• Rate of Miscarriage Following Chorionic Villus Sampling on 315 for Prenatal Diagnosis of Thalassaemia
•
0 gefällt mir•332 views

Poster Presented at RCOG World Congress, 2014 held at Hyderabad International COnvention Centre (HICC), Hyderabad, India

Empfohlen
Weitere ähnliche Inhalte
Was ist angesagt?
Was ist angesagt? (20)
Ähnlich wie • Rate of Miscarriage Following Chorionic Villus Sampling on 315 for Prenatal Diagnosis of Thalassaemia
Ähnlich wie • Rate of Miscarriage Following Chorionic Villus Sampling on 315 for Prenatal Diagnosis of Thalassaemia (20)
Mehr von Sujoy Dasgupta
Mehr von Sujoy Dasgupta (20)
Kürzlich hochgeladen
Kürzlich hochgeladen (20)
• Rate of Miscarriage Following Chorionic Villus Sampling on 315 for Prenatal Diagnosis of Thalassaemia
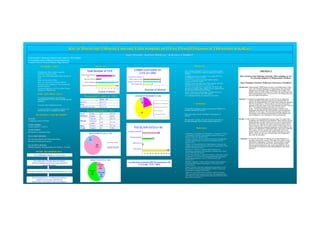
- 1. Rate of Miscarriage Following Chorionic Villus Sampling on 315 for Prenatal Diagnosis of ThalassemiaRate of Miscarriage Following Chorionic Villus Sampling on 315 for Prenatal Diagnosis of Thalassemia in Kolkatain Kolkata Sujoy DasguptaSujoy Dasgupta11, Kanchan Mukherjee, Kanchan Mukherjee22, Kalyansree Chaudhuri, Kalyansree Chaudhuri33 1 Senior Resident, Chittaranjan National Cancer Institute (CNCI), Kolkata 2 Corresponding Author (mukherjee.kanchan@gmail.com) 3 Assistant Professor, Burdwan Medical College, Burdwan INTRODUCTIONINTRODUCTION • Thalassaemia- Most common congenital haemolytic anaemia in India • Every year 10,000 thalassaemic babies are born in India • Huge socio-economic burden • Only way of prevention- Prenatal diagnosis • Chorionic Villus Sampling (CVS) provides early prenatal diagnosis • Commonest indication of CVS in India- Prenatal diagnosis of Thalassaemia1 AIMS AND OBJECTIVESAIMS AND OBJECTIVES • To assess the miscarriage rates following transabdominal CVS for women carrying singleton pregnancy • To assess other complications,if any • To assess its effect on pregnancy outcome with special reference to congenital anomalies MATERIALS AND METHODSMATERIALS AND METHODS SETTINGSETTING A diagnostic centre in Kolkata STUDY PERIODSTUDY PERIOD 2 years (Aug 2011- Jul 2013) STUDY DESIGNSTUDY DESIGN Retrospective Longitudinal Study INCLUSION CRITERIAINCLUSION CRITERIA Previous baby affected with Thalassaemia Major Both parents Thalassaemia carriers EXCLUSION CRITERIAEXCLUSION CRITERIA Multiple pregnancy, Bleeding diathesis & Gestation > 20 weeks STUDY METHODOLOGYSTUDY METHODOLOGY Written Informed Consent from all participants Trans-abdominal CVS under direct US guidance with local anaesthesia taking strict aseptic precautions by a single operator Discharged immediately with broad spectrum antibiotics for 5 days Direct Questionnaire at >3 months post-procedure re vaginal loss, miscarriage, fetal affection, preterm labour, limb reduction and missed diagnosis RESULTSRESULTS 0 50 100 150 200 250 300 350 Total No of CVS Performed CVS for Thalassaemia Nos Lost in Follow Up Number of Women Followed Up Total Number of CVS 320 315 56 259 Number of Women Demographic Variables (n = 315)Demographic Variables (n = 315) Procedural details (n = 315)Procedural details (n = 315) Mean + SD Age (yrs) 25.2 + 1.7 Parity 1.3 + 0.7 Gestational Age (wks) 12.4 + 2.8 No of Punctures Single 313 99.37% Double 2 0.63% Placenta Anterior 153 48.57% Posterior/ Lateral 162 51.43% Blood Group Positive 306 97.14% Negative 09 2.86% INDICATIONS OF CVS ( n- 315) 264 84% 51 16% Previous baby Thal Major No previous H/O Thal Major baby (parents Thal carrier) RESULTS OF CVS (n= 259) Thal major 53 20% Thal trait 58 22% Normal 148 58% 0 1 2 3 Miscarriage (0.39%) Leakage of Liquor (0.78%) Preterm Labour (0.78%) Congenital Anomaly (Nil) COMPLICATIONS OF CVS (n= 259) 1 2 2 Number of Women OUTCOME OF PREGNANCY (n= 259) 53 1 185 20 Termination due to Thal affected baby (20%) Miscarriage (0.4%)- within 6 days of CVS Delivery of Live Baby (71%) Continuing pregnancy >24 wk(7%) 0 20 40 60 80 100 120 140 160 180 200 Total No of Delivery Baby Not living (1%) Thal Status Checked (40%) Thal Status Not Checked (58%) POST-DELIVERY STATUS (n= 185) 185 2 75 108 Corroboration of postnatal Hb Electrophoresis with CVS results- 75/75 = 100% DiscussionDiscussion • Most common indication of CVS in our study is prenatal diagnosis of thalassemia- similar to studies by Choudry et al, 20122 • Sampling success rate was 100% in our study (99.7% as per Williams J 3rd et al, 1992)3 • In 99.37% cases, there was single needle insertion, consistent with other studies3 • Fetal loss rate in our