Extralevator abdominoperineal excision
•Als PPT, PDF herunterladen•
5 gefällt mir•3,602 views

Extralevator abdominoperineal excision

Empfohlen
Weitere ähnliche Inhalte
Was ist angesagt?
Was ist angesagt? (20)
Ähnlich wie Extralevator abdominoperineal excision
Ähnlich wie Extralevator abdominoperineal excision (20)
Mehr von Yannick Nijs
Kürzlich hochgeladen
Kürzlich hochgeladen (20)
Extralevator abdominoperineal excision
- 3. Extralevator abdominoperineal excision - APE Introduction• APR <> LAR – Optimalisation surgical technique (TME) – Increasing rates – local control – survival • APR – Tumors less than 6 cm – No optimalisation surgical technique – perineal phase – More local recurrence <> LAR – Dutch TME trial LR 12% <> 29% – MERCURY trial LR 12% <> 33%
- 4. Extralevator abdominoperineal excision - APE Introduction• APR - LAR – Worse outcome <> LAR – Dutch TME-trial APR – CRM +LR 30% OS 38% – CRM - LR 9% OS 72% – Significantly more inadvertent bowel perforation AR APR Norway 4% 15% Sweden 3% 14% Holland 3% 14%
- 5. Extralevator abdominoperineal excision - APE Introduction • APR – Difficult – conventional technique – High risk bowel perforation – Specimen waist lower border – CRM close rectum – Study posterior perineal approach – More cylindrical specimen – Reduction bowel perforation – positive CRM
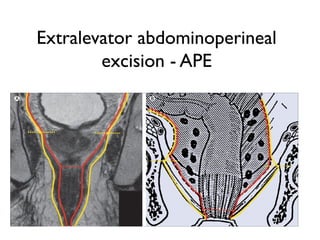
- 6. Extralevator abdominoperineal excision - APE Introduction – Conventional technique – Outside mesorectum – pelvic floor – Mobilisation from levator muscles – Excision anal canal – ischiorectal fat – lower portion levator muscles – “Waist” surgical specimen
- 7. Extralevator abdominoperineal excision - APE Methods – APE – extended posterior perineal approach – No dissection mesorectum off levator muscles – Stop mobilisation upper border coccyx – below autonomic nerves – below vesicles
- 8. Extralevator abdominoperineal excision - APE Methods – Prone jack-knife position – Anus closed double purse-string suture – Dissection outside subcutaneous portion external anal sphincter – Dissection outer surface levator muscles until insertion pelvic side wall – Disarticulation coccyx – Division Waldeyer’s fascia – levator muscles – Dissection off prostate –posterior vagina
- 9. Extralevator abdominoperineal excision - APE Methods
- 10. Extralevator abdominoperineal excision - APE Methods
- 11. Extralevator abdominoperineal excision - APE Methods
- 12. Extralevator abdominoperineal excision - APE Methods• APR – Wound complications – 35-66% (pre-op RTX – extensive dissection) – Various flap techniques – Gluteus maximus flap reconstruction – Arises iliac bone, sacrum – coccyx and insertion lateral femur – Rotational musculocutaneous flap based cranially – Large defect bilateral – based cranially and distally
- 13. Extralevator abdominoperineal excision - APE Methods • Gluteus maximus flap reconstruction – Local anesthesia adrenaline – Subcutaneous tissue incised gluteus maximus and fascia – 1/3rd muscle divided medial border – Avoid sciatic nerve ! – Further submuscular dissection cranially and medially – Sutured four layers » Muscle, Scarpa’s fascia, deep dermis, skin
- 14. Extralevator abdominoperineal excision - APE Methods
- 15. Extralevator abdominoperineal excision - APE Methods • Gluteus maximus flap reconstruction – Two drains (deep muscle – along flap subcutis) – Kept 4-6 days – Surgical tape dressing – Decubital mattress – Specific mobilisation schedule
- 16. Extralevator abdominoperineal excision - APE Results• Patient characteristics – 28 patients – 19 men and 9 women – median age 66 (range 49-86 yrs) – T3-T4 tumour lower rectum MRI – All neoadjuvant treatment – 6 patients intraoperative radiotherapy – Single surgeon performed resection
- 17. Extralevator abdominoperineal excision - APE Results – Inadvertent bowel perforation 1 patient – 23 patients unilateral flap – 5 bilateral – Operating time 80 min – 110 min – 3 wound infection of which 1 partial wound rupture – 1 postoperative bleeding – 24 other primary healing no delay
- 18. Extralevator abdominoperineal excision - APE Results – Histopathological examination – T0 2 patients,T3 20 patients,T4 6 patients – CRM +(< 1mm) 2 patients (T4) – Median FU 16 months (1-45) – 2 patients local recurrence – 8 patients died – 4 no disease – 3 distant M+ – 1 local recurrence and distant M+
- 19. Extralevator abdominoperineal excision - APE Discussion – Posterior perineal approach alternative conventional APR –Poor results after APR –APR common procedure tumours < 6 cm –T1-T2 tumours utralow anterior resection partial resection IAS / less extensive posterior perineal resection – Low rate perforation and CRM involvement –LR rate 7% low T3-T4 tumours –Short FU time
- 20. Extralevator abdominoperineal excision - APE Discussion – Surgical technique posterior perineal approach –No dissection mesorectum off levator muscles –Perineal part prone jack-knife position –Levator muscle resected en bloc anal canal –Cylindrical specimen –Lower risk LR and bowel perforation –Excellent exposure
- 21. Extralevator abdominoperineal excision - APE Discussion – Low rate perineal wound complications –Extensive resection posterior perineal approach –Flap reconstructions superior primary closure –Intact muscular layers without strain – Gluteus maximus flap superior –Rectus abdominis flap technically more demanding –Distant donor-site morbidity- denervated – not contractile –No functional disordes – good cosmetic outcome –Plastic surgeon
- 22. Thank you