2. INTRODUCTION
• COPD may include diseases that cause airflow obstruction (e.g.,
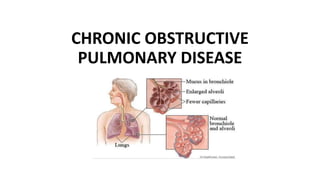
emphysema, chronic bronchitis) or a combination of these disorders.
• Chronic bronchitis: is a chronic inflammation of the lower
respiratory tract characterized by excessive mucous secretion, cough,
& dyspnea (at least 3 months in each of 2 consecutive year).
• Emphysema: is a complex lung disease characterized by damage to
the gas- exchanging surfaces of the lungs (alveoli)
5. RISK FACTORS FOR COPD
• Exposure to tobacco smoke accounts for an estimated 80% to 90% of
COPD cases. (smoking)
• Passive smoking
• Occupational exposure
• Air pollution
• Genetic abnormalities, including a deficiency of alpha1-antitrypsin
enzyme.
6. PATHOPHYSIOLOGY
Abnormal inflammatory response of the lungs due to toxic gases.
Response occurs in the airways, parenchyma & pulmonary vasculature
Narrowing of the airway takes place.
Destruction of parenchyma leads to emphysema.
Destruction of lung parenchyma leads to an imbalance of
proteinases/anti-proteinases. (this proteinases inhibitors prevents the
destructive process)
7. CONT..
Pulmonary vascular changes
Thickening of vessels
Collagen deposit
Destruction of capillary beds
Mucus hypersecretion (cilia dysfunction, airflow limitation, cor-
pulmonale (RVF)
Chronic cough and sputum production
8. CLINICAL MANIFESTATIONS
• COPD is characterized by three primary symptoms:
1. Cough
2. Sputum production and
3. Dyspnea on exertion (DOE)
• Dyspnea may be severe and often interferes with the patient’s
activities.
• Weight loss is common because dyspnea interferes with eating.
9. DIAGNOSTIC EVALUATION
1. History collection
• Exposure to risk factors—types, intensity, duration.
• Past medical history—respirator diseases including asthma, allergy,
sinusitis, nasal polyps, history of respiratory Infections.
• Family history of COPD or other chronic respiratory diseases.
• Pattern of symptom development.
• History of exacerbations or previous hospitalizations for respiratory
problems.
• Presence of comorbidities
• Available social and family support for patient
10. CONT..
2. Pulmonary function studies: to help confirm the diagnosis of
COPD.
3. Spirometry: to evaluate airflow obstruction.
4. Arterial blood gas (ABGs): to assess baseline oxygenation and gas
exchange
5. Chest x-ray
6. Alpha1antitrypsin deficiency screening: for patients under age 45
or for those with a strong family history of COPD.
11. MANAGEMENT
The objectives of treatment are
• Relieve symptoms
• Prevent disease progression
• Reduce mortality & improve exercise tolerance
• Prevent and treat complications
12. CONT..
1. Risk reduction:
• Smoking cessation
• yearly influenza vaccine and the pneumococcal vaccine
every 5 to 7 years as preventive measures.
2. Management of exacerbation:
• Oxygen therapy
• Bronchodilators: relieve bronchospasm and reduce
airway obstruction. These medications are delivered
through a metered-dose inhaler (MDI) or by nebulization.
• Corticosteroids: Inhaled and systemic corticosteroids
(oral or intravenous) may also be used.
13. CONT..
3. Surgery
• Bullectomy
• Lung volume reduction surgery
• Lung transplantation
4. Pulmonary rehabilitation: The primary goal of rehabilitation is to
restore patients to the highest level of independent function possible
and to improve their quality of life.
• Education
• General exercise training
• Breathing retraining
• Outcome assessment
• Nutritional advise
• Psychological support
14. NURSING MANAGEMENT
1. Ineffective breathing pattern related to chronic airflow limitation.
2. Ineffective airway clearance related to bronchoconstriction, increased
mucus production, ineffective cough, possible bronchopulmonary
infection.
3. Risk for infection related to compromised pulmonary function, retained
secretions and compromised defense mechanisms.
4. Imbalanced nutrition: less than body requirements related to poor intake,
presenting dyspnea & drug effects.
