
Empfohlen
Weitere ähnliche Inhalte
Was ist angesagt?
Was ist angesagt? (20)
Ähnlich wie Diptheria Final.pptx
Ähnlich wie Diptheria Final.pptx (20)
Mehr von bhavanibb
Mehr von bhavanibb (20)
Kürzlich hochgeladen
Kürzlich hochgeladen (20)
Diptheria Final.pptx
- 2. DIPHTHERIA • Is an acute infectious disease caused by toxigenic strains of Cornybacterium diphtheriae.
- 3. • The bacilli multiply locally, usually in the throat, and elaborate a powerful exotoxin which is responsible for the following pathology. • The formation of grayish or yellowish membrane (false membrane) commonly over the tonsils, pharynx, with well defined edges and the membrane cannot be wiped away. • Marked congestion, edema or local tissue destruction. • Enlargement of the regional lymph nodes. • Signs and symptoms of toxemia.
- 5. AGENT
- 6. • The causative agent, C diphtheriae is a gram-positive, non motile organism. • It has no invasive power, but produces a powerful exotoxin which can affect the heart leading to myocarditis.
- 7. • Four types of Diphtheria bacilli are differentiated. • gravis, mitis, belfanti and intermedius, all pathogenic to man.
- 8. SOURCE OF INFECTION • The source of infection may be a case or a carrier.
- 9. CASE • Cases range from subclinical infection to clinical cases. • Mild or silent infections may exhibit a mere running nose or sore throat. • These cases pose more threat in the spread than the active cases.
- 10. CARRIER • Carriers are common sources of infection. • Carriers may be temporary or chronic nasal or throat carriers.
- 11. INFECTIVE MATERIAL Nasopharyngeal secretions Discharges from skin lesions Contaminated fomites Infected dust.
- 12. INFECTIVITY • The period of infectivity may vary from 14 to 28 days from the onset of the disease. • But carriers may remain infective for much longer periods.
- 13. • A case or a carrier may be considered non communicable, when at least 2 cultures properly obtained from nose and throat, 24 hours apart are negative for diphtheria bacilli.
- 14. HOST FACTORS • AGE : Diphtheria particularly affects children (1-5 yrs). • GENDER : Both genders are affected.
- 15. IMMUNITY • Infants born of immune mothers are relatively immune during the first few months of life. • Children in developing countries seem to acquire active immunity through active infection.
- 16. ENVIRONMENTAL FACTORS Case of diphtheria occur in all seasons, although winter months favour its spread.
- 17. MODE OF TRANSMISSION • Droplet infection. • Transmitted directly to susceptible persons from infected cutaneous lesions. • Transmission by objects (cups, thermometers, toys, pencils) contaminated by the nasopharyngeal secretions of the patients is possible, but only for short periods.
- 18. PORTAL OF ENTRY • RESPIRATORY ROUTE : Commonly the portal of entry is the respiratory tract. • NON RESPIRATORY ROUTE : The portal of entry sometimes may be the skin where cuts, wounds and ulcers not properly attended to, may get infected with diphtheria bacilli.(umbilical cord) INCUBATION PERIOD • 2 To 6 days.
- 19. CLINICAL FEATURES Respiratory tract forms of diphtheria- pharyngo-tonsillar laryngo tracheal nasal combinations
- 20. Pharyngo-tonsillar diphtheria • Sore throat • Difficulty in swallowing • Low grade fever at presentation • Presence of pseudo membrane over tonsils • Oedema in sub mandibular region • Bull necked appearance
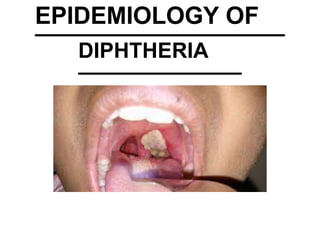
- 21. • Examination of the throat may show only mild erythema, localized exudate or a pseudomembrane. • The membrane may be a localized patch of the posterior pharynx or tonsil, may cover the entire tonsil, or less frequently, may spread to cover the soft palates and the posterior portion of the pharynx. • In the early stage the pseudo- membrane may be whitish and may wipe off easily. • The membrane may extend to become thick, blue- white to grey-black and adherent. • Attempts to remove the membrane may result in bleeding. • A minimal area of mucosal erythema surrounds the membrane.
- 22. PSEUDOMEMBRANE
- 24. • Patients with severe disease may have marked edema of the sub mandibular area and the antererior portion of the neck, along with lymphadenopathy, giving a characteristic • “bull- necked” appearance.
- 26. Laryngo-tracheal diphtheria • Preceeded by pharyngo tonsillar diphtheria • Fever, hoarseness and croupy cough • Dyspnoea • necrosis in heart muscles, liver, kidneys and adrenals • vision difficulties, speech, swallowing or movements of arms or legs • paralysis of soft palate, eye muscle or extremities Toxin damage • parenchymatous degeneration
- 27. • If the infection extends into the bronchial tree, it is the most severe of disease. • Prostration and dyspnoea soon follow because of the obstruction caused by the membrane. • This obstruction may even cause suffocation if not promptly relieved by intubation or tracheostomy. • The diphtheria bacilli within the membrane continue to produce toxin actively • This is absorbed and results in distant toxic damage, particularly paranchymatous degeneration, fatty infiltration and necrosis in heart muscle, liver, kidneys and adrenals and some time accompanied by gross hemorrhage.
