
Empfohlen
Weitere ähnliche Inhalte
Was ist angesagt?
Was ist angesagt? (20)
Ähnlich wie Femoroplasty for Hip Fractures
Ähnlich wie Femoroplasty for Hip Fractures (20)
Mehr von Arun Shanbhag
Mehr von Arun Shanbhag (15)
Femoroplasty for Hip Fractures
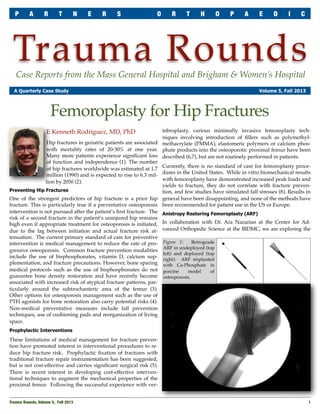
- 1. P A R T N E R S O R T H O P A E D I C Trauma Rounds Case Reports from the Mass General Hospital and Brigham & Women’s Hospital A Quarterly Case Study Volume 5, Fall 2013 Femoroplasty for Hip Fractures tebroplasty, various minimally invasive femoroplasty techniques involving introduction of fillers such as polymethylHip fractures in geriatric patients are associated methacrylate (PMMA), elastomeric polymers or calcium phoswith mortality rates of 20-30% at one year. phate products into the osteoporotic proximal femur have been Many more patients experience significant loss described (6,7), but are not routinely performed in patients. of function and independence (1). The number of hip fractures worldwide was estimated at 1.7 Currently, there is no standard of care for femoroplasty procemillion (1990) and is expected to rise to 6.3 mil- dures in the United States. While in vitro biomechanical results with femoroplasty have demonstrated increased peak loads and lion by 2050 (2). yields to fracture, they do not correlate with fracture prevenPreventing Hip Fractures tion, and few studies have simulated fall stresses (8). Results in One of the strongest predictors of hip fracture is a prior hip general have been disappointing, and none of the methods have fracture. This is particularly true if a preventative osteoporosis been recommended for patient use in the US or Europe. intervention is not pursued after the patient’s first fracture. The Anistropy Restoring Femoroplasty (ARF) risk of a second fracture in the patient’s uninjured hip remains high even if appropriate treatment for osteoporosis is initiated, In collaboration with Dr. Ara Nazarian at the Center for Addue to the lag between initiation and actual fracture risk at- vanced Orthopedic Science at the BIDMC, we are exploring the tenuation. The current primary standard of care for preventive Retrograde intervention is medical management to reduce the rate of pro- Figure 1: ARF in undeployed (top gressive osteoporosis. Common fracture prevention modalities left) and deployed (top include the use of bisphosphonates, vitamin D, calcium sup- right). ARF implanted plementation, and fracture precautions. However, bone sparing with Ca-Phosphate in medical protocols such as the use of bisphosphonates do not porcine model of guarantee bone density restoration and have recently become osteoporosis. associated with increased risk of atypical fracture patterns, particularly around the subtrochanteric area of the femur (3). Other options for osteoporosis management such as the use of PTH agonists for bone restoration also carry potential risks (4). Non-medical preventative measures include fall prevention techniques, use of cushioning pads and reorganization of living space. E Kenneth Rodriguez, MD, PhD Prophylactic Interventions These limitations of medical management for fracture prevention have promoted interest in interventional procedures to reduce hip fracture risk. Prophylactic fixation of fractures with traditional fracture repair instrumentation has been suggested, but is not cost-effective and carries significant surgical risk (5). There is recent interest in developing cost-effective interventional techniques to augment the mechanical properties of the proximal femur. Following the successful experience with verTrauma Rounds, Volume 5, Fall 2013 1