5. Deficient knowledge of self-care strategies to be performed at home
19. DEFINITION
Pneumothorax is an abnormal collection
of air or gas in the pleural space
separating the lung from the chest wall
which may interfere with normal
breathing, causing the lungs to collapse.
21. Spontaneous pneumothorax
1. Primary: It occurs in young healthy
individuals without underlying lung disease.
It is due to the rupture of apical subpleural
bleb.
2. Secondary: occurs in the presence of pre-
existing lung pathology. Ex : Cystic fibrosis,
COPD, Asthma, pneumonia, Lung cancer.
22. Traumatic pneumothorax
1. Open: Chest wall is damaged by any wound, outside air enters
pleural space and causes lungs to collapse. Usually associated with
hemothorax. E.g. Penetrating trauma: stab wound or gun shot injury.
2. Closed: nonpenetrating chest trauma such as rib fracture can
lacerates the lung or a ruptured bronchus cause air to leaks into
pleural space.
3. Iatrogenic: Postoperative Mechanical ventilation, Thoracocentesis
& Central venous cannulation.
23. Tension pneumothorax
• It is life threatening condition. The pleural pressure is more than the
atmospheric pressure.
• It occurs when site of air leak acts as one way valve, air enters pleural
space during inspiration but cannot escape during expiration.
• Volume of air and intrapleural pressure increasingly elevated results in
compression of lung on the affected side.
• Mediastinal shift towards the unaffected side, compressing the good
lung which further compromises oxygenation.
24. Cont..
• Possible shift of trachea, pressure on the heart and great vessels,
resulting in decreased venous return and cardiac output.
• Associated with clinical manifestations of circulatory collapse
(tachycardia, hypotension & sweating).
• It is more common with Positive pressure ventilation & Traumatic
pneumothorax.
25.
26. RISK FACTORS
• Sex : men are far more likely to have a pneumothorax than are women.
• Smoking.
• Age: The type of pneumothorax caused by ruptured air blisters is most
likely to occur in people between 20 and 40 years old, especially if the
person is very tall & underweight man.
• Genetics.
• Lung disease
• Mechanical ventilation.
• A history of pneumothorax.
27. PATHOPHYSIOLOGY
• In normal people, the pressure in pleural space is negative during the
entire respiratory cycle.
• Two opposite forces result in negative pressure in pleural space (outward
pull of the chest wall and elastic recoil of the lung).
• The negative pressure will be disappeared if any communication
develops between an alveolus or other intrapulmonary air space and
pleural space.
• Air will flow into the pleural space until there is no longer a pressure
difference or the communication is sealed.
28.
29. CLINICAL FEATURES
• Predominant symptom is acute pleuritic chest pain
• Dyspnea results form pulmonary compression
• Breath sounds may be diminished on the affected side
• Percussion of the chest may be perceived as hyperresonant.
• Other signs include: Tachypnoea, Hypoxemia, Cyanosis, Hypercapnia.
31. DIAGNOSTIC EVALUATIONS
• History Collection
• Physical examination
• CT Scan: to identify underlying lung lesions.
• Chest X-ray: The characteristics of pneumothorax (Pleural line, lung
markings)
• Chest ultrasound
32. TREATMENT
Goals
• To promote lung expansion.
• To eliminate the pathogenesis.
• To decrease pneumothorax recurrence.
Treatment options :
• Simple aspiration
• Intercostal tube drainage
• Trocar tube thoracostomy
• Surgical treatment: pleurodesis, pneumonectomy
33. Simple aspiration
• The aspiration can be done by needle or
catheter
• A volume of < 2.5 L has been aspirated
on the first attempt
• Repeated aspiration is reasonable for
primary pneumothorax when the first
aspiration has been unsuccessful.
34. Trocar tube thoracostomy
• Insertion of trocar into the pleural space.
• Insertion of the chest tube through the trocar
35. Intercostal tube drainage
• A common site of chest tube insertion is in
the 2nd ICS in midclavicular line.
• An alternative site now commonly used is
midaxillary line of 4th and 5th intercostal
space for cosmetic reason and also for
when pleural effusion.
36. Observation of drainage
• No bubble released
oThe lung re-expansion
oThe chest tube is obstructed by secretion or blood clot
oThe chest tube shift to chest wall, the hole of the chest tube is located
in the chest wall.
• If the lung re expanded, removing the chest tube 24 hours after re
expansion. Otherwise, the chest tube will be inserted again or regulated
the position