- 28. • Irregularities of the cardiac rhythm indicate damage to the heart. • Later there may be difficulties with vision, speech, swallowing, or movement of the arms or legs. • The toxin also produces nerve damage, resulting in paralysis of the soft palate, eye muscles or extremities. • Patients who survive complications recover completely.
- 29. Nasal diphtheria • Mildest form • Localized in septum or turbinates of one side of nose • Conjunctiva and genitals also sources of infection • Membrane extends to pharynx.
- 30. Cutaneous diphtheria • Common in tropicalareas • Secondary infection of previous infection orskin abrasion • Presenting lesion-an ulcer surrounded by erythema and covered with membrane.
- 32. SCHICK’S TEST Intra dermal test Tests – presence of antitoxin(immunity status) and state of hypersensitivity to diphtheria toxin. Inject 0.2ml of Schick test toxin intradermally into skin of forearm, while into opposite arm- control (Schick toxin inactivated by heat) is injected.
- 33. Negative reactions if the person is immune, no reaction of any kind. Positive reaction In test arm, a circumscribed red flush of 10-50mm diameter appears within 24-36 hours reaching maximum development by 4th –7th day. This slowly fades into a brown patch and skin desquamates. Control arm shows no change. The person is susceptible to diphtheria.
- 34. Pseudo-positive reactions A red flush develops equally on both arms, much less circumscribed than true +vereactions. Fades by 4th day. allergic reaction found in certain individuals Schick negative Combined reactions Control arm shows pseudo positive reaction and test arm shows positive reaction. The person is susceptible to diphtheria.
- 38. • Start active search immediately from family and school contacts. • Carriers can be detected by culture methods. (swabs taken from nose and throat) CASES & CARRIERS Early detection Isolation all cases, suspected cases and carriers should be isolated, preferably in a hospital for atleast 14 days or until proved free of infection. 2 consecutive throat swabs taken 24 hours apart should be negative before terminating isolation.
- 39. Treatment- Cases • Preliminary test dose of 0.2 ml subcutaneously to detect sensitization to horse serum. • Followed by diphheria antitoxin IM or IV in doses ranging from 20,000-40,000 units or more depending on severity of cases. • Mild early pharyngeal or laryngeal: 20,000- 40,000 units • Moderate nasopharyngeal: 40,000-60,000 units • Severe, extensive or late disease: 80,000- 100,000 units. • Addition to antitoxin, penicillin or erythromycin for 5-6 days to clear throat. Carriers • Should be treated in 10days course of oral erythromycin
- 40. CONTACTS Should be throat swabbed and immunity should be determined. Where primary immunization was received within the previous 2 years- no further action needed. Where primary course or booster dose of diphtheria toxoid was received more than 2 years before, only a booster dose of dip: toxoid need be given. Non-immunized close contacts should receive prophylatic penicilin or erythromycin. They should be given 1000-2000 units of antitoxin and actively immunized againstdiphtheria.
- 41. COMMUNITY Active immunization with diphtheria toxoid of all infants as early in life as possible with subsequent booster dose every 10years thereafter. Immunization rate must be maintained at high level.
- 43. Combined vaccines • DPT • DTP(w) • DTP(a) • DT(d-tetanus toxoid) • dT(diphtheria-tetanus, adult type) single vaccines • FT(formal toxoid) • APT(alum-precipitated toxoid) • PTAP(purified toxoid- aluminium precipitate) • PTAH(p:t:a: hydroxide) • TAF(toxoid-anti toxin - flocculus) Antisera Diphtheria antitoxin
- 44. DPT VACCINE For immunization ofinfants. Pertussis component enhances diphtheria toxoid. Types- plain and adsorbed STORAGE should not befrozen Stored in refrigerator at 2-8 degree celsius Will loose potency if kept at room temperature for a long time.
- 45. Optimum age- DPT an be safely administered as early as 6 weeks after birth. Doses- 3 doses of DPT each is0.5ml. Mode of admn- injected intramuscular. DPT given in upper and outer quadrants of gluteal region.
- 46. Immunization schedule- 6 weeks 10weeks 14weeks 16-18months (booster dose) 5 years (DT)
- 47. Reactions- Fever and mild localreactions 2-6% develop fever of 39 degree or higher. 5-10% experience swelling and induration. Neurological- encephalitis, prolonged convulsions, infantile spasms, Reye’s syndrome. Contra indications- Seriously ill children or who need hospitalization are not vaccinated. Should not be repeated if a severe reaction occurred after a previousdose. In case of DPT, subsequent DT immunization.
- 48. For children over the age of 5 years who have not received DPT- 2 doses of DT vaccine, 4 weeks apart, with a booster dose 6 months to 1year later. Those children who received primary course of DPT earlier, should receive DT as booster at 5-6 years. For immunizing children over 12years of age and adults, preparation –dT (adult type diphtheria tetanus vaccine). Admn:- 2 doses at interval of 4-6 weeks, followed by booster 6-12 months after second dose.
- 49. ANTISERA Diphtheria antitoxin prepared in horse serum is still the mainstay of passive prophylaxis and also for treatment of diphtheria.
- 50. The End