Presentation1.pptx, radiological imaging of upper limb ischemia.

This document discusses radiological imaging techniques for evaluating upper limb ischemia. It begins by providing background on upper limb ischemia, noting it has varied etiologies including atherosclerosis, arteritis, and trauma. CT angiography is described as the preferred initial imaging technique, providing high-quality images of the entire arterial tree to precisely plan revascularization. Other techniques discussed include Doppler ultrasound, MRI, and invasive angiography. The document then provides several examples of upper limb CT angiography findings, demonstrating various pathologies like thrombosis, aneurysms, occlusions, and fistulas. In summary, the document outlines radiological evaluation and various pathologies of upper limb ischemia visualized on CT angiography.

Empfohlen
Weitere ähnliche Inhalte
Was ist angesagt?
Was ist angesagt? (20)
Andere mochten auch
Andere mochten auch (19)
Ähnlich wie Presentation1.pptx, radiological imaging of upper limb ischemia.
Ähnlich wie Presentation1.pptx, radiological imaging of upper limb ischemia. (20)
Mehr von Abdellah Nazeer
Mehr von Abdellah Nazeer (20)
Presentation1.pptx, radiological imaging of upper limb ischemia.
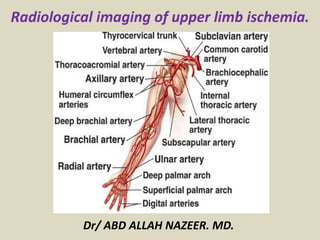
- 1. Radiological imaging of upper limb ischemia. Dr/ ABD ALLAH NAZEER. MD.
- 2. Introduction: Upper limb ischemia is an uncommon entity which presents less commonly as compared to lower limb ischaemia, and has a wide range of etiology and controversies in preoperative investigations and management. Less than 2% of patients with upper limb ischaemia presents with rest pain, gangrene or ulcer. Although upper limb loss is less as compared to lower limb, it can result in severe functional impairment and disability if there should be any delay in diagnosis and treatment. The single most common etiology is thromboembolic events secondary to atherosclerosis followed by trauma. Nevertheless, differential diagnoses such as arteritis, thoracic outlet obstruction and aneurysms need to be considered. The signs and symptoms of presentation ranged from nonspecific slight numbness and weakness to pain, pallor and pulselessness. The most common combination of presenting complaints was cold, pulselessness and painful upper limb.
- 3. Upper extremity occlusive disease is relatively uncommon and accounts for only 5% of all extremity ischemia. Unlike occlusive disease in the lower extremities, which is generally atherosclerotic in origin, the etiology of upper extremity occlusive disease is more varied and can include atherosclerotic disease, arteritis, connective tissue disorders, occupational injuries, and Vasospastic diseases. Etiology Upper extremity occlusive disease can involve the large and small arteries of the arm or a combination. Atherosclerosis is the most common cause of large artery disease and generally involves the subclavian artery, but disease may extend more distally, especially in the setting of diabetes. Patient risk factors are similar to those of other vascular beds. Tobacco use is almost universal. Hypercholesterolemia, hypertension, diabetes and age are also important risk factors. Inflammatory diseases (giant cell and Takayasu’s arteritis) can also involve the large vessels. Small vessel disease due to diabetes can lead to severe complications such as digital ulceration and gangrene.
- 4. Raynaud’s disease is a Vasospastic disorder that produces a tri-phasic colour change in the hands or less commonly the feet, in response to cold or emotional stimuli. The hallmark of this disorder is pallor, cyanosis and post ischemic hyperemia of a digit or digits, although all three may not always be present. The disorder is classified as primary when no identifiable cause is evident or secondary when it is due to either a more proximal occlusion or other disease process resulting in digital artery vasospasm . Patients whose occupations involve the use of vibrational tools or who use their hands as a hammer (especially the hypothenar eminence) can present with Raynaud’s or frank digital ischemia from either hand-arm vibration syndrome or hypothenar hammer syndrome. Occlusive lesions in the arm and hand secondary to scleroderma, rheumatoid arthritis, systemic lupus and other autoimmune disorders can lead to severe upper extremity ischemia manifesting as pain, ulceration and gangrene. Thromboangiitis obliterans (Buerger’s disease) is an inflammatory disease that can produce pain and ulceration in the fingers and toes. The patient is usually a young man with a long history of tobacco use. Rare causes of upper extremity occlusive disease include iatrogenic injury, trauma, malignancy and frostbite.
