Castlewood eating disorder treatment center brochure
•
1 gefällt mir•1,839 views

Eating Disorders constitute the most life-threatening category of mental health issues. Castlewood Treatment Center offers comprehensive and highly individualized treatment planning with expert individual therapists for eating disorders, nutritional counseling, marital and relational therapy and trauma-resolution therapy.

Empfohlen
Empfohlen
Weitere ähnliche Inhalte
Was ist angesagt?
Was ist angesagt? (20)
Andere mochten auch
Andere mochten auch (8)
Ähnlich wie Castlewood eating disorder treatment center brochure
Ähnlich wie Castlewood eating disorder treatment center brochure (20)
Mehr von Castlewood Treatment Center
Mehr von Castlewood Treatment Center (9)
Castlewood eating disorder treatment center brochure
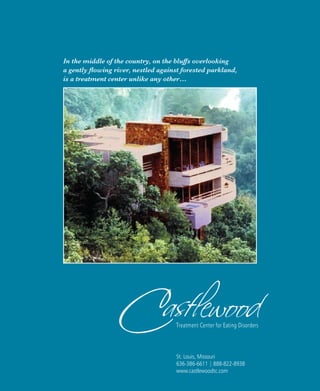
- 1. In the middle of the country, on the bluffs overlooking a gently flowing river, nestled against forested parkland, is a treatment center unlike any other… St. Louis, Missouri 636-386-6611 | 888-822-8938 www.castlewoodtc.com
- 2. Castlewood Treatment Center is a creative collaboration of the owners’ clinical experience and personal and professional evolution. The result is a residential treatment program for eating disorders that allows for the unique treatment of each individual with an emphasis on compassion, respect and empowerment.
- 3. Our vision required that the structure itself be beautiful, unique, and natural, blending harmoniously with its surroundings. Most of all, it had to have the ambiance of a healing community, a sanctuary. After years of searching, we discovered this secluded gem, high on a ridge, overlooking endless acres of state woodlands and the scenic Meramec River.
- 4. Men and women who come to Castlewood are not anorexic; they are not bulimic; they are not compulsive overeaters. At Castlewood we begin with the premise that each person who walks through our doors defies simple categorization. Though we naturally wish to restore our clients to health and functionality as efficiently as possible, we do not place a 30 or 60-day time limit on our residents’ stays. Our mission is not merely to churn out weight-restored women or men who look healthy to others, but whose internal wounds, if unaddressed, will readily result in relapse. Experience has taught us that the full measure of health rests upon more than a temporary absence of symptoms. Castlewood therefore provides an individualized treatment approach tailored to meet the precise needs of each client. We understand that eating disorder clients tend to be more different than similar. This is why at Castlewood, each client’s treatment plan is highly individualized. AN EATING DISORDER is both originated and maintained by a constellation of factors. For each client, every step of the way, we are continually inquiring as a treatment team and in collaboration with the client: what are the necessary and sufficient components of treat- ment needed to restore this person, not only to decreased symptoms, but to a life that is both live-able and worth living? In addition to the eating disorder, some clients have psychiatric diagnoses; some have multiple addictions and some have a history of severe childhood traumas. Some clients will see a specialist for adjunctive therapy, such as seeing our anxiety specialist if needed, in addition to their primary therapist. Whatever is required to help the client, we attempt to provide. When new clients arrive at Castlewood we never know how his/her treatment will end up looking, because therapeutic strategies evolve as we get to know them and identify the pertinent factors that are contributory to the issues they present. Clients say this flexibility distinguishes Castlewood from prior treatments and often constitutes the difference that allows their recovery efforts to at last succeed.
- 5. EatingDisorders Eating Disorders constitute the most life-threatening category of mental health issues. eating disordersEating Disorders
- 6. Eating disorders often occur along with the compounding and further debilitating symptoms of depression, anxiety, addiction (to drugs or alcohol), perfectionism, and stress response syndromes. Family and friends may find aspects of the eating disorder perplexing in the tenacity of the hold it exerts on their loved one, the sufferer’s lack of awareness of their degree of debilitation over time, and the deception that can begin to enter once-honest relationships.