study was 0.32%, matches with data published in the literature (0.7%-1.65%)1,4,5 • The low miscarriage rate is explained by the theory that placenta is a spongy organ, capable of easy expansion after the procedure, allowing early healing6 • Minor complications (like leakage of fluid) occurred in 0.64% cases consistent with other studies1 • No congenital anomaly was reported in our cohort ConclusionsConclusions • CVS has the advantage of making early prenatal diagnosis of hereditary haemolytic anaemia • Allows the option of early termination of pregnancy if required • The procedure is simple, safe, low cost and can be done at the ultrasonography clinic without inpatient admission ReferencesReferences 1. Laksanavilai U, Piyamongkol W, Sirichotiyakul S, Tongprasert F, Leuwan S, Srisupundit K. Chorionic villous sampling: experience of 636 cases. J Med Assoc Thai. 2013 Apr;96(4):383-8 2. Choudry A, Masood S, Ahmed S. Feasibility and safety of transabdominal Chorionic Villus Sampling. J Ayub Med Coll Abbottabad. 2012 Jan- Mar;24(1):38-43 3. Williams J 3rd, Wang BB, Rubin CH, Aiken-Hunting D. Chorionic villus sampling: experience with 3016 cases performed by a single operator. Obstet Gynecol. 1992 Dec;80(6):1023-9 4. Mujezinovic F, Alfirevic Z. Procedure-related complications of amniocentesis and chorionic villous sampling: a systematic review. Obstet Gynecol. 2007 Sep;110(3):687-94 5. Scott F, Peters H, Boogert T, Robertson R, Anderson J, McLennan A, Kesby G, Edelman D. The loss rates for invasive prenatal testing in a specialised obstetric ultrasound practice. Aust N Z J Obstet Gynaecol. 2002 Feb;42(1):55-8 6. Dhaifalah I, Zapletalova J. Safety and risks associated with screening for chromosomal abnormalities during pregnancy. Ceska Gynekol. 2012 Jun;77(3):236-41 7. Gogate S. Methods of fetal tissue sampling and prenatal diagnosis. In Pai HR, ed. Manual of Genetics and Fetal Medicine. Mumbai: Genetics and Fetal Medicine Committee FOGSI, 2006:22 8. Schaap AH, van der Pol HG, Boer K, Leschot NJ, Wolf H. Long-term follow-up of infants after transcervical chorionic villus sampling and after amniocentesis to compare congenital abnormalities and health status. Prenat Diagn. 2002 Jul;22(7):598-604 ABSTRACT Rate of miscarriage following chorionic villus sampling on 315 for prenatal diagnosis of Thalassemia in Kolkata Sujoy Dasgupta, Kanchan Mukherjee, Kalyansree Chaudhuri Introduction: Approximately 10000 babies are born with Thalassemia in India every year. Prenatal diagnosis of Thalassemia is the commonest indication for Chorionic Villus Sampling (CVS) in India. The primary objective of this study was to assess the miscarriage rates following transabdominal CVS for women with Thalassemia trait carrying singleton pregnancy. Methods: A retrospective longitudinal study was carried out at a diagnostic centre in Kolkata. Informed consents were obtained from all patients for transabodiminal CVS under direct ultrasonic guidance with local anaesthesia. All procedures were done by the same operator at the same clinic in two years between Aug 2011 and Jul 2013. The median gestation at the time of CVS was 12 weeks. All but two required single puncture. Patients were discharged immediately after the procedure on broad spectrum andibiotics for five days. Outcome data regarding vaginal loss, miscarriage, fetal affection, preterm labour, limb reduction and missed diagnosis were collected by direct questionnaire. Results: A total of 320 CVS were performed over two years. Five cases were excluded as the indications were different. Three of them were for Spinal Muscular Atrophy (SMA) and one each for Haemophilia and Sickle Cell Anaemia. 56 women were lost in follow up for various reasons. Other 259 women could be followed up, out of which 53 had already terminated pregnancy as their fetuses were shown to be affected by Thalassemia major. Out of the remaining 206 women, 185 have already delivered healthy babies and another 20 have crossed 24 weeks gestation but they are yet to deliver. There was one case of miscarriage which happened 6 days after the procedure. Conclusion: CVS has the advantage of making early prenatal diagnosis of hereditary haemolytic anaemia. This allows the option of early termination of pregnancy if required. The procedure is simple, safe, low cost and can be done at the ultrasonography clinic without inpatient admission. Our results especially the rate of miscarriage is consistent with the data published in the world literature.