- 5. Common Conditions Associated with Upper Extremity Ischemia: • Thromboembolism • Atheromatous Embolization • Atherosclerosis • Connective Tissue Diseases( • Scleroderma, • Rheumatoid Arthritis, • Sjörgren’s Syndrome, • Systemic Lupus Erythematosus) • Large Artery Vasculitis( • Takayasu’s Disease, • Giant Cell Arteritis) • Small Artery Vasculitis(• Thromboangitis Obliterans (Buerger’s disease). • Blood Dyscrasias • Myeloproliferative Disorders • Thoracic Outlet Syndrome • Latrogenic Injury • Occupational Exposure(• Hand-arm Vibration Syndrome, • Hypothenar Hammer Syndrome). • Vasospasm( • Raynaud’s Disease, • Cocaine Use, • Amphetamine Use).
- 6. Acute ischemia in the upper extremity constitutes 10–15% of all acute extremity ischemia. The etiology is emboli in 90% of the patients. The reason for this higher rate compared with the leg is that atherosclerosis is less common in arm arteries. Emboli have the same origins as in the lower extremity and usually end up obstructing the brachial artery. Sometimes plaques or an aneurysm in the subclavian or axillary arteries is the primary source of emboli. Embolization to the right arm is more common than to the left due to the vascular anatomy. For the 10% of patients with atherosclerosis and acute thrombosis as the main cause for their arm ischemia, the primary lesions are located in the brachiocephalic trunk or in the subclavian artery. Such pathologies are usually asymptomatic due to well-developed collaterals around the shoulder joint until thrombosis occurs, and they cause either micro- or macroembolization.
- 7. Clinical Presentation Acute arm ischemia is usually apparent on the basis of the physical examination. The symptoms are often relatively discreet, especially early after onset. The explanation for this is the well developed collateral system circumventing the brachial artery around the elbow, which is the most common site for embolic obstruction. The "six Ps” – pain, pallor, paresthesia, paralysis, pulselessness, poikilothermia– are applicable also for acute arm ischemia, but coldness and color changes are more prominent than for the legs. Accordingly, the most common findings in the physical examination are a cold arm with diminished strength and disturbed hand and finger motor functions. Tingling and numbness are also frequent. The radial pulse is usually absent but is pounding in the upper arm proximal to the obstruction. Gangrene and rest pain appear only when the obstruction is distal to the elbow and affects both of the paired arteries in a finger or in the lower arm. Ischemic signs or symptoms suggesting acute digital artery occlusion in only one or two fingers, imply microembolization.
- 8. Chronic symptomatic ischemia in the upper extremity is the result of blood flow that is nutritionally inadequate to fulfill metabolic requirements. Symptoms may also result from inappropriate thermoregulatory function. Ischemia may be secondary to inappropriate vessel response when vessels are unable to vasodilate in response to stress or inappropriate vasoconstriction (i.e., vasospastic disease); intima/media injury resulting in aneurysm, embolism, and thrombosis (occlusive disease); or a combination of both (vaso-occlusive disease). Occlusive events may occur secondary to low-flow states in vasospastic disease that precipitate thrombosis development (i.e., secondary occlusion) or secondary to ischemia from occlusive disease that may produce autonomic dysfunction and secondary vasospasm. This cross-over phenomenon creates difficulty in evaluation and management. The goal of this article is to assess contemporary methods of evaluation, classification, and management of upper extremity ischemia.
- 9. Radiological Imaging: X-Ray to show any evidence of cervical rib. Duplex ultrasound is rapid, can be performed at the bedside, and has near 100% sensitivity for diagnosing complete arterial occlusion. Ankle-brachial index (ABI) will be near zero for patients with acute limb ischemia. CTA has the benefit of rapid availability and high-quality imaging, which allows for precise planning of revascularization. CTA provides imaging of the entire arterial tree from the aortic inflow to the digital level. CTA typically requires 150 mL of iodinated contrast and therefore has to be used with caution in patients with baseline renal insufficiency (glomerular filtration rate <40). For patients with renal insufficiency, aggressive hydration before and after examination with sodium bicarbonate is recommended for CTA or invasive angiography. MRA has a limited role in acute limb ischemia, as the examination can be lengthy (45–60 minutes), is less often available outside regular work hours, and generally has poorer arterial imaging than 64 (or greater) slice CTA. Invasive angiography has the advantage of allowing for simultaneous percutaneous revascularization with both mechanical thrombectomy and thrombolytic therapy.
- 12. Acute Upper Limb Ischemia with right subclavian and brachial thrombus.
- 13. Upper limb acute ischemia with recent jugular vein thrombosis.
- 14. With significant external compression with the probe, a visualized thrombus (blue arrow) is seen within a non-compressible brachial artery
- 16. The distal (right side subclavian shows no flow.
- 17. Thrombosis of the brachial artery.
- 18. Vessels and nerve trauma. Biker’s hammer. (A) Longitudinal and (B) axial colour Doppler US obtained over the palmar aspect of the hypothenar region. Images show a nearly complete thrombosis (black arrowheads) of the superficial branch of the ulnar artery. Some small persistent internal flow signal can be detected (white arrowheads). Note increase in size of the artery and thickening of its wall. HH=hook of the hamate.
