
Empfohlen
Weitere ähnliche Inhalte
Was ist angesagt?
Was ist angesagt? (20)
Andere mochten auch
Andere mochten auch (16)
Ähnlich wie Early repolarisation syndrome (2)
Ähnlich wie Early repolarisation syndrome (2) (20)
Kürzlich hochgeladen
Kürzlich hochgeladen (20)
Early repolarisation syndrome (2)
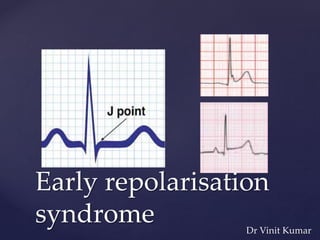
- 1. { Early repolarisation syndrome Dr Vinit Kumar
- 2. Definition Prevalence and Arrhythmic Risk Mechanism of ERP Genetic basis Clinical manifestations Diagnosis Prognostic variables Therapy Conclusion.
- 3. Definition
- 4. In 1976 by Kambara and Phillips suggested that early repolarization was defined by: 1) end-QRS notching or slurring; 2) elevation of the ST-segment; and 3) an upwardsloping ST-segment followed by a tall, symmetrical T-wave. Haissaguerre et al. defined early repolarization as “an elevation of the QRS-ST-segment junction (J-point) in at least 2 leads” (within the same territory; e.g., inferior or lateral leads) as being a sign of early repolarization. The amplitude of the J-point elevation had to be at least 0.1 mV above the baseline level, as either QRS slurring or notching. The amplitude and slope of the ST-segment were not part of the definition Definition
- 5. Tikkanen et al. definition also measured the degree of J-point elevation, which was stratified at levels of 0.1 and 0.2 mV. These investigators also introduced the concept of the ST-segment slope, showing that a horizontal or downwardsloping ST-segment is associated with greater arrhythmic risk
- 6.
- 9. The prevalence of early repolarization in the general population varies from 1% to 9%, depending on age (predominant in young adults), race (highest among black populations), gender (predominant in men), and the criterion for J point elevation (0.05 mV versus 0.1 mV) In a study of a community-based general population of 10,864 middle-aged subjects, the prevalence of early repolarization (J point elevation >0.1 mV) was Overall- 5.8%, inferior leads- 3.5%, lateral leads-2.4%, both- 0.1% J point elevation > 0.2 mV, Overall- 0.33%.
- 10. The ST segment after the J point was horizontal or descending – 71.5% rapidly ascending - 28.5%. incidence - idiopathic VF age <45 years - 3:100 000. J-waves- 11:100 000 The presence of ER is associated with 3 times the risk of developing VF, but the overall risk is still negligible
- 11. ER syndrome - syncope or cardiac arrest is attributed to ER after systematic exclusion of other etiologies.
- 12. N Engl J Med 2008;358:2016-23.
- 15. Another concurrent case–control study also demonstrated a higher prevalence of ER (42%) among survivors of idiopathic VF compared with controls (13%, P<0.01) ER increases the RR of arrhythmic events, the AR remains very low. Incidental identification of ER should not be interpreted as a high risk marker. Clinical decisions are driven by the presence and severity of symptoms and comorbidities
- 16. { Mechanism of Early Repolarization and Idiopathic Ventricular Fibrillation
- 17. the association of ER with arrhythmic risk is typically at rest or during sleep,and not during physical activity.
- 20. Prominent phase 1 notch larger transient-outward K+ current (Ito) - epicardium Greater net repolarizing (outward) current flow during phase 1. In ER -enhancement in epi net outward current, enhancement of the endo-to-epi AP differences manifests as J-waves which reflects current flow from depolarized endo to substantially-repolarized epi - phase 1
- 22. { Genetic Basis
- 23. {
- 24. Case Report: This young female (14 years) was resuscitated in 2001 following an episode of sudden death due to VF. All examinations including coronary angiogram with ergonovine injection, MRI, and flecainide or isoproterenol infusion were normal. The patient had multiple (>100) recurrences of VF unresponsive to beta-blockers, lidocaine/mexiletine, verapamil, and amiodarone. Recurrences of VF were associated with massive accentuation of the early repolarization pattern at times mimicking acute myocardial ischemia. Coronary angiography during an episode with 1.2 mV J/ST elevation was normal. Isoproterenol infusion acutely suppressed electrical storms, while quinidine eliminated all recurrences of VF and restored a normal ECG over a follow-up of 65 months. Genomic DNA sequencing of KATPchannel genes showed missense variant in exon 3 (NC_000012) of the KCNJ8 gene, a subunit of the KATP channel, conferring predisposition to dramatic repolarization changes and ventricular vulnerability. Haissaguerre et al Ventricular fibrillation with prominent early repolarization associated with a rare variant of KCNJ8/KATP channel. J Cardiovasc Electrophysiol. 2009;20:93–98.
- 25. ER vs Brugada J-waves, pause/bradycardia dependent accentuation dynamic nature - ECG pattern, suppression of the ECG features and arrhythmia with isoproterenol and quinidine.
