Presentation1.pptx, ultrasound of the hand and fingers.
•Als PPTX, PDF herunterladen•
51 gefällt mir•13,289 views


Empfohlen
Empfohlen
Weitere ähnliche Inhalte
Was ist angesagt?
Was ist angesagt? (20)
Ähnlich wie Presentation1.pptx, ultrasound of the hand and fingers.
Ähnlich wie Presentation1.pptx, ultrasound of the hand and fingers. (20)
Mehr von Abdellah Nazeer
Mehr von Abdellah Nazeer (20)
Presentation1.pptx, ultrasound of the hand and fingers.
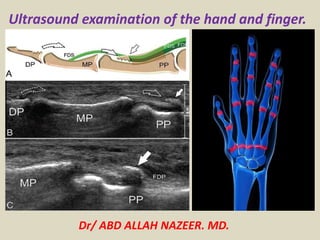
- 1. Dr/ ABD ALLAH NAZEER. MD. Ultrasound examination of the hand and finger.
- 2. SCANNING TECHNIQUE Either: Sit the patient on the side of the bed with a pillow on their lap to support their hand Sit the patient on a chair on the opposite side of the bed with their hand resting on the bed. EQUIPMENT SELECTION AND TECHNIQUE Use of a high resolution probe (7-15MHZ)with a small footprint is essential when assessing superficial structures. Careful scanning technique to avoid anisotropy (and possible misdiagnosis). Beam steering or compounding can help to overcome anisotropy in linear structures such as tendons. Good colour / power / Doppler capabilities when assessing vessels or vascularity of a structure. Be prepared to change frequency output of probe (or probes) to adequately assess both superficial and deeper structures.
- 3. ULTRASOUND OF THE HAND & FINGERS - Normal PALMAR ASPECT (Flexors) Finger Flexors There are 2 flexor tendons of the fingers: Flexor digitorum superficialis, inserting as 2 separate slips onto the base of the middle phalanx. Flexor digitorum profundus, inserting onto the distal phalanx. Scan plane for the Flexor digitorum tendons. The Profundus and superficialis. Normal Flexor digitorum Profundus (FDP) and superficialis tendons (FDS) at the level of the metacarpal neck.
- 4. Scan plane for the flexor digitorum tendons in transverse prior to the separation of superficialis from profundus. The Flexor digitorum superficialis tendon slips (green) can be seen peeling off the Profundus portion (blue).
- 5. Scan plane for the flexor digitorum tendon at the A4 pulley, distal to the superficialis insertions. Flexor digitorum profundus tendon in transverse. The neurovascular bundles are circled in red.
- 6. Scan plane for the flexor digitorum profundus insertion. The Flexor digitorum profundus insertion onto the distal phalanx.
- 7. Pulleys The flexor tendons are secured in place by a series of pulleys which are fibrous bands wrapping over the tendons and attaching to the bone. Annular pulleys: which wrap transversely over the tendons. Numbered A1 – A4. Cruciate pulleys: which are paired and cross diagonally over the tendons. Numbered C1 - C3. The annular pulleys are readily visible with high resolution, high quality equipment. The cruciate pulleys are poorly seen. Scan plane A2 pulley. A2 pulley at the proximal phalanx.
- 8. Scan plane for the A2 pulley in transverse. Transverse view of the A2 pulley (green) firmly overlying the flexor digitorum tendon at the mid proximal phalanx.
- 9. Palmar fascia Scan plane when assessing for the palmar fascia Normal palmar fascia (green).
- 10. DORSAL ASPECT Extensor digitorum tendons Unlike the flexors, there is only an extensor digitorum Scan plane for the extensor digitorum insertion. Even with high frequency transducer, the very thin tendon is difficult to visualize without using a stand-off pad or thick gel. The extensor digitorum tendon insertion to the distal phalanx. The tendon is extremely thin and lies intimately against the bone.
