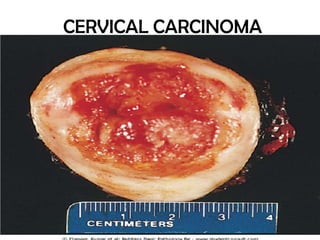
Cervical carcinoma
•Als PPTX, PDF herunterladen•
27 gefällt mir•8,106 views

This presentation is well approved by various professors of Gynecology.

Empfohlen
Weitere ähnliche Inhalte
Was ist angesagt?
Was ist angesagt? (20)
Andere mochten auch
Andere mochten auch (20)
Ähnlich wie Cervical carcinoma
Ähnlich wie Cervical carcinoma (20)
Kürzlich hochgeladen
Kürzlich hochgeladen (20)
Cervical carcinoma
- 2. • Common cancer, only next to Breast Cancer. • One of the major causes of cancer related deaths in women of age (35-45)years in developing countries. • Nearly all forms of carcinoma are Squamous cell Carcinoma.
- 3. PREDISPOSING RISK FACTORS • • • • • • Early age at first intercourse(18years) Multiple Sex Partners. Male partner with multiple previous sex partners. Persistent infection by Human Papilloma Virus. Poor personal Hygiene & socioeconomic status. STD, HIV infections, Herpes Simplex virus 2 infection or Condylomata. • Immunosuppresed Individuals, • Progesterone use over 8 years. • Smoking and drug abuse. Smegma is not carcinogenic. Spermatozoa may be carcinogenic because they provide DNA to cervical cells.
- 4. Pathogenesis Viral genome able to integrate into host genome & expess protein that inactivate tumor suppressor gene Viral genome unable to integrate into host genome
- 5. Definitions Dysplasia:- It is the disorderly but non neoplastic proliferation of normal cells resulting in atypical features, eg: -variation of cell size, shape and polarity. - alteration in nuclear cytoplasmic ratio. - large hyperchromatic nuclei with marginal condensation of chromatin material and mitotic figures. Metaplasia:- It is reversible change in which one adult cell is replaced by another type of cell for adaptation. Due to pH changes, hormonal effect infections and mutagens, Columnar epithelium of Squamocolumnar junction(Site of origin) transforms into Squamous cells. And this can be the precursor of Dysplasia and malignancy.
- 6. Dysplasia Mild Dysplasia (CIN-I) Moderate Dysplasia Severe Dysplasia (CIN-II) (CIN-III) Carcinoma in Situ LSIL According to Bethesda system HSIL HSIL confined to inner 1/3rd of epithlium occupy 50% of epithlial thickness occupy entire thickness of epithelium, with intact Basement membrane. Invasive Carcinoma beyond Basement Membrane
- 8. Invasive Cervical Carcinoma • Epidermoid Carcinoma -more common, 80%cases - arises from stratified squamous epithelium of cervix. May appear as proliferative/ulcerative/flat indurated areas. • Endocervical Carcinoma -less common -arises from mucous membrane endocervical canal - assosciated with use of OCPs and progesterone. - They remain confined to cervical canal for a long time causing barrel shaped enlargement of cervix, later they protrude from cervical canal.
- 9. Mode of Spread 1)Direct-i) Lateral – parametrium, Meckenrodts ligament, lateral pelvic wall. Uteteric obstruction ii) Inferiorly – upper part of the vagina, inguinal lymph nodes. iii) Superiorly – endometrium in 2-8 % cases. iv) Posteriorly – along uterosacral ligament in which sacral plexus is involved causing sciatica. Nerve sheaths and ureteric wall are not penetrated by cancer cells. Invasion to rectum is very rare because of Pouch of Douglas. 2.) LymphaticPrimary group of LN – paracervical, obturator, internal iliac & external iliac, sacral grp Secondary group of LN – common iliac, aortic, inguinal. Distant metastasis to lungs, CVS, 25-30%. Lymphatic spread is by embolism or by permeation. 3)Haematogenous spread –Contributes 5% Cancer cells invade the BVs but not erode them. Organs-lungs, liver, bone, kidney, brain.
