
Empfohlen
Weitere ähnliche Inhalte
Was ist angesagt?
Was ist angesagt? (20)
Ähnlich wie Diseases of pulp for ugs
Ähnlich wie Diseases of pulp for ugs (20)
Kürzlich hochgeladen
Kürzlich hochgeladen (20)
Diseases of pulp for ugs
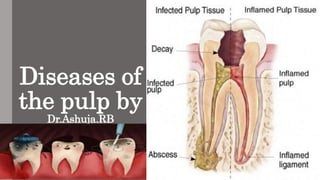
- 1. Diseases of the pulp by Dr.Ashuja.RB
- 2. • Introduction • Definition • Classification • Etiologic features • Reversible and irreversible • Acute pulpitis • Chronic pulpitis • Pulp polyp • Gangrene of pulp
- 3. Introduction: • Like other connective tissue pulp reacts with bacterial infection or the other irritant by inflammatory response. • Pulpitis is the most common lesion to produce. • A focal breach in this barrier can adversely affect the health of the dental pulp. • Inflammatory vascular changes increase the pulpal volume, but swelling is restricted due to the surrounding dentinal walls, often triggering pain.
- 4. Definition: Pulp: Soft tissue within pulp cavity, consisting of connective t issue containing blood vessels, nerves, and lymphatics, and at the periphery, layer of odontoblasts capable of in ternal deposition and repair of the dentin. Periapical: • Encompassing or surrounding the tip of the root of a tooth. Pulpitis : • Inflammation of the pulp of a tooth.
- 5. Clinically normal pulp • Clinically, a normal pulp exhibits no signs or symptoms that suggest pulpitis. • Teeth respond to cold with mild pain that resolves in 1 to 2 seconds, whereas heat is not associated with pulpal discomfort. • No pain on percussion. • Radiographic examination of the periradicular bone will be within normal limits.
- 6. History • During World War II in flying personnel,condition clinically simulating pulpitis by the incidence of toothache was reported - aerodontalgia. • Described in aircrew flying at high altitudes, astronauts, submarine crews, and in deep sea divers. • It is relatively uncommon and is associated particularly with recently filled teeth.
- 7. • The pain in decompression does not usually occur in normal pulps. • Some cases of pain localized to the dental area and resembling aerodontalgia have been reported to represent aerosinusitis and not to be related to the teeth.
- 8. Classification: 1. Depending on severity: • Acute and chronic 2. Depending upon the extent of involvement of pulp • Partial or focal pulpitis • Total pulpitis or generalized pulpitis 3. Based on the communication between pulp and oral environment • Open pulpitis (Pulpitis Aperta) • Closed pulpitis (Pulpitis Clausa)
- 9. Etiologic features: • Four main types of noxious stimuli are common causes of pulpal inflammation (pulpitis): 1.Mechanical damage: Traumatic accidents, iatrogenic damage from dental procedures, attrition, abrasion, and barometric changes. 2. Thermal injury: Cavity preparation, polishing, and exothermic chemical reactions of dental materials.
- 10. 3. Chemical irritation: Erosion or from the inappropriate use of acidic dental materials. 4. Bacterial effects: Bacteria can damage the pulp through toxins or directly after extension from caries or transportation via the vasculature.
- 11. • Anachoretic pulpitis: Bacteria circulating in the blood stream tend to settle out or accumulate at sites of pulpal inflammation, such as that which might follow some chemical or mechanical injury to the pulp. • Anachoresis is a phenomenon by which blood borne bacteria, dyes, pigments, metallic substances, foreign proteins, and other materials are attracted to the site of inflammation.
- 12. • Cause: Increased capillary permeability in the particular area. • Anachoretic pulpitis probably occurs in a clinically irrelevant number compared with the number of cases occurring as a result of dental caries.
- 13. Cracked tooth syndrome • In cracked tooth syndrome, a tooth, usually a restored premolar may split under masticatory stress. • These cracks are often minute and invisible clinically, and they allow the bacteria to enter into the pulp.
- 14. • Bacterial invasion may also occur as a result of a bacteremia and septicemia. • Pulpitis may rarely follow chronic periodontal disease wherein the microorganisms enter through the accessory canals of the exposed root surface especially through lateral canals infurcation areas of molars.
