Seal of Good Local Governance (SGLG) 2024Final.pptx
Clinical examination of the equine respiratory system
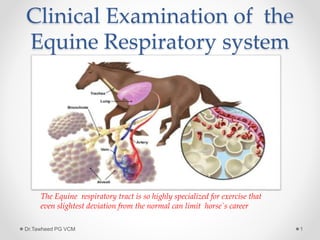
1. Clinical Examination of the
Equine Respiratory system
Dr.Tawheed PG VCM 1
The Equine respiratory tract is so highly specialized for exercise that
even slightest deviation from the normal can limit horse`s career
2. Anatomy and Physiology
Nostrils, nasal cavity
,pharynx, larynx, trachea
and lungs
Provides oxygen to blood,
Removes waste gases CO2
Dr.Tawheed PG VCM 2
The nose is for breathing, the mouth is for eating
3. What can we learn
Location of pathology
for example :- upper v/s lower
Pathophysiology
for example:- obstructive v/s restrictive
Etiology
for example:- infectious v/s allergic v/s parasitic
Dr.Tawheed PG VCM 3
4. What do we need to know
Signalment:- (Age, Breed, sex)
In examining the equine respiratory system, the only
one of these that really matters is AGE
Rhodococcus equi infection occurs in foals
between 3 weeks to 5 month of age
COPD is disease of adult horse
Dr.Tawheed PG VCM 4
7. History
History is exceptionally important.
We should make sure to note the following:
• Involvement of individual or multiple animals
• Onset ( slow progressive to per acute)
• Duration(hrs, days, weeks, months years)
• Seasonality
• Association with time of feeding
• Out door environment( dust, pollutants. toxins)
• Hygiene of the indoor environment( tobacco smoke,
ventilation, dust exposure mold,)
• Anthelmintics
• Recent travel/transport
• Previous medication and response to treatment
Dr.Tawheed PG VCM 7
8. Physical examination
The respiratory physical exam should begin by observing
the horse from a distance. This should be done in a quiet
area, noting breathing pattern, stance, sneezing, coughing,
respiratory rate and respiratory effort. This is ideal time to
take history
Dr.Tawheed PG VCM 8
9. First Examine the Nostrils
Dr.Tawheed PG VCM 9
Flared nostrils can indicate pain or
increased effort to bring in air
Check both nostrils for presence of
airflow and whether or not it is equal on
both sides
10. Nostrils
Dr.Tawheed PG VCM 10
Any nasal exudates should be noted.
Important considerations are:
unilateral/bilateral, +/- blood, color,
consistency. Examine the alar fold for any
abnormalities or masses
11. Examine the mouth
Dr.Tawheed PG VCM 11
It is important to check the nostrils and
mouth for odor since this is often
associated with the presence of anaerobic
bacteria which may be contributing to an
infection. This is also a good time to listen
to the horse’s breathing, noting any
abnormal masses
Also check the oral and nasal mucous
membrane color.
12. Examine the Inter mandibular
lymph Nodes
Dr.Tawheed PG VCM 12
Palpate the inter mandibular lymph nodes,
noting any enlargement or painful
response to palpation.
14. Percuss the Sinuses
Dr.Tawheed PG VCM 14
Percuss the sinuses. Resonance will be greatly increased if the
tongue is held out of the mouth while percussing. Compare the
resonance on both sides while also noting if the horse seems
painful or objects to this procedure. Also check for facial
symmetry, general attitude and expression
15. Palpate the larynx
Dr.Tawheed PG VCM 15
Palpate the dorsal aspect of the larynx on
both sides noting any asymmetry or
muscle atrophy. If laryngeal hemiplegia is
present the muscular process of the
arytenoid cartilage may feel more
pronounced with muscle atrophy
16. Auscultate and palpate the
trachea
Dr.Tawheed PG VCM 16
Palpate the trachea for any abnormalities
such as irregular cartilage rings or
fractures.
The trachea can also be ausculted for any
abnormal sounds.
17. Examine the jugular vein
Dr.Tawheed PG VCM 17
Examine the jugular veins for patency and
filling. This is a good estimation of
hydration status along with checking skin
turgor. Any distention or pulsation of the
jugular veins may indicate a pleural
effusion or cranial thoracic mass
obstructing the return of blood flow to the
heart
18. Examine the Ventral
Thorax and Abdomen
Dr.Tawheed PG VCM 18
Check for any edema along the ventral
thorax and abdomen. A pleural effusion
can inhibit blood flow from the ventrum of
the thorax, leading to ventral edema.