- 10. Clinical Features SYMPTOMS - woman in 3rd and 4th decade of life. - Menstrual problems - irregular menses, menometrorrhagia. - continuous bleeding - post coital bleeding. - Vaginal Discharge -Is secondary to infection of the tissues or ulceration -Watery in nature which is initially white - Becomes yellowish & changes to dirty brown then blood stained -Odour due to saprophytic infection May be the only symptom of ca cervix.
- 11. Late symptoms are due to spread of disease -Renal – frequency, dysuria, hematuria, renal colic, urinary Incontinence because of fistula -Rectal – tenesmus, diarrhea, proctitis. -Pelvic symptoms – deep pelvic pain, low back ache, sciata, Swelling of the leg due to blockage of the lymphatics. -Terrible triad: sacral pain U/L lymphoedema of the leg U/L ureteric obstruction -Late & bad prognosis Anaemia, cachexia, anorexia, loss of weight
- 12. Signs Earliest sign on speculum -erosion - infected ulcer Ulcers - hardness, irregularity, bleeds on touch. Once the disease is established, 4 cardinal symptoms -induration -friability -fixity -bleed on touch Every lady with ca cervix a part from all clinical tests must undergo per rectal examination to find out any infiltration/thickness of the rectal mucosa.
- 13. Signs Late Lesions:1) Exophytic growth-papillary & polypoidal types – 95%, friable, cauliflower like lesion which has rough granular, hard surface which bleeds on touch. The lesion has got typical smell because of saprophytic infection. 2) Endophytic growth – could ulcerative or infiltrative or nodular. Uterus bulky due to pyometra in advanced stage, when cervix is blocked by growth. Rectal examination reveals thickened induration of uterosacral ligaments.
- 14. Complications: Pyometra Fistula. Ureteric obstruction-hydronephrosis, pyonephrosis Uraemia-because of infection & obstruction of renal system Cause of death in lady with ca cervix: Uraemia Cachexia Infections Complications of surgery Radiotherapy
- 15. Diagnosis • Pap Smear To reduce incidence of False Negative reporting following procedures are added to Pap Smear -- Endocervical scrape cytology – HPV testing by Hybridization or PCR. – Liquid Based Cytology. – Visual inspection of Acetowhite Areas (VIA) • Colposcopy directed Biopsy. • Cervicography. • Cone Biopsy.
- 16. Pap Smear • Screening test with Sensitivity:- 70-80% and Specificity:- 9598% • Offered to all women above 21 years of age who are sexually active for at least 3years.
- 17. Pap Smear Technique. To sample the ectocervix, a wooden spatula is placed against the external os and rotated 360 degrees. To sample the endocervix, a cytobrush is inserted into the external os and rotated. The sample obtained by the spatula and cytobrush is spread on a glass slide and immediately placed in a fixative, usually 95% ethanol, fixed for 30 minutes, and then stained with Papanicolaou stain. The sample is stained using the Papanicolau technique in which tinctorial dyes and acids are selectively retained by cells.
- 18. Cytology of CIN seen in Pap Smear Normal CIS-I CIS-II CIS-III There is Progressive reduction of size of Cytoplasm, and increase in Nuclear Cytoplasm Ratio as the grade of lesion progresses, which reflects there is loss of cellular differentiation on the surface of cervical lesion
- 20. False positive reporting - Infection, Inflammatory or reparative changes, and the effects of irradiation can result in atypical smear results suggestive, but not diagnostic, of CIN. - In these cases, smears should be repeated in 3–6 months.
- 21. If the Pap Smear is Negative: • It could be False Negative Reporting, 15-30% chances, so in such case Pap Smear is repeated annually for 3 consequtive years, and if still negative, then Pap Smear is repeated 3-5 yearly upto the age of 50 years. Pap test should not be done when a woman is menstruating, because endometrial cells can obscure cervical cells. But it can be performed during a woman's menstrual period, if the physician is using a liquid-based test.
