 68. A-Cylindrical bronchiectasis with the characteristic signet ring appearance B-Varicoid bronchiectasis C-Cystic bronchiectasis