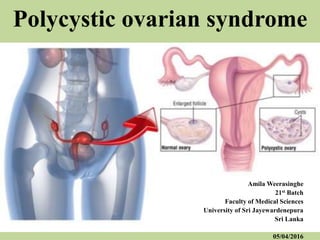
Polycystic ovarian syndrome
•Als PPTX, PDF herunterladen•
87 gefällt mir•5,450 views

Polycystic ovarian syndrome (PCOS) is a condition of unexplained hyperandrogenic chronic anovulation that most likely represents a heterogenous disorder. About 10% of women in the reproductive age group suffer from this disorder.

Empfohlen
Weitere ähnliche Inhalte
Was ist angesagt?
Was ist angesagt? (20)
Andere mochten auch
Andere mochten auch (20)
Ähnlich wie Polycystic ovarian syndrome
Ähnlich wie Polycystic ovarian syndrome (20)
Kürzlich hochgeladen
Kürzlich hochgeladen (20)
Polycystic ovarian syndrome
- 1. Polycystic ovarian syndrome Amila Weerasinghe 21st Batch Faculty of Medical Sciences University of Sri Jayewardenepura Sri Lanka 05/04/2016
- 2. Objectives 1. Introduction 2. Aetiology 3. Clinical features 4. Diagnosis 5. Management 6. Outcomes
- 3. 1. Introduction • A syndrome of ovarian dysfunction with cardinal features of hyperandrogenism polycystic ovary morphology • Often complicated by chronic anovulatory infertility • Clinical manifestations include oligomenorrhoea, hirsutism and acne
- 4. • Many women are obese and have a higher prevalence of impaired glucose tolerance, type 2 diabetes and sleep apnoea • They exhibit an adverse cardiovascular risk profile.
- 5. • Cardiometabolic syndrome as suggested by a higher reported incidence of , hypertension dyslipidaemia visceral obesity insulin resistance hyperinsulinaemia
- 6. • Prevalence - 5 – 10 % of women of reproductive age • The commonest cause for anovulation (80%) • USS evidence of polycystic ovaries in 20-30 % of women • The most common endocrine disorder in women
- 8. High risk groups • Women with oligo ovulatory infertility • Obesity and/or insulin resistance • Type 1 , type 2 or gestational diabetes mellitus • A history of premature adrenarche • First-degree relatives with PCOS • Women using antiepileptic drugs (valproate)
- 9. 2. Aetiology • Not fully known • No gene or specific environmental substance has been identified. • Genetic studies showed a link between PCOS and metabolic disturbances such as disordered insulin metabolism. • Hence it may be a manifestation of a complex genetic disorder.
- 10. • Selective insulin resistance may be central to the aetiology of PCOS. • Compensatory hyperinsulinaemia • Decreased levels of serum hormone binding globulin (SHBG) • Trophic stimulus to androgen production in the adrenals and ovaries • Direct effect on the hypothalamus causing abnormally stimulated appetite and increased gonadotropin secretion
- 11. • Hypersecretion of LH Stimulation of androgen secretion from ovarian thecal cells • Elevated LH : FSH ratio
- 12. 3.Clinical features • Oligomenorrhoea / amenorrhoea - 75% • Hirsutism • Subfertility 75% • Obesity 40% • Recurrent miscarriage 50 – 60% • Acanthosis nigricans • Asymptomatic
- 17. 4.Diagnosis 2 out of 3 features of Rotterdam criteria • Amenorrhoea/oligomenorrhoea (cycle >42 days) • Clinical or biochemical hyperandrogenism ( acne, hirsutism,alopecia ) • Polycystic ovaries on ultrasound ( 8 or more subcapsular follicular cysts <10mm in diameter and increased ovarian stroma)
- 18. USS • Bilateral enlargement of the ovaries > 8.0 cm. Increased ovarian volume ( >10ml ). • Thickened tunica albugenea • Multiple small cysts (12 foliclles or lesser) of 0.2-0.9 cms in each ovary • Absence of dominant follicle • Thickened stroma (hyperthecosis) • Resting or follicular endometrium
- 21. Laboratory investigations: • Demonstration of biochemical hyperandrogenaemia. – Total testosterone (>200ng/dL)/ Free testosterone > 2.2pg/mL. • S. Estradiol and FSH estimations. – Exclude hypogonadotropic hypogonadism ( E2, FSH). – Exclude premature ovarian failure ( E2, FSH).
- 22. • S. Dehydroepiandrosterone sulfate. – Not of value if S. Testosterone is normal – Values > 430μg/dL significant. It is indicative of adrenal source of androgens. – Levels > 700 μg/mL suggestive of androgen producing adrenal tumour. • 24 hours urinary cortisol – Cortisil < 50 μg/24 hours – Exclude Cushing’s syndrome if patient is hypertensive.