- 7. Eating Disorder can result as a symptom of many different syndromes with many developmental pathways. For some clients, there is fear of growing up and assuming adult responsibilities. For others, external functioning seems great while inside, they are confused, distressed and need a symptom to yell: help! Some become trapped in the role of pleasing others, perfectionism, and being the “good child”. For some clients, there was a major loss during childhood, such as a mother with post-partum depression or other experiences of separation from a key loved one. Others have experienced tremen- dous pain in their social interactions in school or with peers that has led to an ongoing sense of anxiety and isolation. Some clients’ families are themselves disengaged, without sufficient emotional connections, or shame-based with many intergenerational secrets and/or layers of unresolved intergenerational trauma. Some are enmeshed, without appropriate boundaries, resulting in overindulged children who get things rather than parenting. Some clients have perfect families, in appearance, and feel over- whelmed because they cannot live up to the parents’ perceived achievements or expectations. Once the eating disorder takes hold as a “survival strategy” of sorts, it can begin to take on a life of its own, as a recourse from, while simultaneously a perpetuator of, anxiety and isolation. As the illness progresses, various types of disequilibrium occur in mind and body, which cyclically, cause the individual to rely more heavily on the eating disorder symptoms to maintain an illusory sense of stability amidst the increasing chaos. As the cycle of the eating disorder continues, habituation results, as in any addiction, and it takes more of the same behavior to achieve the desired effect of feeling temporarily o.k. – more restriction, more food, more binging and purging, diet pills, laxatives, exercise, etc. When reliance on the eating disorder is discon- tinued, a client’s whole world can feel upside- down, out-of-control and initially, impossible to manage. This unfortunate, yet understandable predicament is what Castlewood exists to address. Our goal is to provide a container for the initial and inevitable distress, to provide the support of community, in lieu of that seemingly provided by the eating disorder, and to assist the client to learn and re-learn the skills necessary to stabilize and rebuild their lives. WHAT CAUSES EATING DISORDER?
- 8. Core Symptoms • Weight loss or gain with endocrine or metabolic abnormalities • Fat phobia/food phobia • Rituals around body checking, exercise and food • Purging (undoing and punishing) by fasting, vomiting, diuretics and exercise • Dissociation/lack of autonomy from craving and rituals/addiction • Body dissatisfaction, body image distortion • Binge eating, secretive eating, hoarding and stealing food • Chewing and spitting food as an attempt to control weight • Taking in excessive amounts of fluid or restricting fluid intake • Use or abuse of diet pills, herbal supplements or teas • Increased isolation, spending less and less time with family and friends • Refusing or avoiding eating with family and friends
- 9. Treatment Castlewood Treatment Center offers comprehensive and highly individualized treatment planning. The program is specifically designed to treat all types of eating disorders as well as co-existing disorders, including trauma, addictions, body dysmorphia, self-harm and other frequently co-occurring issues. treatment componentsComponents
- 10. EACH CLIENT RECEIVES: • A total of six sessions weekly with skilled and experienced clinicians. • Daily work with Dr. Mark Schwartz, and Lori Galperin, each nationally known for their clinical expertise, workshops and publications on eating disorder, childhood trauma and addictions. • Four individual sessions per week with the primary therapist. • A weekly session with his/her nutritionist who eats meals with clients. • A weekly session with our psychiatrist. • A small, well-chosen therapeutic community. • Levels of care that allow for increasing autonomy with continuing support • Excellent aftercare programming, including follow-up visits offered at Castlewood. Castlewood maintains a high staff-to- patient ratio providing for greater individualized care. Many of our clients have had treatment at other programs and have found recovery at Castlewood. Working with a qualified nutritionist, who has a solid background in eating disorders is the cornerstone of our program. Our residential nutritionist is a former eating disorder client herself and understands the process as only someone who has been through the recovery process can. Our therapy begins with a solid individual relationship with the primary therapist, psychiatrist and our nutritionist.
- 11. Residential Our Residential level of care is designed for stabilization and restoration of healthy eating habits. At the Residential level, we work to establish and foster a therapeutic community that can allow each client to feel supported and to work on building social connections while establishing a stronger sense of self. residential treatmentresidential
- 12. The Residential program only has a maximum of 10 clients. Each client sees his/her primary therapist four times a week as well as having weekly sessions with the dietician and the psychiatrist. The program itself consists of 40 hours of group therapy. Staff is on site 24/7. Each bedroom is attractive, uniquely decorated and has its own en suite bathroom. There are no more than two clients to a bedroom. Community space is likewise comfortable and inviting with inspiring views.
