2. Although the superiority of biphasic over monophasic
waveforms is well established,7–15
the relative efficacy and
safety of the available biphasic waveforms is less clear. In
addition, the optimal starting energy for biphasic direct-
current cardioversion of AF is not established. This pro-
spective, randomized single-center study was undertaken to
compare the effectiveness and safety of two clinically avail-
able distinct biphasic waveforms for external direct-current
cardioversion of AF.
Methods
The study was approved by the Mayo Foundation Institu-
tional Review Board. All procedures used in this study were
in accordance with Mayo Clinic Cardioversion Unit practice
guidelines. All patients gave written informed consent. This
investigator-initiated study was funded completely by the
Mayo Foundation, without any commercial support or com-
mercial data analysis.
Patient selection and anticoagulation
Between March 2002 and June 2003, patients who un-
derwent direct-current cardioversion of AF at Saint Marys
Hospital in Rochester, Minnesota, were eligible for enroll-
ment unless they met specific exclusion criteria. Patients
were excluded from the study if they were younger than 18
years, were pregnant, had a known contraindication for
conscious sedation or for cardioversion, were unable or
unwilling to provide informed consent, or already were
enrolled in another clinical study. Patients with atrial flutter
or supraventricular arrhythmias other than AF were not
eligible for this study. ECG strips recorded within 1 minute
before cardioversion were blindly reviewed by two senior
investigators (PAF and SCH) to exclude atrial flutter or
other organized arrhythmia. In case of discrepancy, a third
blinded reviewer adjudicated (BJG). Overall, 188 patients
were prospectively randomized. Data, which included age,
gender, height, weight, body mass index, type of heart
disease, use of antiarrhythmic medication, duration of AF
prior to direct-current cardioversion, left ventricular ejec-
tion fraction, and presence of diabetes mellitus or hyperten-
sion, were prospectively collected at enrollment.
Patients with AF for Յ48 hours known to be taking
therapeutic heparin within 48 hours of AF onset were car-
dioverted immediately.16
If the patient was not anticoagu-
lated, a weight-adjusted dose of intravenous (IV) heparin
was administered and transesophageal echocardiography
performed within 1 hour prior to direct-current cardiover-
sion to document absence of intracardiac thrombi. Patients
with AF for Ն48 hours were required to have a documented
weekly international normalized ratio (INR) Ն2.0 for 4
weeks or longer (including within 24 hours of direct-current
cardioversion) or a transesophageal echocardiogram docu-
menting absence of intracardiac thrombi within 1 hour prior
to direct-current cardioversion. These patients were treated
with weight-adjusted IV heparin immediately before cardio-
version. All patients were discharged with a recommenda-
tion for therapeutic anticoagulation for at least 4 weeks after
direct-current cardioversion according to American College
of Cardiology (ACC)/American Heart Association (AHA)/
European Society of Cardiology (ESC) guidelines.
Equipment and waveforms
Patients were randomized in a 1:1 ratio to treatment with
either the Medtronic Physio-Control device (Physio-Control
Lifepak-12, Medtronic Physio-Control Corp, Redmond,
WA, USA) or the Zoll M device (Zoll M-series biphasic,
Zoll Medical Corporation, Chelmsford, MA, USA). Both
devices have an integrated patient impedance measurement
sensing pulse at the beginning of the waveform. The
Medtronic Physio-Control defibrillator utilizes a biphasic
truncated exponential (BTE) waveform that compensates
for impedance by adjusting the leading-edge voltage and
pulse durations (Figure 1).17
In contrast, the Zoll device uses
a biphasic rectilinear (BR) waveform designed to maintain a
relatively constant current during the first phase. Impedance
compensation is achieved by adjusting the leading-edge volt-
age while pulse durations are unchanged (Figure 2).18
Maxi-
mal selected energies are 360 J for the Physio-Control
device and 200 J for the Zoll device. Device-specific wet
polymer gel pads (“Physio Quik-Combo” for the BTE
waveform or “Zoll Pro-Padz” for the BR waveform) were
applied to the anterior right parasternal area (anode) and the
posterior left infrascapular area (cathode).