- 15. Reversible pulpitis • One of the earliest forms of pulpitis - focal reversible pulpitis. • Pulp hyperemia. • vascular dilatation can occur artefactually from the ‘pumping’ action during tooth extraction as well as pathologically as a result of dentinal and pulpal irritation. • Therefore, this early mild transient pulpitis, localized chiefly to the pulpal ends of irritated dentinal tubules, is now known as focal reversible pulpitis.
- 16. Clinical Features: • A tooth is sensitive to cold. • The application of ice or cold fluids pain. • Pain disappears upon removal of the thermal stimuli or restoration of the normal temperature. • Tooth responds to stimulation by the electric pulp tester at a lower level of current. • Deep carious lesion, large metallic restorations,or , restorations with defective margins.
- 17. Histologic Features: • Dilatation of the pulp vessels • Edema fluid may collect • Allowing actual extravasation of red blood cells or some diapedesis of white blood cells. • Thrombosis.
- 18. Treatment and Prognosis. • Reversible condition • The irritant is removed before the pulp is severely damaged. • Excavation of caries and restoration or a replacement of defective filling • If the primary cause is not corrected, extensive pulpitis subsequent ‘death’ of the pulp.
- 19. Irreversible pulpitis • Patients with early irreversible pulpitis generally have o sharp, severe pain on thermal stimulation, o pain continues for a longer period of time after the stimulus is removed. • Cold is especially uncomfortable, • Even heat or sweet and acidic foods also can elicit pain.
- 20. • Early stages o The pain often easily localized. o With increasing discomfort,unable to identify the offending tooth within a quadrant. o Although pulpal pain never crosses the midline,it can be referred from arch to arch, o In difficult cases, pulp testing of both arches.
- 21. • Late stages o The pain increases in intensity oAs a throbbing pressure that can keep patients awake at night. o At this point, heat increases the pain; however, cold may produce relief. oElectric pulp testing - at higher levels of current or demonstrates no response. o Mobility and sensitivity to percussion are usually absent. oIf pulpal drainage occurs ,symptoms may resolve if the
- 22. Histological features: • The dental pulp exhibits an area of fibrosis and chronic inflammation peripheral to the zone of abscess formation. Irreversible Pulpitis. Dental pulp exhibiting acute inflammatory infiltrate consisting predominantly of polymorphonuclearleukocytes.
- 23. Treatment: • Complete removal of pulp or pulpectomy • Placement of intracanal medicament • Extraction or root canal therapy
- 24. Features of reversible and irreversible pulpitis Reversible pulpitis Irreversible pulpitis Pain in short, sharp stabs Constant throbbing pain with sharp exacerbations Stimulated by cold as hot and cold or osmotic (sweet) stimuli. In late stages cold may relieve the pain Pain resolves after stimulus removed in seconds or a few minutes< 20 minutes duration Pain persists several minutes or hours after an exacerbating stimulus> 20 minutes duration Easily localized Difficult to localize Unaffected by position Affected by position
- 25. Acute pulpitis • Extensive acute inflammation of the dental pulp. • Frequent immediate sequela of focal reversible pulpitis. • It may also occur as an acute exacerbation of a chronic inflammatory process.
- 26. Causes: • Large carious lesion or restoration, • ‘Recurrent caries’. Clinical features: • Early stages o Involves only a portion of the pulp(beneath the carious lesion) o Severe pain is elicited by thermal changes, particularly to ice or cold drinks. o Pulpal pain is poorly localized. o Pain persists even after the thermal stimulus has disappeared or been removed.
- 27. Late stage: • The pain may become even more severe. • Pain - lancinating or throbbing type. • The pain generally lasts for 10–15 minutes but may be more or less continuous. • Teeth of the upper or lower jaw of the affected side. • Its intensity may be increased when the patient lies down. • The application of heat may cause an acute exacerbation of pain.
- 28. • The electric pulp vitality tester - lower level of current than adjacent normal teeth, indicating increased sensitivity of the pulp. • When necrosis of the pulp tissue occurs, this sensitivity is lost. • Severe pain - entrance to the diseased pulp is not wide open. • Severe acute pulpitis is extremely uncomfortable and at least mildly ill.
- 29. Histopathologic features: • Early acute pulpitis is characterized by the o Continued vascular dilatation seen in focal reversible pulpitis, oAccumulation of edema fluid in the connective tissue surrounding the tiny blood vessels. o Increased PML becomes apparent along the walls of these vascular channels, o leukocytes rapidly migrate through the endothelium lined structures.
