Thyroid hormones and thyroid inhibitors
•
2 gefällt mir•565 views

Synthesis, storage and release of thyroid hormone, thyroid and antithyroid drugs.

Empfohlen
Weitere ähnliche Inhalte
Was ist angesagt?
Was ist angesagt? (20)
Ähnlich wie Thyroid hormones and thyroid inhibitors
Ähnlich wie Thyroid hormones and thyroid inhibitors (20)
Mehr von Amit Kumar
Mehr von Amit Kumar (10)
Kürzlich hochgeladen
Kürzlich hochgeladen (20)
Thyroid hormones and thyroid inhibitors
- 1. THYROID HORMONES AND THYROID INHIBITORS
- 4. HORMONES SECRETED BY THYROID GLAND • Thyroxine ( T4 ) THYROID HORMONES • Triiodothyronine ( T3 ) • Calcitonin - interfollicular c cells
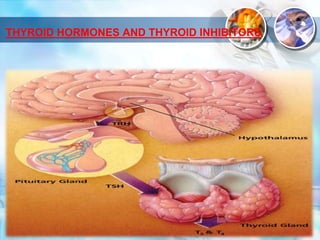
- 5. INTRODUCTION • The thyroid gland secretes 3 hormones – thyroxine (T4), triiodothyronine (T3) and calcitonin. • T3 and T4 are produced by the thyroid follicles under the influence of TSH secreted by the pituitary gland. • Calcitonin is produced by the parafollicular ‘C’ cells. It is important for calcium metabolism and is considered along with parathormone.
- 8. SYNTHESIS OF THYROID HORMONES 1. IODIDE UPTAKE 2. OXIDATION AND IODINATION 3. COUPLING 4. STORAGE AND RELEASE 5. PERIPHERAL CONVERSION OF T4 TO T3
- 10. IODIDE UPTAKE • The thyroid cells have an active transport process (Na+: I¯ symporter or NIS) • To concentrate iodide ion - pumps dietary I - into the cell • This trapping is stimulated by TSH • Rate –limiting step in thyroid hormone synthesis
- 11. OXIDATION • Iodide trapped by follicular cells is carried across the apical membrane by another transporter termed ‘pendrin’. • Oxidized by the membrane bound thyroid peroxidase enzyme with the help of H2O2 form iodinium (I+) ions
- 12. NIS P
- 13. IODINATION • These forms of iodine combine with tyrosil residues of thyroglobulin. • To form monoiodotyrosine (MIT) and diiodotyrosine (DIT).
- 14. COUPLING • MIT +DIT = T3 (Tri-iodothyronine) • DIT + DIT = T4 (Thyroxin) • All attached to thyroglobulin and stored in the colloid Thyroglobulin molecule • This process is stimulated by TSH
- 15. STORAGE AND RELEASE • Thyroglobulin containing iodinated tyrosil and thyronil residues is transported to the interior of the follicles by endocytosis and broken down by lysosomal proteases. • The T4 and T3 so released is secreted into circulation while MIT and DIT residues are deiodinated and the iodide released is reutilized.
- 16. CONT…. • The uptake of colloid and proteolysis are stimulated by TSH • Normal human thyroid secretes 60–90 μg of T4 and 10–30 μg of T3 daily.
- 17. NIS P
- 18. PERIPHERAL CONVERSION OF T4 TO T3 • Peripheral tissues, especially liver and kidney, convert T4 to T3. • About 1/3 of T4 secreted by thyroid undergoes this change and most of the T3 in plasma is derived from liver. • Target tissues take up T3 from circulation for their metabolic need, except brain and pituitary which take up T4 and convert it to T3 within their own cells.
- 19. ABSORPTION, TRANSPORT, METABOLISM AND EXCRETION • Oral bioavailability of l-thyroxine is ~ 75%, but severe hypothyroidism can reduce oral absorption. • It should be administered in empty stomach to avoid interference by food. • Sucralfate, iron, calcium and proton pump inhibitors also reduce l-thyroxine absorption. • Thyroid hormones are avidly bound to plasma proteins—only 0.03–0.08% of T4 and 0.2–0.5% of T3 are in the free form. • Binding occurs to 3 plasma proteins. In the order of affinity for T4, these are: (i.) Thyroxine binding globulin (TBG) (ii.) Thyroxine binding prealbumin (iii.) Albumin
- 20. CONT…. • Only the free hormone is available for action as well as for metabolism and excretion. • Metabolic inactivation of T4 and T3 occurs by deiodination and glucuronide /sulfate conjugation of the hormones. • CYP3A4 inducers like rifampin, phenytoin and carbamazepine accelerate metabolism of T4; dose of l-thyroxine may need enhancement. • Liver is the primary site (also salivary glands and kidneys). The conjugates are excreted in bile. • Plasma t½ of T4 is 6–7 days, while that of T3 is 1–2 days.