- 13. Thursday 7:30 – 8:00 Breakfast 8:15 – 9:15 Process Group 9:30 – 10:30 Core Group 10:30 – 11:00 Snack 11:00 – 12:00 Core Group II 12:30 – 1:30 Chef’s Choice 1:30 – 2:30 Pilates 3:00 – 3:30 Snack 3:30 – 4:30 Cognitive Group 4:30 – 6:00 Individual Sessions/Free Time 6:15 – 7:00 Dinner & Post Meal Free Time 9:00 – 9:30 Snack Friday 7:30 – 8:00 Breakfast 8:30 – 10:00 Core Group 10:00 – 10:30 Snack 10:30 – 12:15 Eating Disorder Group 12:30 – 1:30 Lunch & Post Meal 1:30 – 2:30 Body Image 2:30 – 3:00 Snack 3:00 – 4:30 Art Therapy 5:30 – 6:15 Dinner & Post Meal Movie Outing 9:00 – 9:30 Snack Saturday 7:30 – 8:00 Breakfast 8:15 – 9:30 Individual Sessions/Free Time 9:30 – 10:30 Gender Sexuality Intimacy & Relationships 10:30 – 11:00 Snack 11:00 – 12:00 Literary Interpretation/Shame Group 12:30 – 1:15 Lunch & Post Meal Outing & Visitors Free Time 9:00 – 9:30 Snack Sunday 7:30 – 8:00 Breakfast 8:00 – 10:30 Individual Sessions/Free Time 10:30 – 11:00 Snack 11:00 – 12:15 Music Therapy 12:30 – 1:15 Lunch & Post Meal Visitors & Passes 5:00 – 6:00 Addictions Group 6:15 – 7:00 Restaurant Outing or Family Style Meal Free Time 9:00 – 9:30 Snack Monday 7:30 – 8:00 Breakfast 8:30 – 10:30 Core Group Weekend Check-in & Goals 10:30 – 11:00 Snack 11:00 – 12:15 Core Group II 12:30 – 1:15 Lunch & Post Meal 1:30 – 3:00 Eating Disorder Group 3:00 – 3:30 Snack 3:30 – 4:30 Yoga Group 4:30 – 6:00 Individual Sessions/Free Time 6:15 – 7:00 Dinner & Post Meal Compulsory Play 9:00 – 9:30 Snack Tuesday 7:30 – 8:00 Breakfast 8:30 – 10:00 Core Group 10:00 – 10:30 Snack 10:30 – 12:00 Movement Group 12:30 – 1:15 Lunch & Post Meal 1:30 – 3:00 Expressive Therapy 3:00 – 3:30 Snack 3:30 – 4:30 DBT Group 4:30 – 6:00 Individual Sessions/Free Time 6:15 – 7:00 Dinner & Post Meal 7:15 – 8:15 Pre-Contract 9:00 – 9:30 Snack Wednesday 7:30 – 8:00 Breakfast 8:15 – 9:15 Eating Disorder Expressive Group 9:15 – 9:45 Menu Group 9:45 – 10:30 Nutrition Group 11:00 – 12:00 Treatment Module 12:30 – 1:15 Lunch & Post Meal 1:30 – 2:30 Sexual Healing or Containment 2:30 – 3:00 Snack 3:00 – 4:00 Eating Disorder Group 4:00 – 5:00 Relapse Prevention 5:00 – 6:00 Individual Sessions/Free Time 6:15 – 7:00 Dinner & Post Meal Compulsory Play 9:00 – 9:30 Snack Residential Program Weekly Schedule
- 14. The people at Castlewood Treatment Center saved my life. But they did more than that. They opened up my eyes to what life is all about, to all that I have to look forward to. I came in closed off from the world. The people here helped me find my strength. They didn’t just give me wings, they helped me find my own, and let me realize that I had the power to fly inside me all the time. I’m not just alive today because of the people here, but I’m actually living life as well. – MB ‘‘ ‘‘
- 15. Stepdown Our Step Down program is usually a transition from residential care. stepdownstepdown