- 11. Nail-bed Sac plane for the extensor digitorum insertion. Note the thick gel. The nail bed is best viewed through a thick gel standoff.
- 12. Ulnar collateral ligament of the thumb (UCL) The ulnar collateral ligament of the 1st metacarpophalangeal joint medially. Rupture is a skiier's or gamekeeper's thumb. If the torn ligament folds under the adductor pollicis it is referred to as a 'Stenner lesion'. The ulnar collateral ligament on the 1st metacarpophalangeal joint. Rupture is called a skiier's or gamekeeper's thumb. If the torn ligament folds under the adductor pollicis it is referred to as a 'Stenner lesion'.
- 13. ROLE OF ULTRASOUND To assess for: muscular, tendinous and ligamentous damage (chronic and acute). Foreign bodies. Joint effusions. Soft tissue masses such as ganglia, lipomas. Classification of a mass e.g solid, cystic, mixed. Post surgical complications e.g abscess, edema. Guidance of injection, aspiration or biopsy. Relationship of normal anatomy and pathology to each other. Some bony pathology.
- 14. Joint Effusions Size Simple/complex Any synovial thickening Any vascularity on power Doppler - Normal is little or no discernable flow. Hyperemia = acute. Detection of Effusion in the volar recess of the PIP joint – longitudinal and transverse views.
- 15. Joint and bursal effusion.
- 16. Inflammatory Arthritis Ultrasound(Sonography) aids in the confirmation of synovitis in early inflammatory arthritis. The sonographic evaluation of inflammatory arthritis has been aided by consensus definitions of synovitis and erosions by the OMERACT group. Small amounts of fluid can be detected in joints as well as tendon sheaths. Ultrasound is also more sensitive in the detection of enthesitis. Increased vascularization can be demonstrated by power Doppler. Active synovitis overlying a large metacarpal head erosion.
- 17. Longitudinal view of the wrist revealing active synovitis.
- 18. Grey scale ultrasound can be used to demonstrate synovitis. In this image of a metacarpophalangeal joint of a patient with rheumatoid arthritis, the joint capsule is markedly distended outwards (arrows) due to underlying synovial effusion and hypertrophy. The presence of power Doppler demonstrates the increased microvascular flow of the joint, which is suggestive of active inflammation. M, metacarpal bone; P, proximal phalanx.
- 19. Colour spots correspond to areas of increased synovial perfusion and/or angiogenesis: (A) metacarpophalangeal joint (longitudinal dorsal scan), (B) metacarpophalangeal joint (longitudinal dorsal scan) (detail showing colour spots inside a bone erosion (*) filled by synovial tissue), (C) finger flexor tendons (T) (longitudinal volar scan), (D) finger flexor tendons (longitudinal transverse scan).
- 20. Longitudinal and transverse views of the first MTP revealing tophaceous dorsal deposit as well as double contour sign.
- 21. Tendon abnormalities Look for hyperemia, tendon sheath fluid (simple/complex) and tendon integrity/homogeneity Check for tendon thickening (compare with other side) Fluid in the tendon sheath Integrity of the tendon- any tear? does the tendon slide freely when mobilized? Longitudinal (A) and transverse (B) scans of a flexor tenosynovitis distal palmar region. The thorn (between calipers, arrow) can be seen as a hyperechoic stripe in a hypoechoic cavity (C). T: tendon.
- 22. Flexor Tenosynovitis (Fluid around tendon sheath).
- 23. TB tenosynovitis of the hand flexor tendons. Transverse (top) and longitudinal (bottom) ultrasound images. The transverse views demonstrate enlarged, heterogenous appearing tendons with neovascularity within them. There is thickening and effusion within the tendon sheath on the longitudinal views.
- 24. Tenosynovitis of the flexor tendons with a large effusion and synovial thickening in the tendon sheath in a patient with rheumatoid arthritis.