- 19. Left Cervical rib with upper limb chronic ischemia.
- 20. CT angiography using modern MDCT scanners has evolved into a highly accurate noninvasive diagnostic tool for the evaluation of patients with pathologic abnormalities of the upper extremity arterial system. upper extremity CTA can effectively evaluate for stenosis, occlusion, aneurysm, or embolic events, especially when they affect vessels proximal to the wrist. Atherosclerotic disease affects the upper extremities disproportionately less than the lower extremities. However, proximal involvement of the upper extremities is not infrequent. Risk factors are no different than those for other sites of atherosclerotic involvement and include hypertension, dyslipidemia, diabetes mellitus, age, and a history of smoking . Claudication is the most common presenting symptom, though most patients are asymptomatic because of collateral formation. Blood pressure differences between the upper extremities can frequently be found in these patients. Symptoms are often chronic, with more acute symptoms suggesting acute thrombosis or an embolic event. In the setting of subclavian involvement, upper extremity symptoms may be masked or overshadowed by symptoms related to compromised flow to the ipsilateral vertebral artery due to subclavian steal, particularly syncope and presyncope. In patients with left or right internal mammary bypass grafts, subclavian artery disease can cause myocardial ischemia. Atherosclerotic disease, when identified on imaging, should prompt inquiry into concomitant sites of involvement processes—namely, cardiovascular and cerebrovascular involvement.
- 21. CT Angiography of the Upper Extremity Arterial System: Axial subvolume maximum intensity projection better outlines stenosis (arrowheads). Axillofemoral bypass (asterisk) is depicted end-on. Volume-rendered image shows axillofemoral bypass graft (arrow) with stenosis proximal and distal to anastomosis in native left axillary artery (arrowheads).
- 22. Volume-rendered CT angiography shows long occlusion of brachial artery, which was caused by acute thromboembolism.
- 23. Old woman with acute type A thoracic aortic dissection who presented with acute chest pain and syncope. Physical examination revealed weak right upper extremity pulse. CT angiography of right upper extremity, chest, abdomen, and pelvis was performed to evaluate for aortic dissection and upper extremity arterial pathology. Oblique multiplanar reconstruction image reveals ascending aortic dissection, with intimal flap (arrowheads) covering origins of all supraaortic branch vessels.
- 24. 49-year-old man in chronic phase of Takayasu disease involving arch and supraaortic vessels. A, Volume-rendered image shows right subclavian artery aneurysm (arrow) and left subclavian artery stent (arrowhead) implanted for steno-occlusive disease. 49-year-old man in chronic phase of Takayasu disease involving arch and supraaortic vessels. B, Axial image shows concentric thickening (arrowheads) of wall of origins of all three supraaortic branches.
- 25. 64-year-old woman with giant cell arteritis who presented with fever, malaise, and bilateral upper extremity weakness. CT angiography using axial curved multiplanar reconstruction algorithm shows typical irregular wall thickening (arrowheads) of bilateral axillary and subclavian arteries.
- 26. 29-year-old male heavy smoker with thromboangiitis obliterans who presented with ischemic symptoms of both upper and lower extremities. A, Upper extremity CT angiography (CTA) shows distal ulnar artery occlusion (short thick arrow) and distal radial artery contour irregularity (arrowheads) in right upper extremity. Note typical corkscrew collaterals (long thin arrow). Stenoocclusive disease was also present in left ulnar and interosseous arteries.
- 27. 50-year-old woman with history of embolic disease to left arm and fibromuscular dysplasia involving bilateral carotid, renal, and external iliac arteries (not shown) who also had involvement of left brachial artery with medial fibrosis, which shows typical “string-of- beads” sign (arrowheads).
- 28. 17-year-old girl with thoracic outlet syndrome who was evaluated at outside institution for embolic event to left hand. She was found to have aneurysm of left subclavian artery, which was subsequently treated with covered stent. Several months after procedure, patient presented to our institution with heaviness and coolness of left arm and hand. A, Volume- rendered image shows subclavian artery stent, with proximal occlusion (arrowhead) and presence of left cervical rib (single asterisk). First rib is marked with double asterisks. Clavicle was excluded for clarity.
- 29. 17-year-old girl with thoracic outlet syndrome who was evaluated at outside institution for embolic event to left hand. She was found to have aneurysm of left subclavian artery, which was subsequently treated with covered stent. Several months after procedure, patient presented to our institution with heaviness and coolness of left arm and hand. B, Curved multiplanar reconstruction of left subclavian artery shows completely thrombosed stent (asterisks). Patient underwent subclavian artery vein graft placement and resection of left cervical and first ribs. Volume-rendered image shows vein graft (asterisks) and resection of left cervical and first ribs. Curved multiplanar reconstruction confirms vein graft patency (asterisks).
