
Empfohlen
Weitere ähnliche Inhalte
Ähnlich wie Osteoporosis.pptx
Ähnlich wie Osteoporosis.pptx (20)
Mehr von VinodkumarMugada1
Kürzlich hochgeladen
Kürzlich hochgeladen (20)
Osteoporosis.pptx
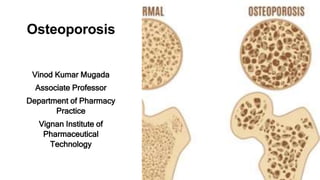
- 1. Osteoporosis Vinod Kumar Mugada Associate Professor Department of Pharmacy Practice Vignan Institute of Pharmaceutical Technology
- 2. Definition This disease is a long-term and gradually worsening condition that causes bones to become thinner, weaker, and more likely to break. Over time, the structure of the bones breaks down and their overall strength decreases, making them more fragile and prone to fractures.
- 3. Pathophysiology- Primary Osteoporosis • Primary osteoporosis chiefly afflicts the geriatric population • Etiology: progressive bone loss and microarchitectural deterioration • Alternatively denominated as age-related osteoporosis • Idiopathic primary osteoporosis: atypical manifestation in juveniles and young adults • Obscure etiology for idiopathic primary osteoporosis • Potential causes: reduced bone genesis, augmented bone resorption, or both • Underlying factor: primary defect in osteocyte functional regulation
- 4. Pathophysiology- Secondary Osteoporosis • Genetic disorders: cystic fibrosis, idiopathic hypercalciuria, hemochromatosis, osteogenesis imperfecta • Hypogonadal states: anorexia nervosa, athletic amenorrhea, Turner syndrome, Klinefelter syndrome, premature ovarian failure • Endocrine disorders: Cushing syndrome, adrenal insufficiency, type 1 diabetes mellitus, hyperparathyroidism, thyrotoxicosis • Gastrointestinal diseases: malabsorption, inflammatory bowel disease, gastrectomy, primary biliary cirrhosis
- 5. Pathophysiology- Secondary Osteoporosis • Secondary osteoporosis results from a variety of specific clinical conditions, diseases, or medications, all of which can accelerate bone loss • Hematologic disorders: sickle cell disease, multiple myeloma, hemophilia, leukemias, lymphomas • Rheumatic and autoimmune diseases: rheumatoid arthritis, lupus, ankylosing spondylitis • Medications: heparin, glucocorticoids, anticonvulsants, lithium, methotrexate, thyroxine, parenteral nutrition, gonadotropin- releasing hormone agonists, cyclosporine A, tacrolimus
- 6. Mechanism of Age-Related Osteoporosis •Age-related osteoporosis: most prevalent form of the condition •Affects both genders; 2-3 times more common in females •Women's bone loss: biphasic (rapid menopausal phase lasting 4-8 years, followed by slower phase) •Men's bone loss: monophasic, slow, and continuous •Rapid phase in women: 5-10% cortical bone loss; 20-30% trabecular bone loss •Osteoporotic fractures: predominantly in trabecular bone (proximal/distal limb bones, vertebral bodies)
- 7. Mechanism of Age-Related Osteoporosis •Slower phase: 20-25% of cortical and trabecular bone loss for both genders •Rapid phase cause: estrogen deficiency, increased bone resorption, decreased bone formation •Slower phase factors: impaired bone formation, reduced calcium/vitamin D intake, decreased physical activity •Men's hormone conversion: testosterone transformed to estrogen by aromatase enzyme •Deficiency in men: primarily due to increased sex hormone- binding globulin, reducing bioavailability of testosterone and estrogen
- 8. Mechanism of Age-Related Osteoporosis •99% of bodily calcium reserves: sequestered within the skeleton •Calcium: vital for robust skeletal support structure •Calcium requirements: stable for women pre-menopause; increase during menopause •Menopausal calcium demand: driven by estrogen-related alterations in renal calcium conservation and intestinal calcium absorption •Age-related decrease in calcium absorption efficiency: contributing factor •By age 65: intestinal calcium absorption efficiency declines to 50% below adolescent peak absorption levels
- 9. History and Physical + The FRAX® tool has been developed to evaluate fracture risk of patients. It is based on individual patient models that integrate the risks associated with clinical risk factors as well as bone mineral density (BMD) at the femoral neck.
- 11. History and Physical • Fall risk assessment: crucial during patient evaluation • Risk factors to consider: • History of falls, loss of consciousness, or fainting • Balance, dizziness, or coordination issues • Muscle weakness • Lower extremity arthritis • Difficulty standing or walking • Impaired vision • Lower extremity neuropathy • Medication history: potential impact on coordination and balance • 4 or more risk factors: 80% increased likelihood of a fall • Home assessment: may be necessary for comprehensive fall
- 12. Medical History • Female gender: nonmodifiable risk factor; 2-3 times more common than in men • Adult, geriatric (>65 years): increased risk with age • White ethnicity: higher risk for white and Asian women • Family history of osteoporosis: significant genetic influence • Past medical history of bone fracture: increased future fracture risk • Weight <70 kg: higher osteoporosis risk • Smoking: direct toxic effects on osteoblasts; decreases bone mineral density
- 13. Medical History • Adrenal glucocorticoid use: major risk factor for bone loss and fractures • Hypogonadism: secondary osteoporosis cause in both genders • Menopause: rapid bone loss post-menopause • Amenorrhea: risk factor for osteoporosis • Delayed puberty: nonmodifiable risk factor • Lactation: associated with mild BMD decreases • Dietary calcium deficiency: decreases bone mineral density
- 14. Medical History • Vitamin D deficiency: contributes to osteoporosis • Alcohol abuse: detrimental effects on BMD, increased fall and fracture risk • Sedentary lifestyle: significant and rapid bone loss • Hyperthyroidism: associated with decreased bone mass and osteopenia • Hypervitaminosis A: secondary osteoporosis cause • Anticonvulsant use: increased fracture risk; secondary osteoporosis cause • Heparin use: associated with bone loss; increased osteoporosis risk • Proton pump inhibitor use: independent risk factor for osteoporotic fracture in older adults, especially postmenopausal women
- 15. Treatment Summary • Goals of therapy: prevent fractures, stabilize/increase bone mass, relieve symptoms, maximize physical function • Fracture prevention: primary goal for confirmed diagnosis or increased osteoporosis risk • Strategies: maintain bone health, prevent bone injury, dietary measures, lifestyle modifications • Individual treatment recommendations: based on risk assessment, fracture history, BMD measurements • Pharmacologic therapy: for men and women with osteoporosis or fragility fractures • National Osteoporosis Foundation: drug therapy recommendations based on BMD T-scores and fracture probability
- 16. Treatment Summary • American Association of Endocrinology: drug therapy recommendations based on BMD T-scores and fracture history • North American Menopause Society: osteoporosis pharmacotherapy recommendations • FDA-approved agents: antiresorptive agents and anabolic agent (teriparatide) • Tailoring treatment: consider severity of bone loss and comorbidities • United States Surgeon General's office: encourage prevention of bone loss in young and middle-aged adults • Treatment for specific populations: FDA-approved Prescribing Information recommendations • Acute symptomatic vertebral compression fracture: calcitonin therapy, surgical treatment considerations, avoid vertebroplasty