- 22. Investigations.. 1) Liquid Based Cytology: Here, the plastic spatula(instead of wooden) is used which is placed in liquid fixative (buffered methanol), instead of directly smearing on a slide. This removes blood, mucus, and inflammatory cells. Suspended Cells are then sucked onto filter paper and then smear is made and stained on glass slide.
- 23. 2) Visual inspection of Acetowhite Areas (VIA) - done where the facilities for Pap Smear is not present. Procedure:- 5% acetic acid solution is applied on cervix, this dehydrates abnormal areas (high nuclear material and protein) turning them into acetowhite. Normal areas containing glycogen remain normal.
- 24. 5% acetic acid Acetowhite (abnormal) Schiller’s Iodine Cervix Unstained (Normal) Biopsy Visual Inspection of Acetowhite Areas (VIA) Mahogany Brown (Normal) Cervix Unstained (Abnormal) Biopsy Visual Inspection with Lugol’s Iodine (VILI)
- 25. Colposcopy • Colposcope is the instrument that is inserted into vagina and permits examination of cervix and upper part of vagina. Aims:- To study cervix when Pap Smear detects abnormal cells. - To locate abnormal areas. - To study extend of abnormal lesion. - To take Biopsy. - Conservative surgery following colposcopic guidance. - Follow up of conservative therapy cases.
- 26. Technique -Acetic acid (3.0% or 5.0%) is applied to the cervix. This removes mucus and dehydrates cells. The more protein in the cell, the whiter it becomes. Dysplastic cells contain large nuclei with abnormally large amounts of chromatin (protein). The application of acetic acid coagulates these intracellular proteins and makes them opaque and white. Hence, cells with an increased nucleus to cytoplasm ratio appear opaque on colposcopic examination.
- 27. Colposcope can visualise: - Acetowhite areas, - mosaics, - punctuations, - Abnormal vessels.
- 28. Pap Smear and Colposcopic Examination in Post Menopausal Women The test is often negative in them because of - dry vagina, senile vaginits - poor exfoliation of cells. - indrawing of squamocolumnar junction. So, oestrogen cream daily for 10 days or, 400µg misoprostol is used.
- 30. Other Investigations 1) Basic Investigations:- Hemogram, Urinalsis, Blood Sugar levels, LFT, RFT, serum electrolytes, ABO & Rh typing, cystoscopy, Chest Xray, ECG. 2) CT Scan and MRI: can detect Lymph Node Enlargment more than 1 cm. helps in Staging of tumor. 3) FDG-PET can detect lymphnode involvement can detect recurrence. Mechanism:- FDG accumulates in the malignant tissue because they exhibit greater glycolysis, resulting in increased tumour contrast. CT and MRI shows anatomical changes, PET shows Biochemical Changes in the tissues.
- 31. Staging of Cervical Carcinoma
- 33. <
- 34. Differential Diagnosis 1) CervicitiesInfectious or Noninfectious cervicitis. 2) Endometrial Carcinoma 3) Pelvic Inflammatory Disease. 4) Vaginitis. 5) Vaginal cancer. 6) Metastatic cancer to cervix (rare)
- 35. TREATMENT
- 36. Treatment of preinvasive(Stage 0)lesion 1) Local destructive • Cryotherapy -done for small lesions, OPD procedure w/o Analgesia -agents like N2O, CO2 are used, that causes crystallization of intracellular fluid. - Freeze-thaw-Freeze technique over 9 minutes. - least painful and cheap. - Advised to abstain from sexual intercourse for 4 weeks. - Side effects- Profuse Discharge, Uterine Spasms • Laser ablation - also an OPD procedure, done under Local Analgesia under colposcopic guidance. - converts cellular water to steam, and explodes the cells. - Minimal Bleeding, no infections, no scars, no indrawing of squamocolumnar junction.
- 37. 2) Local excision • • • • Conization with knife, laser LLETZ (Large Loop Excision of Transformation Zone) LEEP (Loop Electrosurgical Excision Procedure) NETZ (Needle Excision of Transformation Zone) -Done in immediate Postmenstrual phase, under Colposcopic view under Local Anesthesia. - preferred for young woman desiring future child birth. - can cause- stenosis of cervix, Abortion, Preterm labour.