20. Auscultate the Lungs
Dr.Tawheed PG VCM 20
A rebreathing bag may be used to help cause
the horse to breathe more deeply when lung
sounds are quiet. Make sure to hold the bag
away from the nose so that it does not block
the nostrils and thereby inhibit inspiration.
Also note how well the horse tolerates this
procedure and whether or not any coughing is
elicited, as well as how quickly the horse
recovers after the bag is removed.
21. Normal lung sounds
Bronchial sound- generated in the large air ways
Vesicular sounds- generated in the large airways, but
heard peripherally after attenuation through aerated
parenchyma
Dr.Tawheed PG VCM 21
22. Abnormal lung sounds
Changes in sound transmission
Consolidated areas- lung sounds will be louder, because
sounds carried more efficiently
Pleural effusion- lung sounds will be quieter, but heart
sounds will be louder
Pneumothorax- Both lung and heart sounds will sound
quieter
Increased inspiratory sounds- extra thoracic or large
airways obstruction
Increased expiratory sounds- lower air way obstruction
Other abnormal lung sounds- Crackles, wheezes
Dr.Tawheed PG VCM 22
23. Ancillary Diagnostic test
Arterial blood gas analysis
Arterial blood gas determinations are the most sensitive
indicator of respiratory function readily available to the
clinician.
Dr.Tawheed PG VCM 23
24. Arterial blood gas analysis
• Ventilation is best assessed using PaCO2 as a guide
• Decreased alveolar ventilation results in
hypercapnia(respiratory acidosis, )
• Cause of low PaO2 include hypo ventilation, right to left
intra pulmonary shunt, ventilation – perfusion mismatch,
and decreased diffusion capacity.
• The shunts responds poorly to oxygen supplementation
as opposed to other cause
• Ventilation perfusion-mismatch responds well to oxygen
supplementation
Dr.Tawheed PG VCM 24
25. Macroscopic tests
Endoscopy
The nasal passage , naso maxillary meatus opening,
pharynx, larynx, trachea ,main stem bronchi, segmental
and sub-segmental bronchi are accessible
Endoscope ranges from 15mm to 2-3mm outer diameter
Dr.Tawheed PG VCM 25
29. Macroscopic test
• Radiography
Indication for radiography include auscultaion of adventitios
sounds (wheezes,crackles, absence of sounds),abnormal
percussion of the sinuses or chest, dyspnea , chronic
cough, external chest trauma exercise intolerance,
cyanosis
Dr.Tawheed PG VCM 29
33. Macroscopic test
• Thoracic USG
The USG Is an excellent technique to investigate pleural
effusion, diaphragmatic herniation ,lung consolidation,
atelectasis , but not broncheictasis
Dr.Tawheed PG VCM 33
35. Macroscopic test
Pulmonary Function test
These tests are aimed at describing the mechanical
function or gas exchange capacity of the respiratory
system. PFT are indicated where there is air ways
obstruction or restrictive lung disease where more
characterization is required
Dr.Tawheed PG VCM 35
36. Microscopic sampling
• Respiratory cytology
The indication for recovering respiratory secretions for
cytological evaluation are inflammation, infection, and
neoplasia
In general, when infection of the lower respiratory tract is
suspected, an aspirate of tracheal secretion(tracheal
aspirate, tracheal wash or TTA) is indicated
If disease produce is more profuse, chronic, peripherally
located lesion that is non-infectious(e.g allergic,
inflammatory,neoplasia) a more peripheral sampling
method is indicated. This can be achieved by
brochoalveolar lavage(BAL)
Dr.Tawheed PG VCM 36
39. Thoracocentesis
Indication for thoracocentesis is pleural effusion.
The procedure should be carried out under sterile condition.
The site is usually as ventral
as possible at the 8-10th
intercoastal space to avoid
heart. If sampling and therapeu-
-tic drainage is required , a
large bore canula(chest tube)
is placed to remove exudate. Gen-
-erally less 5000 cells per microliter &
protein less than 25 g/l
are considered normal
Dr.Tawheed PG VCM 39