- 16. The Stepdown program focuses less on stabili- zation and more on practice, with an emphasis on acquiring the necessary life skills to facilitate long-term recovery. Coping skills and healthy eating habits learned in residential are built upon and tried out in circumstances more closely resembling what clients will encounter post treatment. There is greater autonomy, encouragement of self responsibility, yet with help, support, guidance and community. We understand that each new phase in a client’s recovery process entails novel challenges. We endeavor to provide the feedback, opportunities, support and skill-building necessary to navigate each sequential hurdle. Our Stepdown nutritionist has successfully helped hundreds of clients nav- igate the pitfalls of eating in “the real world.” Again, this program is tailored to fit the indi- vidual’s situation. Some clients in Stepdown, will begin to work a certain number of hours, some to attend academic courses or to volunteer with local agencies or organizations. Learning to sustain a balanced lifestyle that includes: appropriate nutrition, work or school, supportive relationships, recreational activities and self-care simultaneously, is often a foreign concept con- trasted with how clients were functioning prior to treatment. The more opportunity to practice in this manner, the greater the odds for a sustained recovery post discharge. During the Stepdown phase, a meal and exer- cise plan is developed for the individual client by the nutritionist with client input and goals considered. Clients frequently say that our dietician and nutritionist are the BEST they’ve ever worked with. We consider this a supreme compliment and a variable that makes the process of recovery so much smoother!
- 17. DayTreatment day treatmentday treatment Castlewood offers a full spectrum of care. Our Day Treatment program is open to clients living in or around the St. Louis area who require more than outpatient treatment but who may be able to meet his/her treatment goals without a residential stay.
- 18. Day Treatment In order to achieve a level of stabilization and symptom reduction, some clients require a level of care beyond outpatient. Our Day Treatment program is provided for clients living in or around the St. Louis area who can commute to treatment and for whom an overnight stay is not a necessary treatment component. The program is available on either a 5- or 7-day basis. Clients become part of the therapeutic community and participate in all residential groups and programming. Depending upon whether in the 5 or 7 day version, clients receive 3-4 individual sessions with the primary therapist, one with the psychiatrist and one with his/her dietician weekly. Day Treatment is often the treatment of choice when a program of intensive outpatient care has not been adequate in effectively assisting the client to reach and/or maintain treatment goals.
- 19. Intensive Outpatient Our IOP Program is for clients needing more structure than individual outpatient therapy alone can provide or for the client who is transitioning back to life, work or school after treatment at a higher level of care, such as Residential or Stepdown. intensive outpatientIOP (intensive outpatient program)
- 20. Castlewood’s IOP Program consists of both group and individual therapy held four evenings each week. A supervised meal also comprises one facet of each evening’s programming. For motivated and less severely compromised clients, IOP may be the treatment of choice. There are four types of groups offered in the program. Castlewood Treatment Center offers a complete menu of outpatient services with expert individual therapists for eating disorders, nutritional counseling, marital and relational therapy and trauma-resolution therapy. For more information please call: 1-888-822-8938.