- 25. Ultrasound appearance of normal flexor tendon sheath and tenosynovitis. a, Normal appearance, longitudinal view. b, Normal appearance, transverse view. c, Flexor tenosynovitis, longitudinal view. d, Flexor tenosynovitis, transverse view. Arrows in c and d indicate tendon sheath thickening. MC: metacarpal; P: phalanx; FT: flexor tendon.
- 26. Extensor tendinosis in a 34-year-old woman. Sagittal US scan of the dorsal metacarpophalangeal joint shows a thickened extensor pollicis brevis tendon (ET). Posttraumatic development of an osseous excrescence (arrow) resulted in chronic repetitive friction against the adjacent tendon, culminating in tendinosis. MCP = metacarpal.
- 27. Dupuytren's contracture What is it? Fibrosis of the palmer fascia forcing the flexion of the 4th/5th fingers. Gradual onset M>F Often inherited. Generally affects 4th and 5th fingers. Scan in longitudinal from the base of the proximal phalanx down into the palm looking superficial to the flexor tendon It will appear as a hypoechoic focal fusiform thickening of the palmar fascia at the metacarpal head level. Not to be confused with trigger finger
- 30. Dupuytren's contracture of the hand.
- 31. Trigger finger What is it? Tenosynovitis of a flexor digitorum tendon causing forced flexion of a finger. Initially in transverse, identify the flexor digitorum tendons at the metacarpal head level. Follow the common tendon proximally to the carpal tunnel. Then follow distally to the insertions: The Flexor digitorum superficialis divides, with two slips inserting onto the side of the base of the middle phalanx. Flexor digitorum profundus inserts onto the distal phalanx.
- 32. Short-axis view of the normal A1 pulley in the right middle finger. Open arrow indicates the A1 pulley and needle trajectory; asterisk, middle of the target triangle and ideal location for the needle tip for injection; dotted arrows, digital nerves; L, lumbrical muscle; M, metacarpal; and VP, volar plate. The bifurcation of the common digital artery is shown as 2 small hypoechoic dots below the digital nerve on the left. The common digital artery is shown as the larger hypoechoic dot below the bifurcating digital nerve on the right.
- 33. First annular pulley injection for trigger finger before (A) and after (B) injection with triamcinolone acetonide and lidocaine. Distention of the pulley is noted (arrows). The images are from a patient not in the study.
- 34. Trigger thumb with a tenosynovitis and a thickened A1 pulley.
- 35. Trigger thumb. Left: Axial US scan of the metacarpophalangeal joint of the left thumb shows focal thickening of the flexor pollicis longus tendon (arrows). Right: Axial US scan of the metacarpophalangeal joint of the right thumb shows a normal tendon (arrows).
- 36. Finger Pulleys What are they? Bands of fibrous tissue holding the flexor tendon to the finger similar to runners on a fishing rod. They are named according to their type-Annular (around) or Cruciform (cross), and numbered from proximal to distal. Scan longitudinally over the anterior surface of the finger. The pulleys may be seen as thin hypoechoic zones intimately overlying the flexor tendon sheath. If ruptured, the tendon will no longer follow the bone and will instead "bowstring".
- 37. Thickness of A1 pulley and flexor digitorum tendons, but also changes of quality of these structures contributed to pathogenesis of trigger fingers .
- 38. Arrows depict A1 pulley hypertrophy on US, with Power Doppler demonstrating hyperemia, and post-contrast T1 fat-suppressed MRI demonstrating pulley enhancement
- 39. A, Volar longitudinal ultrasonographic scan obtained in a volunteer shows the A3 annular pulley (arrows). B, Corresponding macroscopic section. Also note the distal end of the A2 pulley (arrowhead). C, Volar transverse ultrasonographic scan obtained in another volunteer shows the fibrillar pattern of the A3 annular pulley. Asterisk indicates volar plate of the proximal interphalangeal joint.