- 2. P A R T N E R S O R T H O P A E D I C T R A U M A R O U N D S Summary We envision ARF could be indicated for patients at high risk for hip fractures or as a procedure performed during the same surgical session on the intact contralateral side of a patient presenting for ORIF of a hip fracture. Kenneth Rodriguez, MD,PhD, is Chief of Orthopaedic Trauma at Beth Israel Deaconess Medical Center, Boston, MA. References Figure 2: Restoration of failure loads to controls levels in porcine model with ARF plus Ca-Phosphate. concept of Anisotropy Restoring Femoroplasty as a minimally invasive interventional option for hip fracture prevention. We have developed a technique and device that partially restores the material anisotropy of the proximal femur with a polymeric or Ca-phosphate filler. This composite structure, consisting of metallic elements embedded in an isotropic filler, restores both shear and axial energy dissipation potential to the proximal femur beyond what is possible with isotropic filling of the proximal femur. The technique allows for minimally invasive insertion of an antegrade ARF device from the greater trochanter combined with retrograde ARF device from the lesser trochanter, both interlinked within a Ca-phosphate (Ca-P) filled proximal femur, each inserted through separate 5 mm drill holes (Figure 1). We are presently testing a prototype device in a pig femur model (Figure 1) that has optimistic early results when compared with isotropic femoroplasty alone. Insertion of our ARF prototype device with calcium phosphate in a de-trabeculated pig femur model simulating osteopenic bone restores load to failure (Figure 2) and bone stiffness to control levels. Trauma Faculty Mark Vrahas, MD — 617-726-2943 1. Brauer CA, Incidence and mortality of hip fractures in the United States. JAMA, 2009; 302(14): 1573-9. 2. Gullberg B, Johnell O and Kanis JA, World-wide projections for hip fracture. Osteoporos Int, 1997; 7(5): 407-13. 3. Seraphim A, et al., Do bisphosphonates cause femoral insufficiency fractures? J Orthop Traumatol, 2012; 13(4): 171-7. 4. Augustine M and Horwitz MJ, Parathyroid Hormone and Parathyroid Hormone-Related Protein Analogs as Therapies for Osteoporosis. Curr Osteoporos Rep, 2013; Sep 28. 5. Faucett SC et al, Is prophylactic fixation a cost-effective method to prevent a future contralateral fragility hip fracture? J Orthop Trauma, 2010; 24(2): 65-74. 6. van der Steenhoven TJ, et al, Elastomer femoroplasty prevents hip fracture displacement In vitro biomechanical study comparing two minimal invasive femoroplasty techniques. Clin Biomech, 2011; 26(5): 464-9. 7. Strauss EJ, et al, Calcium phosphate cement augmentation of the femoral neck defect created after dynamic hip screw removal. J Orthop Trauma, 2007; 21(5): 295-300. 8. Sutter EG, Mears SC and Belkoff SM, A biomechanical evaluation of femoroplasty under simulated fall conditions. J Orthop Trauma, 2010; 24(2): 95-9. New England Regional Fracture Summit, Stowe, VT The annual AO Fracture Summit will be held January 17 – 20, 2014 in Stowe, VT. The highly interactive course is chaired by Drs. Mark Vrahas, Jesse Jupiter and Raymond White, and features several members of the Harvard Orthopaedic Trauma faculty. This year’s invited sage is Dr. David Helfet of the Hospital for Special Surgery, NY. The course is designed to educate community orthopedic surgeons who are actively involved in the treatment of patients with fractures. Participants are encouraged to bring their own cases for discussion. Registration is still open. For more information: www.aona.org AchesAndJoints.org/Trauma Read archives of all previous issues Jesse Jupiter, MD — 617-726-5100 Please share your comments online, or by email: MGH Hand & Upper Extremity Service Mark Vrahas, MD / mvrahas@partners.org Yawkey Center for Outpatient Care, Ste 3C 55 Fruit Street, Boston, MA 02114 Partners Chief of Orthopaedic Trauma mvrahas@partners.org jjupiter@partners.org Mitchel B Harris, MD — 617-732-5385 MGH Hand & Upper Extremity Service dring@partners.org Chief, BWH Orthopedic Trauma mbharris@partners.org R Malcolm Smith, MD, FRCS — 617-726-2794 Chief, MGH Orthopaedic Trauma rmsmith1@partners.org David Lhowe, MD — 617-724-2800 MGH Orthopaedic Trauma dlhowe@partners.org Michael Weaver, MD — 617-525-8088 BWH Orthopedic Trauma mjweaver@partners.org 2 David Ring, MD — 617-724-3953 Brandon E Earp, MD — 617-732-8064 BWH Hand & Upper Extremity Service bearp@partners.org George Dyer, MD — 617-732-6607 BWH Hand & Upper Extremity Service gdyer@partners.org Editor in Chief Mark Vrahas, MD Program Director Suzanne Morrison, MPH (617) 525-8876 smmorrison@partners.org Editor, Publisher John Kwon, MD — 617-643-5701 Arun Shanbhag, PhD, MBA MGH Foot & Ankle Service www.MassGeneral.org/ortho www.BrighamAndWomens.org/orthopedics jkwon@partners.org Trauma Rounds, Volume 5, Fall 2013