- 21. Relation between T4 and T3 • secretion of T4 more than T3, but in iodine deficient state T4 is reduced. • T4 is 15 times more tightly bound to plasma proteins While T3 is more tightly bound to the nuclear receptor . • T3 is 5 times more potent and acts faster acting while T4 less potent and slow acting. • Peak effect of T3 comes in 1–2 days while T4 takes 6–8 days. • About 1/3 of T4 is converted to T3 in the thyroid cells, liver and kidney by type 1 deiodinase (D1) and released into circulation. In addition, T3 is generated within the target cells (skeletal muscle, heart, brain, pituitary) by another type (D2) of deiodinase. • Thus, it may be concluded that T3 is the active hormone, while T4 is mainly a transport form; functions as a prohormone of T3. • Due to the fast action T3 is preferred in emergency (myxoedema coma) while due to the long acting T4 is preferred for long treatment required (hypothyroidism)
- 22. MOA
- 23. CONT…. ACTIONS 1.) Growth and development • T4 and T3 are essential for normal growth and development. • Congenital deficiency of T4 and T3 resulting in cretinism emphasizes their importance.
- 24. METABOLISM LIPID • T4 and T3 indirectly enhance lipolysis by potentiating the action of catecholamines and other lipolytic hormones • Plasma free fatty acid levels are elevated. • Thus, hyperthyroidism is characterized by hypocholesterolemia. • LDL levels in blood are reduced.
- 25. CONT…. • CARBOHYDRATE • Carbohydrate metabolism is also stimulated.
- 26. CONT…. • Protein Synthesis of certain proteins is increased • But the overall effect of T3 is catabolic— increased amounts of protein being used as energy source.
- 27. CONT…. CALORIGENESIS • T3 and T4 increase BMR by stimulation of cellular metabolism. • This is important for maintaining body temperature.
- 28. CONT…. CVS • Heart rate, contractility and output are increased resulting in a fast, bounding pulse. • BP, specially systolic, is often raised.
- 29. CONT…. SKELETAL MUSCLE • Muscles are flabby and weak in myxoedema, while thyrotoxicosis produces increased muscle tone, tremor and weakness due to myopathy. GIT • Propulsive activity of gut is increased by T3/T4. • Hypothyroid patients are often constipated, while diarrhoea is common in hyperthyroidism.
- 30. CONT… • HAEMOPOIESIS • Hypothyroid patients suffer from some degree of anaemia which is restored only by T4 treatment. • Thus, T4 appears to be facilitatory to erythropoiesis
- 31. CONT…. REPRODUCTION • Normal thyroid function is required for maintenance of pregnancy and lactation. • Fertility is impaired in hypothyroidism and women suffer from oligomenorrhoea.
- 32. THYROID DISORDERS • Hypothyroidism ↓ free T3 and T4 ↑ TSH • Hyperthyroidism ↑ free T3 and T4 ↓ TSH
- 33. USES 1. Cretinism – • It is due to failure of thyroid development or a defect in hormone synthesis or due to extreme iodine deficiency . • It is usually detected during infancy or childhood. • Treatment with thyroxine (8–12 μg/kg) daily should be started as early as possible, because mental retardation that has already ensued is only partially reversible.
- 36. CONT….. 2. Adult hypothyroidism • This is one of the commonest endocrine disorders • CAUSES - thyroiditis, thyroidectomy, severe iodine deficiency, or may be idiopathic. • Important drugs that can cause hypothyroidism are 131I, lithium and amiodarone. • Treatment with T4 - start with a low dose—50 μg of l thyroxine daily and increase every 2–3 weeks to an optimum of 100–200 μg/day (adjusted by clinical response and serum TSH levels).
- 37. Adult hypothyroidism Thyroiditis, thyroidectomy Severe iodine deficiency Idiopathic Drugs 50µg/day, ↑ to 100- 200µg
- 38. CONT…. 3. Myxoedema coma • It is an emergency; characterized by progressive mental deterioration due to acute hypothyroidism. • More common in old age associated with CAD may lead to angina and MI • Rapid thyroid replacement is crucial. • Though liothyronine (T3) acts faster, its use is attended by higher risk of cardiac arrhythmias, angina, etc. • Drug of choice is l-thyroxine (T4) 200– 500 μg i.v. followed by 100 μg i.v. OD till oral therapy can be instituted.
- 39. CONT….. 4. Nontoxic goiter • Iodine deficiency which may be accentuated by factors present in water excess calcium), food or milk (goitrin, thiocyanates). • A defect in hormone synthesis may be responsible for sporadic cases. • In both types, deficient production of thyroid hormone leads to excess TSH → thyroid enlarges. • Treatment with T4 • Endemic goiter due to iodine deficiency is preventable by ensuring daily ingestion of 150–200 μg of iodine. • This is best achieved by iodizing edible salt.