- 21. SKILLS GROUP The SKILLS GROUP is a structural psycho- educational group that provides clients with practical skills for coping with challenges and helps create alternative strategies to reliance on the eating disorder symptoms. Instead of binging and purging, utilization of self-sooth- ing, distraction, and problem solving. Instead of restricting, patients examine unhealthy thought processes, body image distortion and underlying feelings and needs. Clients are taught to use their voice rather than symptoms to communicate internal states and to facilitate problem solving, communication and to devel- op relationship skills and resources. The groups focus on body acceptance, behavior therapy, enhancing motivation, diminishing anxiety, appropriate nutrition, mindfulness, spirituality and self care. GENERAL PROCESS GROUPS The PROCESS GROUP allows an opportunity to discuss emotions and underlying dynamics that maintain eating-disorder symptoms. Feed- back from group members, particularly those farther along or those who have had similar experiences is useful. Assignments are often given to lend focus and assist clients in identification and exploration of symptom-maintaining cir- cumstances and issues. MEAL PROCESS GROUP In the MEAL PROCESS group, individuals are helped to recognize hunger and fullness, to learn to prepare or portion satisfying meals with variety, nutrition and in appropriate servings. The therapists eat with the clients, and clients are challenged and supported to confront their anxiety incrementally. EXPERIENTIAL GROUP In EXPERIENTIAL GROUP, clients deal directly with circumstances or situations having to do with body, movement and strong emotions. Clients often say these types of groups are the most challenging, but also the most useful. Clients may role play difficult situations to pro- vide insight and mastery. Through behavioral rehearsals, clients lessen anxiety and increase efficacy in dealing with new or challenging situations they face. Castlewood Program Coordinators (from left to right) Amy Kayda – IOP Coordinator & Therapist Emily Williams – Step Down Coordinator & Therapist Deanna James – Assistant Program Director & Therapist
- 22. SUPPORT GROUP Castlewood sponsors a free weekly sup- port group for people in recovery from Anorexia Nervosa, Bulimia and Binge Eating Disorder. The group is open to anyone regardless of stage of recovery. The purpose of the group is to establish a safe, reliable setting that emphasizes positive aspects of recovery. The format offers time for participants to briefly check in about the week, followed by an open discussion that focuses on various issues or topics that are common during the recovery process. Examples include: relapse prevention, negotiating boundaries, and utilizing healthy coping tools. Par- ticipation in support group requires that the individual be engaged in outpatient therapy, as the support group is not in- tended to replace on-going therapy or as a stand-alone form of support. Castlewood welcomes inquiries by both clients and therapists about appropriateness of the Support Group for you or for your client. Information about the Support Group is available from Nancy Albus at 636-386-6611. From the very first day I was warmly welcomed and though terrified I found support. The groups were extremely difficult but vital to my recovery. I formed friendships on a level I had never experienced before and found hope that had been covered by layers of fear. I can’t begin to explain the care that the staff at Castlewood had for me. At times it was overwhelming to think that anyone could care that much. From my relentless and kind therapist that helped me through my most difficult days, the psychiatrist that respected my every boundary, the directors who’s intuition still amazes me today, the staff who’s safety I remember when I was strug- gling the most, and let’s not forget the dieticians that I would have never imagined to be my biggest allies. With all of that, the structure of filled days of groups, the focus on the fear and trauma that was fueling my behaviors, and the many levels of step down I found my path to recovery. And most importantly I found myself. ‘‘ ‘‘ The groups were… vital to my recovery.
- 23. Trauma Resolution Clients need to return to the root of “what happened”… trauma resolutiontrauma resolution therapies
- 24. With one foot in the present and one foot in the past, the client re-examines the memories, re-associates the emotions, and changes the trauma-based or childhood attributions used to make meaning of the experience at the time to an adult perspective of enhanced clarity, wisdom and compassion. The event no longer exerts the same influence over behavior, choices and sense of self it did previously.
- 25. Unresolved experiences of child sexual abuse or rape, for example, will almost always result in symptoms. Where traumatically-originating symptoms prevail or complicate the individual’s ability to achieve a fuller recovery, therapies such as EMDR, Attachment-based Psychotherapy or Internal Family Systems therapy can be utilized to facilitate and speed up the necessary shifts in processing once some degree of safety, containment and stabilization exist. EMDR Clients who have suffered for years from anxiety or distressing memories, nightmares, insomnia, abuse or other traumatic events can often gain relief from a revolutionary therapy called EMDR (Eye Movement Desensitization Repro- cessing). Research shows that EMDR is rapid, safe and effective. EMDR does not involve the use of drugs or hypnosis. It is a simple, non-invasive patient-therapist collaboration in which healing can happen effectively. This powerful short-term therapy is highly effective for a wide range of disorders including chronic pain, phobias, depression, panic attacks, eating disorders and poor self-image, stress, worry, stage fright, performance anxiety, recovery from sexual abuse and traumatic incidents. Attachment-based PSYCHOTHERAPY When a client has experienced early attachment deficits with their caretakers in the first few years of life due to sensory hyperactivity or parental unavailability, they will evidence attachment dis- orders later in life. They will become dismissive of, or preoccupied with, securing love. So often, eating disorder results from a hunger for love, and the person is either too afraid to seek love (dismissive) or approaches partners with a binge mentality (preoccupied), or both (disorganized). Castlewood utilizes directive interventions to work with attachment difficulties.