Cardioversion protocol
Direct-current cardioversion was performed with the pa-
tient in the sedated, postabsorptive state after documenta-
tion of AF on the ECG and verification of qualification
criteria, including anticoagulation status. Shock protocols
used a step-up method of 50, 70, 100, 125, 150, 200, 300,
and 360 J for the BTE waveform, and 50, 75, 100, 120, 150
and 200 J for the BR waveform. Patients who were not
converted with the maximum shock from one device could
receive the maximum shock from the other device. Success-
ful direct-current cardioversion was defined as conversion
to sinus rhythm for at least 1 minute. Data, which included
the amount of selected and delivered energy, current, im-
pedance, and success in restoring sinus rhythm, were re-
corded for each shock. Complications, which included skin
burns and shock-induced arrhythmia, also were recorded.
Statistical analysis
The primary hypothesis of the study was that cardiover-
sion efficacy of the two waveforms (BTE and BR) was not
equivalent. Assuming the cumulative efficacy for one of the
waveforms was 85%, a sample size of 75 patients in each
383Alatawi et al Comparison of Biphasic Waveforms for Cardioversion
3. group was needed to achieve a power of 80% in rejecting
the null hypothesis (that the difference in cumulative effi-
cacy was Ն15%). Continuous variables are expressed as
mean Ϯ SD or median values and compared with two-
sample Wilcoxon rank sum test. Categorical variables are
expressed as percentages and compared using the Chi-
square or Fisher’s exact test (where appropriate). P Յ .05
was considered statistically significant for all comparisons.
Results
Patient characteristics
Of the 188 patients initially enrolled, 47 were excluded
from the final analysis because of one of the following
conditions: presence of atrial flutter in the immediate pre-
cardioversion ECG upon blinded review (n ϭ 25), presence
of an intracardiac mass on precardioversion transesophageal
echocardiogram (n ϭ 7), or failure to adhere to study pro-
tocol (n ϭ 15). Of the 15 protocol deviations, six resulted
from immediate recurrence of atrial fibrillation (within 1
minute) following shock delivery; therefore, defibrillation
energy was not escalated by the operator as required by the
protocol (i.e., the same energy was repeated and success
achieved; 3 BTE, 3 BR). Overall, 141 patients were ran-
domized to treatment with either the BTE waveform (N ϭ
70) or the BR waveform (N ϭ 71). After exclusions, the
number of patients in each group was just below the number
suggested by the power calculation (n ϭ 75). However, with
70 patients in each group, a difference of 16% could be
detected if present (with power 80%), so enrollment was not
reopened. Table 1 lists the clinical characteristics of the
patients enrolled. There was no difference in any of the
baseline clinical variables between the two treatment
groups. Specifically, there was no difference in body mass
index, presence of structural heart disease, use of cardioac-
tive and antiarrhythmic medications, or duration of AF
before direct-current cardioversion, all factors known to
affect cardioversion success. A separate analysis (not re-
ported), which included all patients excluded for protocol
violations, was performed to exclude the possibility of bias.
Inclusion of these patients did not affect baseline patient
characteristics, success rates, or number of shocks.
Cardioversion results
Overall, direct-current cardioversion success was very
high using the two biphasic waveforms. No significant dif-
ference was observed for overall success between patients
treated with the BTE waveform or the BR waveform (97%
vs 93%, respectively, P ϭ .44). In addition, there was no
difference in the total number of shocks used by either
system (2.7 Ϯ 2.0 for BTE vs 2.7 Ϯ 1.8 with BR, P ϭ .60)
or first-shock success (30% with BTE vs 21% with BR, P ϭ
.23). Failure to restore sinus rhythm with maximal shock
energy was observed in two patients randomized to BTE
waveform. Sinus rhythm could not be restored using the
maximal energy (200-J) BR waveform. Of the five patients
who did not respond to maximal BR shock, three were
successfully converted with a maximal energy (360-J) BTE.