- 30. • WBC are found in the inflamed region, beneath an area of carious penetration, the odontoblasts usually destroyed in this area. • The entire odontoblastic layer degenerates. • Entire pulp tissue undergoes rather rapid disintegration ,when there is closed pulp. • Numerous small abscesses may form.
- 31. • Eventually the entire pulp undergoes liquefaction and necrosis. • Acute suppurative pulpitis. • The pulp, especially in the later stages of pulpitis following carious invasion, contains large numbers of bacteria.
- 32. Treatment and prognosis: • Pulpotomy (removal of the coronal pulp) • Root canal treatment.
- 33. Chronic pulpitis • May arise on occasion through quiescence of a previous acute pulpitis. • But more frequently it occurs as the chronic type of disease from the onset. • The signs and symptoms are considerably milder than those in the acute form of the disease.
- 34. Clinical Features: • Pain o Not a prominent feature. o Even sometimes the patient complains of a mild, dull ache. o More often intermittent than continuous. • The reaction to thermal change is dramatically reduced in comparison to that in acute pulpitis. • The general features are not typical. • In the absence of significant symptoms, serious involvement of the pulp may be present.
- 35. • Even in wide-open carious lesions with open pulp, there is relatively little pain. • Bleeding may occur, pain is often absent. • Pulps may become totally necrotic without pain.
- 36. Histologic Features: • Chronic pulpitis is characterized by infiltration of the pulp tissue by varying numbers of mononuclear cells, chiefly lymphocytes and plasma cells and more vigorous connective tissue reaction. • Capillaries are usually prominent; • Fibroblastic activity is evident; • Collagen fibers arranged in bundles.
- 37. • Sometimes the pulp attempt to ward off the infection through deposition of collagen fibers around the inflamed area. • The tissue reaction may resemble the formation of granulation tissue on the surface of the pulp tissue in a wide- open exposure.
- 38. • With bacterial stains,microorganisms may be found in the pulp tissue, especially in the area of a carious exposure. • In some cases, the pulpal reaction fluctuates between an acute and a chronic phase.
- 39. Treatment and Prognosis: • Does not differ intensely from that of acute pulpitis. • Root canal therapy or extraction of the tooth.
- 40. Pulp polyp • Chronic hyperplastic pulpitis • A unique form of pulpitis • The inflamed pulp, instead of perishing by continued suppuration, reacts by excessive and exuberant proliferation. • It occurs either as a chronic lesion from the onset or as a chronic stage of a previously acute pulpitis.
- 41. Clinical features : • Children and young adults. • It involves teeth with large, open carious lesions. • Appears as a pinkish-red globule of tissue protruding from the pulp chamber.
- 42. • Deciduous molars and the first permanent molars. • Have an excellent blood supply. • Unusual proliferative property of the pulp tissue. • Tooth is asymptomatic except for a possible feeling of pressure when it is placed into masticatory function.
- 43. Histopathological features: • The surface may or may not be covered with stratified squamous epithelium, which migrates from the adjacent gingiva or arises from sloughed epithelium within the oral fluids. • The deeper pulp tissue within the canals typically shows fibrosis and a chronic inflammatory infiltrate. • Pulpal calcifications are common in both the radicular and coronal portions.
- 44. • Often the apical portion of the pulp tissue is normal with minimal inflammation or fibrosis. • The well-vascularized granulation tissue mass often becomes epithelialized, presumably by auto transplantation of epithelial cells from nearby mucosal surfaces.
- 45. Treatment: • Extraction of the tooth or by root canal therapy.
- 46. Gangrenous necrosis of pulp • Untreated pulpitis, either acute or chronic complete necrosis of the pulp tissue. • Generally associated with bacterial infection, the term pulp gangrene has sometimes been applied to this condition. • Gangrene being defined as necrosis of tissue with superimposed bacterial infection.
- 47. • Cause: sudden traumatic event, untreated irreversible pulpitis. • Infected pulpal necrosis: Dental decay Pain • Non infected pulp necrosis: No symptoms for many months.
- 48. • First sign in non infected : Discoloration of tooth due to result of the decomposing tissue debris and breakdown products of RBCs entering the open ends of the dentinal tubules and becoming distributed throughout the dentin. • After tooth is non vital - Tooth loses its ability to rehydrate the dentin, making it more brittle and subject to cracks and fracture.