- 26. INTERNAL FAMILY SYSTEMS THERAPY Internal Family Systems (IFS) therapy is a therapy that is very applicable to clients who have complex traumatic stress disorders and allows for a reworking of those experiences with one foot in the present, and one foot in the past. IFS has in common with Ego State therapies the idea that each individual has multiple selves or self-states. IFS, like Ego State therapies, is predicated on the notion that having self-states, (generally referred to as “parts”) is not (solely) a function of a dissociative process in need of therapeutic correction, but rather the normative state of all human beings. Working with these parts can be a very efficient and potent method of resolving past events and freeing the indi- vidual to rely more fully on his/her own innate capacities for change, growth and healing. Richard C. Schwartz, Ph.D., the originator of Internal Family Systems Therapy, is integral to Castlewood in both his training of our staff and as a clinical consultant.
- 27. Staff The staff at Castlewood is passionate. Their skill and dedication are surpassed only by their compassion for the hard work involved in each client’s process of recovery. castlewood staffcastlewood staff
- 28. Our therapists include highly trained master- and doctoral-level professionals with numerous specialties who are unequivocally committed to helping people heal. They understand the obsessive, often labyrinthine thought processes that create and maintain our clients’ cognitive distortions. Mark Schwartz, Sc.D. Clinical Co-Director Mark earned his doctorate in Psychology and Mental Health from Johns Hopkins University. He is a licensed psychologist and an adjunct professor in the departments of Psychiatry at St. Louis University School of Medicine. Over the past 25 years, Dr. Schwartz has achieved international recognition for his contribu- tions in a variety of clinical arenas including the treatment of intimacy disorders, marital and sexual dysfunction, sexual compulsivity, sexual trauma and eating disorders. He lectures nationally and internationally on these topics and has authored numerous articles and book chapters, as well as the books, Sexual Abuse and Eating Disorders and Sexual Compulsive Behavior, Sex and Gender. Dr. Schwartz is cur- rently on the Editorial Board of the Journal of Eating Disorders. Lori Galperin M.S.W., L.C.S.W. Clinical Co-Director Ms. Galperin initially earned her undergraduate degree in Psychology and later completed her gradu- ate degree in Clinical Social Work at Tulane University. She is an accomplished contributor in the fields of marital and sexual dysfunction, sexual compulsivity, sexual trauma, dissociative and eating disorders, lecturing nationally and internationally on these topics. She has au- thored various journal articles and book chapters, is trained in Clinical Hypnosis, EMDR, Internal Family Systems, Expressive and Attachment-based therapies. Over the past 22 years Ms. Galperin has treated several thousand inpatients and trained more than 100,000 clinicians throughout the United States, Canada and Europe. Nancy Albus M.Ed., L.P.C. Program Director Nancy earned her Master of Arts degree in Counsel- ing from the University of Missouri-St. Louis. She is a licensed Professional Counselor and trained in Internal Family Systems. In addition to her interest in eating disorders, Nancy works with femininity and sexuality issues, including facili- tating the Femininity and Sexuality group in Residential Treatment. Nancy joined Castlewood in 2002 as a therapist and is also the program director for the treatment center.