- 23. Exclusion of other causes of hyperandrogenism. – Estimation of TSH to exclude thyroid dysfunction – Estimation of serum prolactin to exclude hyperprolactinemia – Estimation of 17α hydroxyprogesterone. Non classical congenital adrenal hyperplasia caused by 21-hydoxylase deficiency.
- 24. – Consider screening for Cushing’s syndrome, and – Rare conditions like acromegaly. – Evaluation for metabolic syndrome X.
- 25. 5. Management Treatment goals of polycystic ovary syndrome: – Prevent endometrial hyperplasia, atypia/ cancer – Restore normal ovulation / fertility – Restore normal menstruation – Correct hirsutism
- 26. Aspects of management 1. Lifestyle modification 2. Improving menstrual regularity 3. Controlling symptoms of hyperandrogenism 4. Subfertility 5. Insulin sensitizers 6. Psychological issues
- 27. 1.Lifestyle modification • Weight reduction through exercise and diet – the most important step in managing overweight women. • Even a modest weight loss (5%) can improve symptoms. • Effective in restoring ovulatory cycles and achieving pregnancy.
- 31. 2. Improving menstrual regularity • Weight loss • Combine oral contraceptive pills (COCP) inhibits LH Reduces circulating androgens increases circulating SHBG Low dose combination pill containing low dose of synthetic estrogen in combination with a low- androgenic progestin
- 32. • Metformin Benificial in patients with hyperinsulinaemia and CVS risk factors. Improves peripheral insulin sensitivity; improve ovulation rates improve glucose tolerance increased SHBG leading to reduced bioavailability of androgens
- 33. 3. Controlling symptoms of hyperandrogenism • Mainly hirsutism 1st line treatment Weight reduction COCP Medroxyprogesterone acetate
- 34. 2nd line treatment Spironolactone Cyproterone acetate Finasteride Flutamide Eflornithine hydrochloride GnRH agonists Last resort Ketoconazole
- 35. Cosmetic approaches Permenent Laser Electrolysis Non-permanent Local chemical depilatories Bleaching Waxing Tweezing Mechanical epilators
- 36. 4. Subfertility • Weight loss • Ovulation induction with antioestrogens or gonadotrophins Clomiphene citrate Is a selective estrogen receptor modulator 1st line treatment in women with PCOS and anovulatory infertility Ovulation rate 70-80 % Pregnancy rate 30-40 % over 6 cycles
- 37. • Laparoscopic ovarian diathermy Effective in patients who are resistant to clomiphine.
- 38. • In vitro fertilization ( IVF ) when ovulation can’t be achieved; or doesn’t succeed in pregnancy.
- 40. 5. Insulin sensitizers Metformin • Metformin combined with clomiphene citrate increases ovulation and pregnancy rates. • No significant increase in birth rate. • No significant improvement in acne or hirsutism. • Lowers androgen levels.
- 41. 6. Psychological issues • Symptoms can be distressing and resulting lower self esteem. • Holistic approach
- 42. Definite / common consequences of PCOS • Insulin resistance: Type-II diabetes • Endometrial hyperplasia / atypia • Gestational diabetes • Sleep apnoea
- 43. Possible consequences of PCOS • Hypertension • Coronary heart disease • Dyslipidemia • ? Risk of ovarian cancer • ? Risk of abortion
- 44. Summary
Hinweis der Redaktion
- 80 % from oxford hand book Cardiometabolic syndrome (CMS) is a clustering of interrelated risk factors that promote the development of atherosclerotic vascular disease and type 2 diabetes mellitus.
- Cardiometabolic syndrome (CMS) is a clustering of interrelated risk factors that promote the development of atherosclerotic vascular disease and type 2 diabetes mellitus
- BMI >30 in 35-60% of women with PCOS Obesity worsens insulin resistance. (The best evidence comes from a meta-analysis of 11 studies demonstrating a twofold excess risk of developing PCOS in 556 women treated with valproate compared with 593 women treated with other antiepileptic drugs)
- does not prevent insulin effect on its receptors on the ovary, or the effect on insulin SHBG and the hepatic production of insulin growth factor-1 (IGF-1)
- The main effect of insulin on the ovaries is not only to increase androgen production, but also to derange the regulation of androgen synthesis so as to prevent the down regulation of the LH receptors leading to increased production of androgens and estrone which coupled with insulin effect of lowering SHBG leads to hyperestrogenism and reduced FSH levels.
- Estimation of 17α hydroxyprogesterone. Random normal level < 4 ng/ml. Fasting < 2 ng/ml.
- Improving insulin sensitivity is associated with improved ovulation rates, improved glucose tolerance and increased SHBG leading to reduced bioavailibility of androgens. Sex hormone binding blobulin
- Causes increasing cervical mucus thickening and also exhibits its anti-estrogenic effect on the endometrial lining; thereby negating any benefits of ovulation should it occur.. generally started at a dose of 50 mg/day starting from day 2 - day 6 of the period. If treated for more than 12months risk of endometrial CA