- 38. 3) Radical excision • Hysterectomy - older and parous lady. - concurrent fibriods, DUB, or prolapse. - if microinvasion persists. - if recurrence occurs. - if lady cannot comply for followup
- 39. Management of CIN Pap smear Class I (normal) Repeat yearly for 3yr and then 3-5 yrly until 50yrs Class II (inflammatory) Class III CIN I (LSIL) Treat infection and repeat in 3 months Test for HPV and f/u yearly Normal f/u as class I Persistent repeat smear Normal Local Destruction •Coagulation •Cryosurgery •Laser ablation Lifelong follow up Local excision •Conization •Laser conization •LEEP Follow up Class IV Moderate, severe CIN II,III (HSIL) Class V Invasive carcinoma Biopsy, Rx acc. to stage Surgical or Radiation. Colposcopy and biopsy Persistent (Rx as HSIL) Radical excision •Conization •Hysterectomy with/out removal • of vaginal cuff Follow up
- 40. STAGE IA • Large loupe electrosurgical excision (best) -For preservation of reproduction. But tumor cell free margin is a must, with followup for 1 year. • Hysterectomy (abdominal/vaginal): choice of treatment because follow up in our setting is difficult.
- 41. STAGE IB-2A • Radical/Vaginal Hysterectomy • Wertheim’s hysterectomy (Thorough exploration of the abdomen, paraaortic LN biopsy, removal of the entire uterus, both adnexa, pelvic LN, medial 1/3 of the parametrium and upper 1/3 of the vagina) • Radiation following radical hysterectomy is needed if 1. Bulky lesion>4cm 2. deep stromal invasion 3. LN enlargement 4. margin of tissue show cancerous cell
- 42. STAGE IIB, IIIA, IIIB, IV Radiotherapy (traditional) -Goal is to achieve cytotoxic dose to cervical parametrium, pelvic nodes by external radiation. -Bladder and rectum should be protected. • In case of III b, intra cavity radiation along with external radiation. • Bulky irregular tissue should be treated with radiation
- 43. Concurrent chemotherapy is a radio sensitizer, & results in improved overall survival compared with radiation alone. Vs Surgical Therapy • Applicable only to stage I & Applicable to all stages of IIA. Carcinoma. • Requires Operation OPD procedure. Theatre. Ovaries cannot be preserved. • Accurate Surgical Staging is Vaginal Stenosis, fistula possible. formation occurs which are • Ovaries can be preserved. difficult to treat. • Concurrent uterine , Not applicable if Uterine or ovarian pathology can be ovarian pathology are treated. present. Radiotherapy • • • • •
- 44. 5year survival • • • • • CIN: good, >90% IB, IIA: 87-90% Stage III: 30-40% Stage IV:- 14% Survival is inversely related to the number and location of lymph node metastases, especially pelvic and para-aortic lymph nodes, Tumor size, staging and raised CEA level. • If chemotherapy is also used i.e cisplastin along with radiation better survival rate. • AdenoCarcinoma(1-5%): Treatment is radiotherapy.
- 45. FOLLOW UP • Every 3 mths for 1-2yrs because most Carcinoma cervix recur between 24-36 mths after treatment. • During follow up: total physical examinations including weight, - bimanual examination, - CXR, - USG pelvis, - Pap smear • After 3yrs of treatment: follow up every 6mths and after 5 yrs every year
- 46. RECURRENCE -Development of sciatic pain, lymphoedema, fistula are sure signs of Recurrence. -Radiotherapy- Treatment of choice. - Exenteration operation. - Anterior Exenteration. - Posterior Exenteration - Total Exenteration
- 47. Palliative Therapy • Pain relief with morphia(5-60mg) and tramadol. • Correction of vomiting and electrolyte imbalance. – Haloperidol 1.5-3mg - Metoclopramide, Domperidone and steroids • Diuretics and spironolactone for Ascites. • Betadine douche or metronidazole irrigation for vaginal discharge.
- 48. Prophylaxis -HPV vaccines are available now, expensive. -Given before the exposure to virus to adolescent before sexual activity begun. - confers 70% protection.