- 29. Theresa Chesnut M.S.W., L.C.S.W. Therapist Theresa initially earned her undergraduate degree in Family Life and Com- munity Services from Kansas State University and later completed her graduate degree in Clinical Social Work at the University of Kansas. Theresa has been on staff at Castlewood since 2000 and has held various positions: Primary Therapist, Program Director and currently as the Marketing Direc- tor. Theresa has also been on staff for the Menninger Clinic and she has over 15 years experience in lecturing on college campuses and to psychiatric professionals about the signs, symptoms and prevention of eating disorders. Currently, her area of research, focus and lecturing is on the recovery process and various intervention strategies as well as providing In- services for elite athletes, coaches and trainers. James Gerber M.A, A.T.R., Ph.D. Therapist Dr. Gerber earned a Masters Degree in Art Therapy/Counseling at Southern Illinois University, Edwardsville. He earned his Ph.D. at Saint Louis University in Counseling and Family Therapy. Dr. Gerber has worked extensively with adults and adolescents in a variety of clinical areas including sexual/marital dysfunc- tion, family therapy, sexual abuse, trauma and compulsivity. He has published and presented papers on sexual aggression, sexual abuse and trauma. Samantha Young M.Ed., L.P.C. Intake Coordinator/ Therapist Samantha Young earned a Masters of Science Degree in Counseling from Missouri Baptist University. She is a Licensed Professional Counselor and is trained in Internal Family Systems, Dialectical Be- havioral Therapy and EMDR. Samantha has worked at Castlewood Treatment Center since 2002 working with trauma and eating disorders. Deborah Hinds, D.T.R. Nutritionist Deborah earned her de- gree in Dietetic Technolo- gy with an emphasis in Nu- tritional Care at Florissant Valley College in Missouri. She is a registered and licensed Dietetic Tech- nician in the State of Missouri, and has experi- ence in clinical nutrition, outpatient counseling, mental health, and facilitating groups on eating disorders and addiction. Deborah is trained in the Internal Family Systems Model and has exclusively treated individuals with eating dis- order for nearly 10 years. Deborah works with residential, intensive outpatient, and outpatient clients to develop custom meal plans and to provide grocery shopping assistance and nutri- tional counseling.
- 30. Anna M. Jurec, M.D. Psychiatrist Anna M. Jurec, M.D. graduated from Medical Uni- versity in Gdansk, Poland and completed her Psychiatry Residency Program at Saint Louis University Department of Neurology and Psychiatry. She has been a member of the Ameri- can Psychiatric Association since 2004. She is cur- rently working as a full time psychiatrist at Castle- wood Residential Treatment Center. She is also a consultant with Places for People – a non-profit organization in St. Louis, treating severely and persistently mentally ill patients. “I enjoy helping to bring out the potential of the human mind in those affected by mental illness. I strive to treat the patient as an integral combination of body, mind and spirit and to allow patients to choose the best individual treatment based on scientific and clinical evidence. My particular professional interests are directed toward psychosomatic medicine (eating disorders in particular,) as well as mood and anxiety disorders.” Iness Panni, RN, MSN Nurse Manager Iness earned a Bachelor’s Degree in nursing from Avila University and a master’s degree in nursing from University of Kansas. Iness Panni has worked with eating disorders and addictions for over 25 years. She brings a special sensitivity to the medical, physical, emotional, psychological, social, and spiritual aspects involved in the complexity of treating eating disorders. As Nurse Manager of Castlewood Treatment Center since 2002, Iness provides a holistic oversight of the care and well being of each client. We chose Castlewood very carefully. When my daughter started I had hope, bits of optimism, and of course some relief in seeing her downward spiral arrested. Almost a month later I still felt those same things, but my daughter was voicing some optimism of her own. The degree to which the staff blend their roles/results/ perspectives, etc. for each client, including my daughter, is what returned her to life, and life to her. You were the reason she believed she might, then could, then would make it: and the strength she “borrowed” when hers wasn’t quite there. – DM ‘‘ ‘‘
- 31. WhyCastlewood A small Residential community fosters greater participation and affords more individualized treatment planning and care within a strong, cohesive therapeutic milieu. Castlewood is located just 25 minutes from St. Louis Lambert International Airport. In addition to state-of-the- art care, our facility, set in a tranquil, secluded environment, is a testimonial to the healing inherent in nature’s ever-renewing beauty. why castlewoodwhy castlewood
- 32. Unlike so many treatment centers, Castlewood helps clients heal the pain that underlies their eating disorders rather than just manage the symptoms. The place is beautiful, not just in it’s physical setting, but also in the compassionate way the staff views and relates to the clients. I wish I could send them all my traumatized clients, not just those with eating disorders. – Richard C. Schwartz, Ph.D. Developer of the Internal Family Systems model. ‘‘ ‘‘