This difference in conversion with maximal energy between
the two waveforms did not achieve statistical significance
(P ϭ .43). In addition, the preconditioning effect of eight
BTE shocks vs six BR before crossover limits interpretation
of the crossover observation. The duration of AF prior to
cardioversion was different between patients with success-
ful cardioversion and those with unsuccessful cardiover-
sion. AF lasting more than 1 month was observed in 6 of 7
patients (86%) who did not achieve sinus rhythm compared
to only 44 of the 134 patients (33%) who underwent suc-
cessful direct-current cardioversion (P Ͻ .01). There was no
difference between successful and unsuccessful patients
with regard to other clinical factors, including age, gender,
body mass index, left ventricular ejection fraction, presence
of different comorbidities, or use of cardioactive and anti-
arrhythmic medications. Although there was no significant
difference between selected and delivered energy for the BTE
waveform, there was a significant difference between selected
and delivered energy for the BR waveform (Table 2). Both
Figure 1 Biphasic truncated exponential waveform.
Figure 2 Biphasic rectilinear waveform.
384 Heart Rhythm, Vol 2, No 4, April 2005
4. cumulative selected energy (median 120 J [50–1,355] J for
BTE vs 125 J [50–695] for BR, P ϭ .04) and cumulative
delivered energy (median 120 J [50–1,355] for BTE vs 157
J [48–857 for BR, P ϭ .009) were lower for the BTE
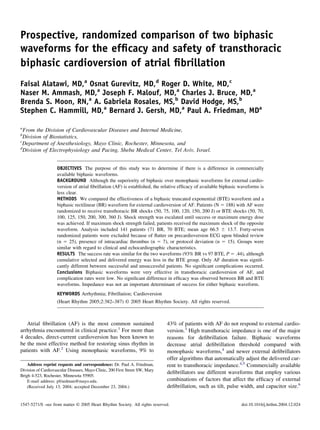
waveform compared to the BR waveform. Figure 3 lists the
cumulative success of sinus rhythm restoration with each
energy level using the different waveforms. No significant
difference between waveforms was observed at the first
energy level, and there was no suggestion of difference at
any subsequent energy levels used in this study. Using an
initial selected direct-current cardioversion energy of 150 J
with either biphasic waveform restores sinus rhythm in 90%
of patients with AF, with no apparent advantage of starting
at lower energies (Figure 3). There was no significant differ-
ence in success rates in patients with high impedance (Ͼ70 ⍀)
compared to patients with low impedance (Figure 4).
Complications
Significant skin redness was observed in 2 patients (3%)
in each group. Transient bradycardia (Ͻ50 bpm) was ob-
served after direct-current cardioversion in 2 patients (2.8%)
from the BR group. One patient from the BTE group was
Table 1 Clinical characteristics of patients enrolled to transthoracic cardioversion by biphasic truncated exponential (BTE) or
biphasic rectilinear (BR) waveform
BTE (N ϭ 70) BR (N ϭ 71) P value
Age at enrollment (years) 65.3 Ϯ 14.5 67.6 Ϯ 12.9 .35
Median (min, max) 66.5 (24, 93) 70.0 (33, 93)
Male gender 50 (71%) 48 (68%) .62
BMI (n ϭ 139) 30.2 Ϯ 6.1 31.8 Ϯ 6.8 .23
Median (min, max) 29.2 (18, 50) 30.7 (19, 55)
Echocardigraphic LVEF (n ϭ 131) 53.9 Ϯ 12.7 54.0 Ϯ 13.0 .71
Median (min, max) 60.0 (15, 70) 55.0 (15, 75)
Left atrial size (cc/m2
) (n ϭ 75) 43.5 12.9 44.5 12.1 .84
Median (min, max) 44.5 (17, 79) 45.0 (17, 82)
Estimated time of present AF .52
Յ48 hours 13 (19%) 12 (17%)
Ͼ48 hours–Յ7 days 20 (29%) 14 (20%)
Ͼ7 days–4 weeks 13 (19%) 19 (27%)
1–12 months 20 (29%) 24 (34%)
Ͼ1 year 4 (6%) 2 (3%)
History of hypertension 26 (37%) 35 (49%) .15
History of diabetes 9 (13%) 11 (15%) .65
History of CAD 14 (20%) 23 (32%) .09
History of cardiomyopathy 15 (21%) 17 (24%) .72
Valvular disease 29 (41%) 30 (42%) .92
Post cardiac surgery 6 (9%) 10 (14%) .30
History of thromboembolism 12 (17%) 10 (14%) .62
Prior cardioversion 25 (36%) 29 (41%) .53
Medications (prior to cardioversion)
Class I antiarrhythmia medications 8 (11%) 11 (15%) .48
Amiodarone 12 (17%) 14 (20%) .69
Sotalol 4 (6%) 3 (4%) .72
Calcium channel blocker 7 (10%) 5 (7%) .53
Beta-blocker 36 (51%) 34 (48%) .67
Lanoxin 18 (26%) 21 (30%) .61
Angiotensin-converting enzyme II inhibitor 27 (39%) 29 (41%) .78
Diuretic 29 (41%) 32 (45%) .66
Values are given as mean Ϯ SD or number (percent) unless otherwise indicated.