- 49. • Associated with a foul odor • Diagnostic tool to determine pulpal necrosis – Percussion test • Gently tapping on several teeth in the area with a blunt instrument because pressure from tapping will produce intense pain.by this its easily identified if tooth has undergone pulpal necrosis.
- 50. • Necrosis of pulp has been reported in sickle cell anemia where there is blockage of pulp microcirculation by sickle erythrocytes . • Dry gangrene sometimes occurs when the pulp dies for some unexplained reason. • The nonvital pulp maintains its general histologic characteristics, being non purulent. • This condition may be due to some traumatic injury or infarct.
- 51. • Pulp gangrene should not be considered a specific form of pulp disease but simply the most complete end result of pulpitis in which there is total necrosis of tissue. • following blockage of the pulp microcirculation by sickled erythrocytes. • Associated with a foul odor when such infected pulps are opened for endodontic treatment. • Necrosis of pulp has been reported in sickle cell anemia where there is blockage of pulp microcirculation by sickle erythrocytes
- 52. Key features of pulpitis • Caused by infection or irritation of the pulp, usually by caries. • Severe stabbing pain in a tooth, triggered by hot or cold food or starting spontaneously, indicates acute irreversible pulpitis. • Pulp pain is poorly localized • Chronic pulpitis is often symptomless. • Untreated pulpitis usually leads to death of the pulp and spread of infection to the periapical tissues.
- 53. Treatment options for pulpitis: • If fractured or cracked, stabilise fracture and seal pulp temporarily. • Removal of caries, obtundent or steroid dressing • Removal of caries and pulp capping • Pulpotomy in deciduous teeth • Endodontic treatment • Extraction • Analgesics are largely ineffective.
- 54. Pulpitis pathway Normal pulp Injury Acute pulpitis Chronic pulpitis Pulp necrosis Periapical inflammation
- 55. Diagnostic techniques • History and nature of the pain • Reaction to thermal changes • Reaction to mild electric stimulation • Reaction to percussion of tooth • Radiograph examination • Visual examination • Palpation of surrounding area
- 56. Guess the diagnosis? 1. • Sharp intense pain • Pain is spontaneous • Sensitive to cold • Pain remains for 5 to 10 minutes. • Low level current responding by patient on electric pulp testing. • Pain disappears on removal of thermal irritant
- 58. 2. • Dull pain • Frequent pain • Sensitive to hot • Pain keeps patient awake at night on lying down to sleep • Difficult to localize the tooth. • Responds to higher level current on electric pulp testing • On removal of stimuli,pain lingers for longer time.
- 60. 3. • Patient may complain of growth of tissue on tooth • Painless • Discomfort while chewing • Children and young adults • Deciduous molars + 1st permanent molar • Clinically, open carious lesion and red globe like tissue protruding from tooth.
- 61. •Pulp polyp
- 62. 4. • Pain during chewing • Cracks on tooth surface • Large restoration or RCT treated teeth • No changes in radiograph.
Hinweis der Redaktion
- Pulpitis, if untreated, is often followed by death of the pulp and spread of infection through the apical foramen into the periapical tissues to cause periapical periodontitis.
- This pain has been attributed to the formation of nitrogen bubbles in the pulp tissue or vessels.
- Mechanical sources of injury include traumatic accidents, iatrogenic damage from dental procedures, attrition, abrasion, and barometric changes. Severe thermal stimuli can be transmitted through large uninsulated metallic restorations or may occur from such dental procedures as cavity preparation, polishing, and exothermic chemical reactions of dental materials.
- The pathways by which microorganisms may invade the pulp and periapical tissues: (1) from the apical foramen, (2) via the periodontal ligament and (3) via the blood stream (anachoresis).
- The significance of microorganisms in the etiology of pulpitis has been confirmed who produced surgical pulp exposures in germ-free rats. It was found that no devitalized pulps or periapical infections developed even when gross food impactions existed. By contrast, conventional animals rapidly developed complete pulpal necrosis.
- One of the earliest forms of pulpitis is the condition known as focal reversible pulpitis.
- Teeth in which this condition exists usually show deep carious lesion large metallic restorations (particularly without adequate insulation), or restorations with defective margins. It will be found also that such a tooth responds to stimulation by the electric pulp tester at a lower level of current, indicating a lower pain threshold (or a greater sensitivity) than that of adjacent normal teeth.