- 33. 1. We are small. Only ten clients in-house with 33 staff permits highly individualized intensive treatment. We provide a great deal of support at the table and have locked access to food. 2. We individualize care. Whether you have obsessive-compulsive disor- der, body dysmorphic disorder, social anxiety disorder, major depression, multiple addictions or dissociative disorder, we provide specific treat- ment for the eating disorder as well as these often concurrent issues. 3. We specialize in trauma-resolution therapies. For clients with a history of childhood or adult trauma, we offer state of the art therapies for resolution of experiences that were overwhelm- ing. Trauma may consist of a one time incident that led to Post Traumatic Stress symptoms, or a series of developmentally prevalent occurrences that generated avoidance, constriction or reen- actment phenomena. 4. We utilize Internal Family Systems Therapy. All of our therapy staff have had training in Internal Family Systems therapy which allows us to work as a team to understand the contex- tual function of the individual’s eating disorder symptoms in order to help each client discover truly viable alternative survival strategies. 5. Our focus is more than simply re-feeding or control of symptoms. Our goal is to help launch a person in his/her development toward a full life. This includes support to transition to or re-enter college, job and relationship. 6. We provide a full continuum of care. We have found that almost all clients slip fol- lowing the support and safety of the in-house program. To allow clients more freedom and independence to practice recovery and rebound from the inevitable slips we began a Stepdown Program. It is a supportive environment where clients receive support from peers, implement relapse prevention plans and continue with his/ her individual therapy. We can further step a client down to Partial Hospitalization or the Intensive Outpatient Program to provide a full spectrum of recovery experiences alongside reintegration into daily life and activities. 7. We encourage family involvement whenever appropriate and possible. We schedule family weekends every 6-8 weeks, which involves the clients inviting all interested family members to 3 days of group and indi- vidualized treatment. Additional individualized family therapy and couples therapy with spouses or significant others are scheduled between Family Weekends as well, as it seems contribu- tory to the client’s overall treatment goals. 8. We create a safe environment. People with bulimia,binge eating disorder and/ or anorexia, are constantly punishing themselves internally with negative self talk. When working towards recovery,one needs people who under- stand this phenomenon and offer reflection with compassion rather than criticism. WHY CHOOSE CASTLEWOOD TREATMENT CENTER?
- 34. For the Professional Castlewood utilizes an evidence-based approach with 1-year follow-up with all clients. We have found that treatment effectiveness is highly dependent on: 1. Bringing the client from a premotivational to a motivational state. 2. Assessing psychiatric co-morbidity including OCD, social anxiety, body dysmorphia, co-addiction, post-traumatic stress disorder, and dissociaton. 3. Working with pertinent family dynamics, burdens the family carries intergenerationally that manifest in: over-control, over-indulgent enmeshment, engulfment or other addictive and secretive dynamics. Often, we need to have the entire family in for intensive work. 4. Couples work. A spouse, if not brought on board to what will be necessary to continue the recovery process, can unravel a great deal of even the most effective in-residence work. 5. Keeping a strong focus on food-related behav- ior and establishing control over out of control behavior, but not as part of a “good girl” over- compliancy but rather with a “real self,” honest and nonreactive stance toward relationships. 6. Looking for the deeper function of the symp- toms. There are good reasons each client de- velops an eating disorder. We don’t “get rid of ” the eating disorder, but instead help integrate a stronger self that no longer requires the illusion of control that comes from engagement in the eating disorder. 7. Integration. Our therapists and Treatment Team will involve the referring therapist in the treatment and recovery process. Let us know how you would like to be kept updated on your clients treatment and progress and we will provide you with the clinical information. 8. Addressing body image difficulties in both group therapy and in individual therapy through sensory exercises and experiential therapy. Clinicians help clients move toward connecting with his/her body and help them learn how to tolerate the connection. 9. Finally, a powerful relationship with the primary therapist and nutritionist, that allows for sufficient trust to incrementally let go of the eating disorder.
- 35. We invite you to compare program quality and costs and to call us for a telephone or in-person assessment and tour. Our intake coordinator, Samantha Young, can be reached at 1-888-822-8938. 800 Holland Road St. Louis, MO 63021 636-386-6611 phone 636-386-6622 fax 888-822-8938 toll-free www.castlewoodtc.com
- 36. 800 Holland Road St. Louis, MO 63021 phone 636.386.6611 toll-free 888-822-8938 fax 636-386-6622 www.castlewoodtc.com