BMI ϭ body mass index; AF ϭ atrial fibrillation; CAD ϭ coronary artery disease; LVEF ϭ left ventricular ejection fraction.
Table 2 Cardioversion data comparison
BTE(N ϭ 70) BR(N ϭ 71) P value
Total no. of shocks mean Ϯ SD 2.7 Ϯ 2.0 2.7 Ϯ 1.8 .6
Cardioversion successful [No. (%)] 68 (97%) 66 (93%) .44
Cumulative selected energy 120 125 .04
Median (min, max) (50, 1,355) J (50,695) J
Cumulative delivered energy 120 156.9 .009
Median (min, max) (50, 1,355) J (48.4, 857) J
385Alatawi et al Comparison of Biphasic Waveforms for Cardioversion
5. fully paced by his preexisting pacemaker after direct-current
cardioversion secondary to bradycardia.
Discussion
Efficacy and safety of biphasic direct-
current cardioversion
Both the BTE and the BR waveforms proved to be highly
effective and safe for treatment of patients referred for
direct-current cardioversion of AF, with cumulative success
rates of 97% and 93%, respectively. This finding is in
accordance with results of previous studies4,19,20
and sig-
nificantly exceeds results obtained with monophasic direct-
current cardioversion.3,4,19
Ricard et al19
reported a 93%
success rate in converting AF in 30 patients treated with a
BTE waveform. Mittal et al4
reported a 94% success rate in
88 patients with AF treated with BR shocks. Neal et al20
compared BTE and BR waveforms for direct-current car-
dioversion of AF in 101 patients. They described a similar
efficacy in restoration of sinus rhythm using either waveform,
reaching 97.9% with the BTE waveform (N ϭ 47) and 100%
in patients treated with the BR waveform (N ϭ 53). The higher
success rates in their study compared with previous studies4,19
and with current study likely result from different definitions
for successful cardioversion. We required maintenance of si-
nus rhythm for at least 1 minute in order to define successful
cardioversion, whereas Neal et al20
considered the presence
of only three consecutive P waves, captured atrial paced
rhythm, or junctional rhythm as successful direct-current
cardioversion. No difference between waveforms was ob-
served with regard to the number of shocks needed.
We observed a significantly higher cumulative delivered
energy with the BR waveform compared with the BTE
waveform (Table 2). With the BTE waveform device, se-
lected and delivered energies remain essentially the same
until an energy selection of 360 J into an impedance Ն100 ⍀
is obtained. On the other hand, with the BR waveform
defibrillator, selected and delivered energies can differ sig-
nificantly from each other depending upon patient imped-
ance. This difference between selected and delivered ener-
gies is a consequence of an attempt to maintain a relatively
constant first-phase current as delivered energy is adjusted
in accord with an impedance schedule. For example, the BR
device delivers 245 J into 86-⍀ impedance with an energy
selection of 200 J. In most studies, including that of Neal
et al, this difference between selected and delivered energies
is not determined.
The manufacturers of the two devices compared in this
study use different methods for measuring impedance,
precluding the possibility of comparisons between the
devices based on patient impedance. Nevertheless, for
each device, patient impedance had no effect on wave-
form efficacy (Figure 4). This observation contrasts with
the widely held belief that shock efficacy is decreased by
increases in patient impedance and may reflect the suc-
cess of impedance compensating algorithms in both de-
vices.