- 26. not seen provocation by sodium channel blocker Some individuals with Brugada syndrome may also have ER (approximately 12%)
- 28. Life-threatening arrhythmias are often the first and unexpected manifestation of ERsyndrome Incidental ECG finding – present intermittently. Repeated measurements from 542 subjects with ER demonstrated the subsequent absence of ER in≈20%. Even in the cardiac arrest population, 58% of patients whose arrest was attributed to ER syndrome had ≥1 ECG that did not demonstrate the ER pattern during their hospitalization There is no proven provocative test to identify concealed ER. Conflicting evidence - association between syncope and ER
- 29. Classification – arrythmic risk associated spatial distribution Type 1 (ER in the lateral precordial leads) - healthy male athletes and - largely benign. Type 2 (ER in the inferior or inferolateral leads) a moderate risk. Type 3 (ER globally in the inferior,lateral, and right precordial leads) - highest risk. Brugada syndrome is classified as type 4 (j-wave/point elevation in the right precordial leads).
- 30. ST characteristics are incremental to the location with a clear higher risk associated with the horizontal or down-sloping pattern.
- 31. ER pattern on ECG should not lead to classification of a ER syndrome other etiologies have been excluded J-point elevation is augmented immediately preceding VF. Systematic assessment of survivors of SCD without evidence of infarction or left ventricular dysfunction. Diagnosis of Ventricular Fibrillation resulting from Early Repolarization Syndrome
- 32. other etiologies excluded High risk baseline ER pattern or Increased parasympathetic tone provokes high risk ER characteristics or Cardiac arrest occurs during sleep/at rest PROBABLE ERS
- 33. current guidelines do not recommend genetic testing cardiac monitoring Echocardiogram evaluation of coronary arteries Signal averaged ECG exercise testing cardiac MRI intravenous epinephrine and sodium channel blocker challenge A careful review of all available ECGs for evidence of ER is warranted, particularly around the time of the cardiac arrest
- 34. { Prognostic Variables of the Early Repolarization Pattern • Electrocardiographic Markers • Sex, Family History, and Ethnicity • Autonomic Tone
- 35. Electrocardiographic Markers inferior location greater amplitude of ER horizontal or down-sloping ST-segment QRS notching vs slurring highest risk - ER of high amplitude (≥0.2 mV) in the inferior limb leads + horizontal or descending ST-segment
- 36. Horizontal ST-segment after early repolarization
- 38. Sex, Family History, and Ethnicity Males African descent
- 39. Autonomic Tone Bradycardia-dependent augmentation of ER is observed in both VF cases and healthy controls Tachycardia tends to normalize ER. night when parasympathetic tone is augmented
- 44. { Early Repolarization modifying risk of underlying Cardiac Pathology
- 45. Much more common modifier in the context of structural heart disease and primary electric disorders ↑ risk of ischemic VF in the event of a myocardial infarction/ischemia ER - inferior leads -increased risk of life-threatening ventricular arrhythmias in patients with chronic CAD , after adjustment for LVEF Predict higher risk of sudden death in nonischemic cardiomyopathy patient ER + Brugada pattern with a ECG is an incremental predictor of arrhythmic events ARVC short QT syndrome .
- 46. { Therapies for Early Repolarization Syndrome
- 47. isoproterenol infusion - acute cases , immediately suppressed electric storms Isoproterenol - initiatedat1.0 μg/min, targeting a20% increase in heart rate or an absolute heart rate 90. bpm, quinidine - chronic cases, decreased recurrent VF suppresses outward currents - Ito, restored a normal ECG Adrenergic activation – enhancing inward currents ( L type Ca2+ current) –offset the net outward K+ current excess Drug Therapy
- 48. Implantable Cardioverter-Defibrillator is indicated after cardiac arrest. highly effective in terminating ventricular arrhythmias in nearly all cases. no current risk stratification strategy for asymptomatic patients Syncope attributed to ER appears clinically uncommon and warrants an aggressive attempt to verify that syncope is related to arrhythmia.
- 50. { Inheritance of Early Repolarization and Family Screening
- 51. heritability in the general population and within families. Siblings - ↑ unadjusted odds of ER ( odds ratio,2.22 ,P= 0.047) A study involving 505 Caucasian nuclear families reported that individuals with ≥1 parent with ER had a 2.5-fold increased incidence of demonstrating the ER pattern. Heritability - higher - inferior leads - notched morphology AD inheritance pattern with incomplete penetrance Currently no recommendation to screen the families in individuals with asymptomatic ER.
- 52. To conclude The ER syndrome as a primary arrhythmogenic disorder causing VF is very rare. lack of clinically useful risk stratifying tools or an established provocative test for identifying malignant ER, despite some ECG features that are associated with a higher risk. As such, patients with asymptomatic ER and no family history of malignant ER should be reassured that their ECG is a normal variant, until such time as better tools enable risk stratification.
- 53. All patients with ER should continue to have modifiable cardiac risk factors addressed
- 54. As in a war when you don’t know well your enemy ,it is better to maintain a constant precaution and look for as many information as possible in order to avoid defeat
- 55. { Thank you
Hinweis der Redaktion
- J > 0.2- RR 3.94, ST – 3.14