RIDDOR Reporting Requirements
•
0 gefällt mir•129 views

This document outlines the UK's Reporting of Injuries, Diseases and Dangerous Occurrences Regulations 1995 (RIDDOR). It summarizes that employers must notify the enforcing authority if any work-related accidents or incidents result in a fatality, major injury, over-3-day injury, or specified dangerous occurrence. A written report is required within 10 days. Employees must not tamper with evidence at an incident site and leave investigation to supervisors. RIDDOR also has reporting requirements for some occupational diseases.

Empfohlen
Empfohlen
Weitere ähnliche Inhalte
Mehr von Clive Burgess
Mehr von Clive Burgess (20)
Kürzlich hochgeladen
Kürzlich hochgeladen (20)
RIDDOR Reporting Requirements
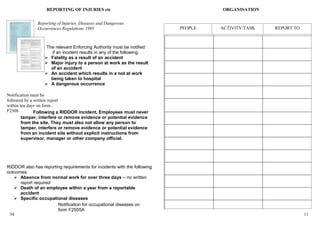
- 1. REPORTING OF INJURIES etc ORGANISATION Reporting of Injuries, Diseases and Dangerous Occurrences Regulations 1995 PEOPLE ACTIVITY/TASK REPORT TO The relevant Enforcing Authority must be notified if an incident results in any of the following: Fatality as a result of an accident Major injury to a person at work as the result of an accident An accident which results in a not at work being taken to hospital A dangerous occurrence Notification must be followed by a written report within ten days on form F2508 Following a RIDDOR incident, Employees must never tamper, interfere or remove evidence or potential evidence from the site. They must also not allow any person to tamper, interfere or remove evidence or potential evidence from an incident site without explicit instructions from supervisor, manager or other company official. RIDDOR also has reporting requirements for incidents with the following outcomes: Absence from normal work for over three days – no written report required Death of an employee within a year from a reportable accident Specific occupational diseases Notification for occupational diseases on form F2505A 34 11
- 2. On back of 12 - 33 INVESTIGATIONS INFORM, INSTRUCT and TRAIN Vehicular ZONE CONTROL SYSTEM Name of Injured Employee ______________________ Date of Accident ______________________________ Job Title _____________________________________________ RISK PPE Issues Housekeeping Prevention FIRE RIDDOR File System Zone Control Electrical Signs Contractors Man. Handling First Aid Auditing COSHH Investigations Time of Accident ______________________________________ GROUND LEVEL Initials Department __________________________________________ Location of Accident ___________________________________ Name of Witness(s) ____________________________________ Description of Accident _________________________________ _____________________________________________________ _____________________________________________________ ________________________________________ _____________________________________________________ Task Being Performed __________________________________ _____________________________________________________ Equipment, Tools, Personal Protective Equipment, Procedures Being Used _____________________________________________________ _____________________________________________________ Description of Injury/Illness (include accident type, injury type and body part injured) _____________________________________________________ _____________________________________________________ Describe All Contributing Factors _________________________ Description of Work Area _______________________________ Injured Employee's Account of Accident __________ _____________________________________________________ Witness’s Account of Accident: (Name, title, address, phone number) _____________________________________________________ What Were the Basic Causes of the Accident (usually multiple causes)? _____________________________________________________ Corrective Measures to be Implemented to Prevent Similar Reoccurrence _____________________________________________________ Investigator’s Name ___________________________________ Date of Investigation __________________________________ 36 9