Unlike Neal et al,20
we observed higher cumulative en-
ergy with the BR waveform needed to achieve direct-cur-
rent cardioversion endpoint. This difference between our
results and theirs could be explained by the different shock
protocols used. We used a detailed step-up protocol, includ-
ing 50, 70, 100, 125, 150, 200, 300, and 360 J for the BTE
waveform and 50, 75, 100, 120, 150 and 200 J for the BR
waveform, whereas Neal et al used a simplified four-step
protocol using only three energy levels of 50, 100, 200, and
200 J for both waveforms.
The safety profile of the two waveforms proved to be
high; only 3% of patients in each group suffered significant
skin redness. Postshock bradycardias were rare. This finding
is in accordance with previous findings.4,19,20
Figure 3 Cumulative success in restoring sinus rhythm with
different energy levels by biphasic truncated exponential (BTE) or
biphasic rectilinear (BR) waveforms.
Figure 4 Effect of transthoracic impedance on waveform success.
Left: Cardioversion success rate with BTE shocks in patients with
low (Ͻ70 ⍀) vs high (Ͼ70 ⍀) impedance is the same (P ϭ .99).
Right: Cardioversion success rate with BR shocks in patients with
low (Ͻ70 ⍀) vs high (Ͼ70 ⍀) impedance is the same (P ϭ .39).
386 Heart Rhythm, Vol 2, No 4, April 2005
6. Optimizing first-shock energy
To optimize the efficacy and risk profile of direct-current
cardioversion, it is desirable to administer only the minimal
amount of energy needed to restore sinus rhythm using a
single shock. The optimal first-shock energy for biphasic
waveforms has not been well defined. In this study, we used
a step-up protocol with eight different energy levels for the
BTE waveform and six levels for the BR waveform (ac-
cording to device capabilities). In contrast with results of
other investigators who recommended a starting energy of
100 J,20
our results suggest the optimal first-shock energy
for transthoracic direct-current cardioversion of AF using
biphasic waveforms should be 150 J (Figure 3). At this
energy, success is 90% with both waveforms compared with
77% (BTE) and 82% (BR) at 100 J. Using the higher energy
does not appear to add complications. Of note, different
starting energies were not directly compared in this study.
Conclusion
Both BTE and BR waveforms are highly effective and safe
for direct-current cardioversion of AF in humans. The op-
timal first-shock energy for transthoracic biphasic direct-
current cardioversion of AF should be 150 J. Impedance is
not a determinant of direct-current cardioversion success
with biphasic waveforms.
Acknowledgments
The authors thank Robert Walker of Medtronic Physio-
Control and Don Boucher of Zoll Medical Corporation for
assistance with waveform specifications.
References
1. Kannel W, Abbott R, Savage D, McNamara P. Epidemiologic features
of chronic atrial fibrillation: the Framingham study. N Engl J Med
1982;306:1018–1022.
2. Lown B, Perlroth M, Kaidbey S, Abe T, Harken D. Cardioversion of
atrial fibrillation: a report on the treatment of 65 episodes in 50
patients. N Engl J Med 1963;269:325–331.
3. Carlson M, Biblo L. Atrial fibrillation: new frontiers. Cardiol Clin
1996;14:607–622.
4. Mittal S, Ayati S, Stein K, Schwartzman D, Cavlovich D, Tchou P,
Markowitz S, Slotwiner D, Scheiner M, Lerman B. Transthoracic
cardioversion of atrial fibrillation: comparison of rectilinear biphasic
versus damped sine wave monophasic shocks. Circulation 2000;101:
1282–1287.
5. Kerber R, Martins J, Kienzle M, Constantin L, Olshansky B, Hopson
R, Charbonnier F. Energy, current, and success in defibrillation and
cardioversion: clinical studies using an automated impedance-based
method of energy adjustment. Circulation 1988;77:1038–1046.
