2. Definition
Cardiomyopathies are defined as
"a heterogeneous group of diseases of the
myocardium associated with mechanical
and/or electrical dysfunction that usually (but
not invariably) exhibit inappropriate ventricular
hypertrophy or dilatation and are due to a
variety of causes that frequently are genetic."
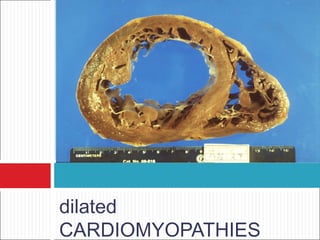
4. Dilated Cardiomyopathy
•An enlarged left ventricle with decreased systolic function
as measured by left ventricular ejection fraction
characterizes dilated cardiomyopathy .
• Systolic failure is more marked
• Diastolic dysfunction, in the setting of marked volume
overload
6. Pathophysiology
Brief primary injury such as infection or toxin exposure.
Some myocytes may die during the initial injury, while
others survive only to have later programmed cell death,
(apoptosis).
As the surviving myocytes hypertrophy to accommodate
the increased burden of wall stress,
Local and circulating factors stimulate deleterious
responses that contribute to progression of disease,
even in the absence of further primary injury,Dynamic
remodeling and the amount of ventricular dilation.
Mitral regurgitation commonly develops as the valvular
apparatus is distorted by ventricular dilation
7.
8. DCM: Inflammatory
Infective
Reported with almost all types of infectious agents
Viral- Co xsackie , adenovirus, HIV, hepatitis C
Parasitic - T. cruzi— Chag as' dise ase , toxoplasmosis
Bacterial- diphtheria, Spirochetal ,Bo re llia
Rickettsial-Q fever
Fungal -with systemic infection
10. DCM: Inflammatory
Mechanism
Direct tissue injury resulting from viral infection
Immune mediated injury
Viral infection in susceptible hosts may be a
proximate cause of cardiomyopathy
11. DCM: Peripartum
Diagnostic Criteria
1 mo pre, 6 mos post
Echo: LV dysfunction
LVEF < 45%
LVEDD > 2.7 cm/m2
Epidemiology/Etiology
1:4000 women
Riskfactors - increased maternal age, increased
parity, twin pregnancy, malnutrition, use of
tocolytic therapy for premature labor, and
preeclampsia or toxemia of pregnancyJAMA
12. DCM: Peripartum
Proposed mechanisms:
Inflammation - reflect increased susceptibility
to viral myocarditis or
Autoimmune -myocarditis due to cross-
reactivity of anti-uterine antibodies against
cardiac muscle.
prolactin cleavage fragment, salt ingestion
Women with full recovery are more likely to
tolerate a subsequent pregnancy than are
14. DCM: Toxic
Alcoholic cardiomyopathy
Toxicity is attributed both to alcohol and acetaldehyde.
Superimposed vitamin deficiencies and toxic a additives
are rarely implicated.
6 drinks daily for 5–10 years, but frequent binge
drinking may also be sufficient.
Reversible with abstinence
Mechanism?:
Myocyte cell death and fibrosis
Directly inhibits: mitochondrial oxidative
phosphorylation Fatty acid oxidation
15. DCM: Toxic
Anthracyclines
Cause vacuolar degeneration and myofibrillar loss.
Generation of reactive oxygen species involving heme
compounds is currently the favored explanation for myocyte
injury and fibrosis.
Disruption of the large titin protein may contribute to loss of
sarcomere organization.
Three different presentations
Acute heart failure/ Early onset /The chronic presentation -
Leads to a relatively nondilated ventricle, perhaps due to
fibrosis.
Thus, the stroke volume may be severely reduced with an
ejection fraction of 30–40%,
Therapy is suppression of "inappropriate" sinus tachycardia,
and attention to postural hypotension .
21. DCM: Idiopathic
Is a diagnosis of exclusion,
when all other known factors have been
excluded.
two-thirds of dcm are still labeled as
idiopathic;
may reflect unrecognized genetic disease.
Continued reconsideration of etiology often
reveals later
22. Miscellaneous
Arrhythmogenic RV Dysplasia
Desmosomal complex disrupt myocyte junctions
and adhesions,
Myocardium of RV free wall replaced:
Fibrofatty tissue
Regional wall motion/function is reduced
Ventricular arrhythmias
SCD in young
"woolly hair," and thickened palms and soles.