- Focal pulpitis is characterized microscopically Reversible Pulpitis. Dental pulp exhibiting hyperemia and edema. Edema fluid may collect because of damage to the capillary walls. The adjacent dentin was cut recently during placement of a dental restoration. Slowing of the blood flow and hemoconcentration due to transudation of fluid from the vessels conceivably could cause thrombosis.
- Mobility and sensitivity to percussion are usually absent because significant inflammation has not spread yet to the apical area. If pulpal drainage occurs (e.g., crown fracture, fistula formation), then the symptoms may resolve—only to return if the drainage ceases.
- Irreversible Pulpitis. Dental pulp exhibiting acute inflammatory infiltrate consisting predominantly of polymorphonuclearleukocytes. Irreversible Pulpitis. Same tooth as depicted in above pic. The dental pulp exhibits an area of fibrosis and chronic inflammation peripheral to the zone of abscess formation.
- Even in its early stages when the inflammatory reaction involves only a portion of the pulp, usually in the area just beneath the carious lesion, relatively severe pain is elicited by thermal changes, particularly when taking ice or cold drinks.
- and may be felt in any of the teeth of the upper or lower jaw of the affected side,.
- accumulation of edema fluid in the connective tissue surrounding the tiny blood vessels.
- The reaction to thermal change is dramatically reduced in comparison to that in acute pulpitis. Because of the degeneration of nerve tissue in the affected pulp, the threshold for stimulation by the electric pulp vitality tester is often increased.
- Bacterial products may act as antigens and the dendritic cells of the pulp capture the antigens, migrate to lymph nodes and present them to lymphocytes. These activated T cells then leave the lymphnodes and reach the pulp.
- Children and young adults who respond to proliferative lesions.
- Have an excellent blood supply because of the large root opening. The open chronic pulpitis an ample blood supply and the increased regenerative capacity of young pulpal tissue appears in some instances to stimulate the pulpal tissue to proliferate or to produce granulation tissue.
- The surface of the polyp may or may not be covered with stratified squamous epithelium, which migrates from the adjacent gingiva or arises from sloughed epithelium within the oral fluids.
- Chronically inflamed granulation tissue fills the coronal defect. Note surface stratified squamous epithelium.
- Since this is generally associated with bacterial infection, the term pulp gangrene has sometimes been applied to this condition,
- Discolor is due to result of the decomposing tissue debris and breakdown products of RBCs entering the open ends of the dentinal tubules and becoming distributed throughout the dentin. Tooth loses its ability to rehydrate the dentin, making it more brittle and subject to cracks and fracture. Gently tapping on several teeth in the area with a blunt instrument because pressure from tapping will produce intense pain.by this its easily identified if tooth has undergone pulpal necrosis.
- Pulp gangrene should not be considered a specific form of pulp disease but simply the most complete end result of pulpitis in which there is total necrosis of tissue. following blockage of the pulp microcirculation by sickled erythrocytes. Associated with a foul odor when such infected pulps are opened for endodontic treatment. Necrosis of pulp has been reported in sickle cell anemia where there is blockage of pulp microcirculation by sickle erythrocytes
- Nature n history: Duration n type of sensation, circumstances of its occurrences. Reversible – sharp, intense pain irreversible pain: dull,frequently vague in its location. Reaction to thermal changes: hot or cold Reversible: Immediate, sharp pain last for upto 20 mins Irreversible : dull pain lasts for much longer duration. Reaction to mild electric stimulation: Reversible : nerves will be easily excited so respond to lower than normal voltage level. Irreversible: nerve tissue within pulp is more severely damaged so higher level of voltage is required before the patient responds. Reaction to percussion of tooth: Positive reaction indicates inflammation in the apical periodontal tissue of a particular teeth in irreversible pulpitis Radiograph examination: Indicates irreversible changes within pulp. Determine the cause of vague pain in a quadrant of the mandible or maxilla. Visual examination: Reveal any expansion of cortical plates of alveolar bone.small nodule over the apex of thetooth represent opening of a draining sinus tract of apical abscess. Palpation of surrounding area Pain in patient signifies that inflammation has reached the tissue surrounding the apex of the tooth. Pulp is necrotic so pulp chamber need to be filled to prevent further spreading of inflammation to the surrounding bone.