- 40. Acute complete tears of A2 pulleys. (A) Schematic drawing and (B) sagittal US obtained over the palmar aspect of the proximal phalanx (PP) of the fourth digit. In (A) note the A2 tear and the subsequent palmar dislocation (arrows) of the flexor digitorum superficialis (FDS) and profundus (FDP) tendons. In (B) the A2 pulley (black arrow) is thickened and hypoechoic. Note the palmar bowstringing of the tendons (white arrow). The tendon sheath contains a fluid collection (arrowheads).
- 41. Game keepers thumb/ skiers thumb What is it? Rupture of the ulnar collateral ligament of the thumb due to a sudden valgus force. May occur after repeated stretching of the ligament. The ligament usually tears at it's distal end from the base of the proximal phalanx. If there is marked angulation of the phalanx, the flailing ligament may impinge under the adductor pollicis creating a ' Stenner lesion ‘.
- 43. Stener lesion in a 28-year-old man. Coronal US scan of the thumb shows a proximally retracted nodule with an irregular lobulated outline (arrows), an appearance diagnostic of a Stener lesion. The nodule represents the retracted proximal segment of the UCL and is consistent with a full-thickness tear. Displacement of this segment superficial to the aponeurosis results in loss of the smooth contour of the aponeurosis and surface lobulation. MCP = metacarpal, PP = proximal phalanx.
- 44. Stener lesion. (a) Coronal US scan of the thumb shows a proximal lobulated nodule (S, arrows), which represents the retracted displaced proximal segment of the UCL. The smooth contour of the aponeurosis is distorted by the superficially lying ligament, resulting in bulging of the surface of the aponeurosis. MCP = metacarpal, PP = proximal phalanx. (b) Axial US scan of the thumb shows a thickened lobulated UCL (cursors). There is loss of the smooth contour of the aponeurosis with bulging (arrow). The diagnosis can be made by using the same criteria as on coronal scans. The left side of the image is radial. ET = extensor tendon, MCP = metacarpal head, TH = thenar eminence. (c) Axial US scan of the thumb, obtained for comparison with b, shows a normal UCL. The adductor aponeurosis (black arrowheads) covers the muscle and UCL (white arrowhead). Note the anisotropy of these structures. There is no nodule, lobulation, or bulging. The right side of the image is radial. ET = extensor tendon, MCP = metacarpal head, TH = thenar eminence.
- 45. Foreign bodies Ensure you approach the proposed site of the foreign body from different angles. Some materials will be poorly reflective and almost invisible unless the beam is perpendicular to them. There will usually be a surrounding hypoechoic halo representing an inflammatory reaction Identify: The plane of tissue it is in. How close it is to the entry wound and to any blood vessels. It may be helpful to mark the location and orientation of the foreign body on the skin to guide removal.
- 46. Foreign body in hand Normal right pulp USG Gray scale.
- 47. Multiple images for the foreign bodies.
- 48. Masses 95% of finger tumours are benign. abscess granuloma Ganglia Neuroma Fibroma Glomus tumour (nail bed tumour) For non-specific palpable or visible masses see our superficial lumps page.
- 49. Giant cell tumor – Longitudinal USG-hypoechoic well defined lesion anterior to the middle finger flexor tendon with increased signal on Doppler.
- 50. Multiple images for Giant cell tumors:
- 51. Finger Abscess Without Involvement of Tendon.
- 52. A ganglion cyst.
- 53. Multiple images for fibrous tumors.
- 54. Multiple images for the Epidermoid cysts.
- 55. Haemangioma with a hypoechoic easy compressible vascularized tumor on the volar side of the flexor tendon
- 56. Glomus Tumor of the thumb.
- 57. Joint Abnormalities Gout: Abnormal uric acid metabolism resulting in joint inflammation. May see tophaceous gout as a complex echogenic mass (tophus) in the soft Osteoarthritis: Bony irregularities at the bone ends with joint effusion. When acute the joint will be hyperemic Rheumatoid arthritis: Thickened synovium with a complex 'thick' joint effusion, pannus & associated bony irregularity
- 58. Gouty arthritis with increased vascularity.
- 60. Thank You.