24. Miscellaneous
LV Noncompaction
Diagnostic Criteria
Prominent trabeculations, deep recesses in LV apex
Thin compact epicardium, thickened endocardium
associated with multiple genetic variants in the sarcomeric
and other proteins such as tafazzin
Prognosis and Treatment
Increased risk of CHF, VT/SCD, thrombosis
Hereditary risk
Screening of offspring
26. Miscellaneous
Tako-Tsubo Cardiomyopathy
The apical ballooning syndrome, or stress-induced
cardiomyopathy, occurs typically
In older women after sudden intense emotional or
physical stress
Presentations include pulmonary edema, hypotension,
and chest pain with ECG changes mimicking an acute
infarction.
May result from intense sympathetic activation with
heterogeneity of myocardial autonomic innervation,
diffuse microvascular spasm, and/or direct
catecholamine toxicity.
28. Evaluation of the DCM
HISTORY
Detailed family history
History of alcohol, illicit drugs, chemotherapy or radiation
therapy
A past or associated history of rheumatologic, endocrine, or
infectious diseases
Assessment of ability to perform routine and desired
activities
Assessment of volume status, orthostatic blood pressure,
body mass index
32. X-RAY CHEST
Cardiomegaly
Pulmonary vascular
congestion
Kerley B lines
Prominent
vasculature of the
upper lung fields.
Pleural effusion
usually on the right
side, but it can be
bilateral
33. Electrocardiogram
No specific electrocardiographic findings
Sinus tachycardia is often present
poor R wave progression, intraventricular conduction
delays, and LBBB.
A wide QRS complex portends a worse prognosis
left ventricular fibrosis may exhibit anterior Q waves
nonspecific ST-segment and T wave abnormalities as
well as P wave alterations
Persistent supraventricular or ventricular
tachyarrhythmias represent an important etiologic factor
for ventricular dysfunction
34. ECHOCARDIOGRAPHY.
Cornerstone in the evaluation and
management
LVEDD are usually greater than 60 mm
Global hypokinesia
Decreased EF and FS
Associated ds
36. CARDIAC MRI AND MULTIDETECTOR CT
RADIONUCLIDE IMAGING
INVASIVE EVALUATION INCLUDING
ENDOMYOCARDIAL BIOPSY.
37. Management
PHARMACOLOGIC ANDDEVICE THERAPY
Neurohormonal antagonists to prevent
disease progression
Diuretics to maintain the volume balance are
the therapeutic cornerstone
Prophylactic implantable cardiac defibrillators
and biventricular pacemakers is indicated in
appropriate patients
39. SURGERY.
Patients with structural heart ds conditions
corrected
Left ventricular assist devices- provide
aggressive mechanical support to patients
with advanced decompensated heart failure
EMERGING SPECIFIC THERAPIES
infections and immunomodulatory agents
Stem cells for cardiac regeneration and gene
40. Presentation with Symptomatic Cardiomyopathy
Dilated Restrictive Hypertrophic
Ejection fraction
(normal 55%)
Usually <30% 25-50% >60%
LVDD (nor<55 mm) 60 mm >60 mm (may be
decreased)
Often decreased
Left ventricular wall
thickness
Decreased Normal or increased Markedly increased
Atrial size Increased Increased; may be
massive
Increased; related to
abnormal
Valvular
regurgitation
Related to annular
dilation; mitral earlier,
during
decompensation;
tricuspid late stages
Related to endocardial
involvement; frequent
mitral and tricuspid
regurgitation, rarely
severe
Related to valve-
septum interaction;
mitral regurgitation
Common first
symptoms
Exertional intolerance Exertional intolerance,
fluid retention early
Exertional intolerance;
may have chest pain
The threshold of left ventricular enlargement and dysfunction necessary to diagnose peripartum cardiomyopathy has not been precisely defined. The following definition, based upon a 1992 NHLBI workshop definition for idiopathic dilated cardiomyopathy, has been proposed [34,35]:
Left ventricular ejection fraction (LVEF) less than 45 percent AND/OR M-mode fractional shortening less than 30 percent PLUS Left ventricular end-diastolic dimension greater than 2.7 cm/m2