6. Tomassoni G, Newby K, Kearney M, Brandon M, Barold H, Natale A.
Testing different biphasic waveforms and capacitances: effect on atrial
defibrillation threshold and pain perception. J Am Coll Cardiol 1996;
28:695–699.
7. Morris JJ, Peter R, McIntosh H. Electrical conversion of atrial fibril-
lation: Immediate and long-term results and selection of patients. Ann
Intern Med 1966;65:216–231.
8. Fain E, Sweeney M, Franz M. Improved internal defibrillation with a
biphasic waveform. Am Heart J 1989;117:358–364.
9. Winkle R, Mead R, Ruder M, Gaudiani V, Buch W, Pless B, Sweeney
M, Schmidt P. Improved low energy defibrillation efficacy in man with
the use of a biphasic truncated exponential waveform. Am Heart J
1989;117:122–127.
10. Chapman P, Vetter J, Souza J, Troup P, Wetherbee J, Hoffmann R.
Comparative efficacy of monophasic and biphasic truncated exponen-
tial shocks for nonthoracotomy internal defibrillation in dogs. J Am
Coll Cardiol 1988;12:739–745.
11. Bardy G, Ivey T, Allen M, Johnson G, Mehra R, Greene H. A
prospective randomized evaluation of biphasic versus monophasic
waveform pulses on defibrillation efficacy in humans. J Am Coll
Cardiol 1989;14:728–733.
12. Kavanagh K, Tang A, Rollins D, Smith W, Ideker R. Comparison of
the internal defibrillation thresholds for monophasic and double and
single capacitor biphasic waveforms. J Am Coll Cardiol 1989;14:
1343–1349.
13. Wyse D, Kavanagh K, Gillis A, Mitchell L, Duff H, Sheldon R, Kieser
T, Maitland A, Flanagan P, Rothschild J, Mehra R. Comparison of
biphasic and monophasic shocks for defibrillation using a nonthora-
cotomy system. Am J Cardiol 1993;71:197–202.
14. Reddy R, Gleva M, Gliner B, Dolack G, Kudenchuk P, Poole J, Bardy
G. Biphasic transthoracic defibrillation causes fewer ECG ST-segment
changes after shock. Ann Emerg Med 1997;30:127–134.
15. White R. Early out-of-hospital experience with an impedence-com-
pensating low-energy biphasic waveform automatic external defibril-
lator. J Interv Card Electrophysiol 1997;1:203–208.
16. Fuster V, Ryden L, Asinger R, Cannom D, Crijns H, Frye R, Halperin
J, Kay G, Klein W, Levy S. ACC/AHA/ESC guidelines for the man-
agement of patients with atrial fibrillation: executive summary: a
report of the American College of Cardiology/American Heart Asso-
ciation Task Force on Practice Guidelines and the European Society of
Cardiology Committee for Practice Guidelines and Policy Conferences
(committee to develop guidelines for the management of patients with
atrial fibrillation) developed in collaboration with the North American
Society of Pacing and Electrophysiology. J Am Coll Cardiol 2001;38:
1231–1265.
17. Geddes L, Havel W. Evolution of the optimum bidirectional (ϩ/Ϫ
biphasic) wave for defibrillation. Biomed Instrum Technol 2000;34:
39–54.
18. Mittal S, Ayati S, Stein K, Knight B, Morady F, Schwartzman D,
Cavlovich D, Platia E, Calkins H, Tchou P. Comparison of a novel
rectilinear biphasic waveform with a damped sine wave monophasic
waveform for transthoracic ventricular defibrillation. J Am Coll Car-
diol 1999;34:1595–1601.
19. Ricard P, Levy S, Boccara G, Lakhal E, Bardy G. External cardiover-
sion of atrial fibrillation: comparison of biphasic vs monophasic wave-
form shocks. Europace 2001;3:96–99.
20. Neal S, Ngarmukos T, Lessard D, Rosenthal L. Comparison of the
efficacy and safety of two biphasic defibrillator waveforms for the
conversion of atrial fibrillation to sinus rhythm. Am J Cardiol 2003;
92:810–814.
387Alatawi et al Comparison of Biphasic Waveforms for Cardioversion