Hand anatomy- harsh amin
•Als PPTX, PDF herunterladen•
13 gefällt mir•2,844 views

HAND ANATOMY , PLASTIC SURGERY

Empfohlen
Weitere ähnliche Inhalte
Was ist angesagt?
Was ist angesagt? (20)
Andere mochten auch
Andere mochten auch (20)
Ähnlich wie Hand anatomy- harsh amin
Ähnlich wie Hand anatomy- harsh amin (20)
Kürzlich hochgeladen
Kürzlich hochgeladen (20)
Hand anatomy- harsh amin
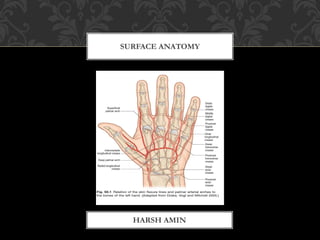
- 1. SURFACE ANATOMY HARSH AMIN
- 20. Clinical Significance. In contrast to the finger MCP joints, which should be immobilized in flexion to avoid contracture of the proper collateral ligaments, the PIP joints are immobilized in full extension to avoid irreversible contracture. The proper collateral ligaments at the PIP joints are under relatively uniform tension in flexion and extension and therefore are not a factor in irreversible contracture. However, the check-rein ligaments at the proximal end of the palmar plate at the PIP joint may hypertrophy and contract, resulting in a fixed flexion contracture.
- 34. THUMB The oblique pulley is the most important pulley in the thumb because the FPB can provide adequate and independent MCP joint flexion, and the A1 pulley often is released for stenosing tenosynovitis without apparent loss of function. The A2 pulley appears to be of no great practical significance if the oblique pulley is intact FINGER A1 is most imp. Following A4
- 36. These four branches, from proximal to distal, are called the branch to the vinculum longum, proximal transverse digital artery, interphalangeal transverse digital artery, and distal transverse digital artery
- 37. Clinical Significance of the Vascular Supply and the Vincular System of the Flexor Tendons in the Sheath This is illustrated by the following clinical examples: • Removal of the FDS for a tendon transfer is best performed proximal to or at the proximal edge of Camper's chiasma to preserve the VBS and the VLP. This may have the incidental side benefit of avoiding the potential for hyperextension deformity at the PIP joint in addition to the preservation of blood supply to the FDS and FDP. • Core intratendinous sutures are placed in the relatively avascular palmar aspect of the profundus tendon when practical. • The vincula may help to tether lacerated flexor tendons near their site of injury, but this also may give a falsenegative result when testing for tendon function. It has been suggested that the VBS at the PIP joint and the VBP at the DIP joint may play an accessory role in flexion because of their attachment to the palmar plate (113),
- 45. EXT TENDON: at middle proximal 1/3 proximal phalanx divide at PIP central slip joined by medial bands at PIP collaterals converge (on ulnar only interosseous/on radial both) at middle n distal 1/3 middle phalanx meet again INTEROSSEOUS: 4 attachment 3 contribution to ext.apperatus LUMBRICALS: 2 contribution SAGGITAL BAND: arciform covers its distal half common attatchment with arciform saggital band taught when MP fully flexed make central slip central/hyperextend MP n also limit the same ARCIFORM: proximally only from interosseous distaly 2 layer-sup. From interosseous /Deep from collateral band through arciform sheet interosseous flexes MP and extend PIP and lateral deviation. centralise EDC
- 49. TRIANGULAR LIG.: proximal ½ middle phalanx TRANSEVERSE LIG.: continuation from triangular to palmar plate PIP and A4 cover collateral lig. And PIP OBLIQUE LIG.: from prox.phalanx and A2 pully near neck of proximal phalanx at PIP volar to joint axes courses over both PIP and DIP so whe PIP extend ligament tight so DIP flexion difficult n vise versa. volar to PIP so pravent its hyperextension
- 52. 1. Experimentally, when the tendon of the extensor digitorum (ED) is retracted and the intrinsics are severed, the finger becomes hyperextended at the MP joint and flexed at the PIP and DIP joints, assuming a clawlike position. Flexion of the PIP and DIP joints results from the natural tone of the flexors. This position may be manifested by paralysis of the ulnar nenre and loss of intrinsic function If the flexor tendons are now divided, the PIP and DIP joints may be extended 2. When the MP joint is hyperextended, the palmar plate moves distally and the sagittal bands then become tightened. This restrains the extensor tendon and prevents it from moving proximally . If the sagittal bands are surgically divided, the extensor tendon may further extend the PIP and DIP joints 3. When the MP joint is in the neutral position, the sagittal bands are loose, allowing the extensor tendon to continue extending the PIP and DIP joints. Any limitation of hyperextension of the MP joint, such as by physiologic force of the intrinsics or by a static tenodesis, may improve extension of the PIP and DIP joints. This mechanism has been used in management of claw deformity due to a paralyzed ulnar nenre
- 53. Winslow's Diamond In 1746, Winslow described "a tendinous rhombus“ formed by splitting and reuniting the collateral bands of the extensor tendon over and in the vicinity of the PIP joint. Winslow's diamond is maintained statically by the triangular ligament and transverse retinacular ligament and dynamically by the lateral tendinous slips of the intrinsics, which join the collateral bands of the extensor tendon on the sides of the PIP joints. When the PIP joint is flexed, Winslow's diamond is widened and the lateral bands glide slightly palmarly and become slack. In this situation, the DIP joint can not be actively extended-the so-called floating distal phalanx. Normally, palmar gliding of the lateral bands of the extensor tendon never descends below the transverse axis of the PIP joint. In a swan-neck deformity, Winslow's diamond becomes narrower, whereas in a boutonniere deformity, it is widened so that the collateral bands pass palmar to the transverse axis of the PIP joint.
- 58. BLOOD VESSELS
- 67. NERVES
- 73. NAILS
- 76. SKIN & RETICULATA & APONEUROSIS
- 90. CROSS SECTION
- 99. FUNCTIONS
Hinweis der Redaktion
- EXT TENDON:at middle proximal 1/3 devide at PIP central slip joined by medial bands at PIP collaterals converge (on ulnar only interosseous/on radial both) at middle n distal 1/3 meet again