- 30. 23-year-old man with arteriovenous malformation in right axilla. B, Maximum intensity projection of upper extremity CT angiography shows malformation (arrowhead), with lateral thoracic artery as main feeder, and early venous drainage, Volume-rendered image shows arteriovenous malformation and anomalous high origin of radial artery (arrowhead), which is normal variant.
- 31. 17-year-old boy with known diagnosis of Ehlers-Danlos syndrome type 4 who presented to emergency department with extremely painful acute onset swelling of right axilla and Pulseless right upper extremity. A, CT of chest and upper extremity was performed. Unenhanced CT shows large right axillary hematoma (asterisk). B, Maximum intensity projection CT angiography shows extravasation from spontaneously ruptured right axillary artery (arrow). Emergent proximal surgical ligation was performed.
- 32. Angiogram of the right- upper extremity. (A) Axillary artery occlusion caused by a distal segment. (B) The injured artery and the extensive collateralization.
- 33. 23-year-old man with dialysis fistula who presented with reduced flows while undergoing hemodialysis and ischemic symptoms in fingers of left hand. B, Subvolume maximum intensity projection (MIP) shows patent arterial anastomosis but diseased radial artery (A) with occlusion distally (arrowheads). There was also stenosis in vein (V) immediately distal to anastomosis (arrow). A, Upper extremity CT angiography volume-rendered view shows dialysis fistula with aneurysm formation (asterisk) on venous side.
- 34. 23-year-old man with dialysis fistula who presented with reduced flows while undergoing hemodialysis and ischemic symptoms in fingers of left hand. More central subvolume MIP shows critical stenosis of left subclavian vein (arrow).
- 35. 59-year-old woman who underwent stent placement in left subclavian artery at outside institution presented with recurrent left upper extremity claudication. CT angiography shows stent fracture (arrow) and severe stenosis (arrowheads) due to intimal hyperplasia.
- 36. Completion angiogram of the right upper limb revealing the axillary– brachial–ulnar axis and the partially-thrombosed aberrant radial artery.
- 37. Chest roentgenogram demonstrates the clavicular abnormality. Arch aortogram demonstrates a filling defect in the right subclavian artery and occlusion of the axillary artery.
- 38. Venogram shows occlusion of the right subclavian vein extending to the first rib, with multiple collateral vessels. An angiogram in a 35-year-old woman with right arm ischemia that demonstrates right subclavian artery occlusion from the medial margin of the first rib to the axillary artery at the level of the humeral head.
- 39. An arteriogram of the right shoulder in neutral position, demonstrating right subclavian stenosis (arrow). An arteriogram of the right upper extremity in abduction, demonstrating increased subclavian artery stenosis and aneurysmal dilation (arrow) in the location of the clavicle and first rib.
- 40. Thoracic outlet syndrome with stenosis of the left subclavian vein.
- 41. 73-year-old woman with acute embolus in left axillary artery .
- 42. Left axillary artery occlusion in a patient with Wegener's granulomatosis .
- 43. Left brachial artery thrombosis in a patient with Wegener's granulomatosis .
- 44. Angiogram of upper extremity. The top is in a normal position. The bottom is in a hyperabducted position (arrow indicates area of stenosis).
- 45. Distal axillo-brachial artery occlusion.
- 46. Septic embolization from severe prosthetic aortic valve endocarditis resulted in a 2.5cm brachial artery pseudoaneurysm (circled) that was associated with a pocket of purulence and upper limb ischemia.
- 48. Angiogram that demonstrates blockage of the ulnar artery.
- 49. Axial CT angiography source image shows ulnar artery thrombosis with ulnar artery aneurysm (between arrowheads). Ulnar artery reconstruction with right leg saphenous vein autograft was performed, and patient became symptom free. Volume-rendered reconstruction shows occluded ulnar artery (between arrowheads) at Guyon canal.
- 50. Angiogram of end-stage Raynaud’s disease with extremely poor peripheral circulation. Angiogram that demonstrates an ulnar artery aneurysm.
- 51. An angiogram demonstrating lack of blood flow to vessels of the hand in Buerger's disease with ischemia to the fingers.
- 52. Angiogram of a patient with Buerger’s disease that shows decreased circulation of index and thumb. Angiogram that shows decreased circulation in the ulnar digits of the hand.
- 53. Angiogram of right upper extremity with "string of beads" appearance of the brachial artery (lower left) in fibromuscular dysplasia with chronic ischemia.
- 54. Conclusions. Upper limb ischaemia remains infrequently seen compared to lower limb ischaemia. Nevertheless, the complications and late effects can result in significant impairment in function. Evaluation of upper limb ischaemia requires careful history taking and clinical examinations. Although angiography remains the gold standard, other non-invasive tools such as duplex US. Prompt surgical intervention results in favorable outcomes.
- 55. Thank You.