- 41. Cont…. • 5. Thyroid nodule • 6. Papillary carcinoma of thyroid • 7. Refractory anaemias. • 8. Menstrual disorders • 9. Chronic/non healing ulcers. • 10. Constipation.
- 42. DRUGS IN HYPERTHYROIDISM 1.) Inhibit hormone synthesis (Antithyroid drugs) Thioamides- e.g- Propylthiouracil, Carbimazole, Methimazole 2.) Inhibit iodide trapping (ionic inhibitors) Thiocynates, perchlorates, nitrates 3.) Inhibit hormone release Iodine, iodides of Na and K 4.) Destroy thyroid tissue Radioactive iodine
- 43. Thioamides (MOA) • Thioamides inhibits the enzyme thyroid peroxidase • Some report suggested that coupling reaction more sensitive then iodination. • Thioamides do not affect on other process but Propylthiouracil also inhibits the peripheral conversion of t4 to t3 by D1 and 5DI but not D2 (Brain, pituitary, hypothalamus, thyroid, brown fat, skeletal muscle)
- 44. NIS P
- 45. PHARMACOKINETICS • All antithyroid drugs are quickly absorbed orally. • Widely distributed and conc. In thyroid glands, Peak conc. Of Propylthiouracil is achieved in 1 hr. • Plasma half-life is shorter (75 min) but effect is longer due to the accumulation ( longer intrathyroid half life ). • Carbimazole convert into active metabolite methimazole which contribute longer action and 10 time more potent. • Cross the Placenta and secrete in milk (avoid in pregnancy and lactation) but Propylthiouracil less cross placenta & less secrete in milk (can be used if necessary) and strongly bound to the plasma protein. • Metabolized in liver and excreted in urine also secrete in milk.
- 48. Difference between Propylthiouracil Carbimazole
- 49. USES 1.) Antithyroid drugs control thyrotoxicosis in both Graves’ disease and toxic nodular goiter.(with propranolol not in CHF, Asthma) 2. For the preparation of pt for surgery of thyroid gland.
- 50. Advantages of antithyroid drugs over surgery are:- • No surgical risk, • No scar • no chances of injury to parathyroid glands or recurrent laryngeal nerve. • Hypothyroidism, if induced, is reversible. • Disadvantages are: • (a) Prolonged treatment is needed. • (b) relapse rate is high. • (c) Drug toxicity.
- 51. Oral dose schedule • Propylthiouracil- 50-150 mg TDS followed by maintenance dose 25-59 mg BD • Carbimazole- 5-15 mg TDS initially followed by maintenance dose 2.5- 10mg BD • Methimazole- 5-15 mg TDS initially followed by maintenance dose 2.5- 10mg BD or OD
- 52. ADVERSE EFFECTS • Hypothyroidism and goiter can occur due to overtreatment, but is reversible on stopping the drug. • Important side effects are: g.i.t intolerance, skin rashes and joint pain. • Loss or graying of hair, loss of taste, fever and liver damage are infrequent. • A rare but serious adverse effect is agranulocytosis (1 in 500 to 1000 cases). • It is mostly reversible.
- 53. IONIC INHIBITORS • Certain monovalent anions inhibit iodide trapping by NIS • Perchlorate is 10 times more potent than thiocyanate in blocking NIS, while nitrate is very weak. • They are toxic and not clinically used now. • Thiocyanates: can cause liver, kidney, bone marrow and brain toxicity. • Perchlorates: produce rashes, fever, aplastic anaemia, agranulocytosis.
- 54. IODIDES & IODINE • Oldest and fast acting agents for earlier control the hyperthyroidism. • Require for synthesis also for the inhibition of thyroid hormone(paradoxical effect) At low dose it stimulate the synthesis & at much higher dose inhibits the release of thyroid hormone.
- 55. MOA • by inhibiting thyroglobulin proteolysis. • Excess iodide inhibits its own transport into thyroid cells by interfering with expression of NIS on the cell membrane. • AT higher conc. It reduced the thyroid blood flow(use for preoperative preparation surgery and Thyrotoxicosis) • Some time acute inhibition of iodination of tyrosine resulting in reduced T3/T4 synthesis (Wolff-Chaikoff effect).
- 56. NIS P
- 57. CONT…. Uses: Preoperative preparation thyroid storms Prophylaxis of endemic goiter antiseptic
- 58. ADR • Acute reaction • It occurs in sensitive individuals only. • swelling of lips, eyelids, angioedema of larynx (may be dangerous), fever, joint pain, hemorrhages, thrombocytopenia, lymphadenopathy.
- 59. RADIOACTIVE IODINE • I-131- • I-123 - Used diagnostically • I-125
- 60. Uses • Diagnostic • Therapeutic Graves disease Toxic nodular goiter Palliative therapy for metastatic carcinoma of thyroid Contraindication in child and pregnancy
- 61. THANK YOU