All posters gl2010_english
•
4 gefällt mir•4,221 views

The document provides guidelines for basic and advanced life support from the European Resuscitation Council. It outlines the steps for assessing an unresponsive victim and providing CPR, including calling for help, checking breathing and pulse, opening the airway, delivering rescue breaths and chest compressions, using an AED if available, and treating reversible causes of cardiac arrest. It also describes treating shockable and non-shockable heart rhythms, minimizing interruptions to chest compressions, considering advanced airways and vascular access, and focusing on high-quality CPR when performing advanced life support.

Empfohlen
Empfohlen
Weitere ähnliche Inhalte
Was ist angesagt?
Was ist angesagt? (20)
Ähnlich wie All posters gl2010_english
Ähnlich wie All posters gl2010_english (20)
Mehr von Shery Hassan
Kürzlich hochgeladen
Kürzlich hochgeladen (20)
All posters gl2010_english
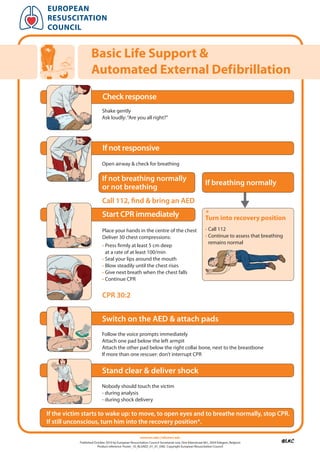
- 1. european resuscitation council Basic life support & automated external Defibrillation Check response Shake gently Ask loudly: “Are you all right?” If not responsive Open airway & check for breathing If not breathing normally If breathing normally or not breathing Call 112, find & bring an AED Start CPR immediately * turn into recovery position Place your hands in the centre of the chest • Call 112 Deliver 30 chest compressions: • Continue to assess that breathing remains normal • Press firmly at least 5 cm deep at a rate of at least 100/min • Seal your lips around the mouth • Blow steadily until the chest rises • Give next breath when the chest falls • Continue CPR CPR 30:2 Switch on the AED & attach pads Follow the voice prompts immediately Attach one pad below the left armpit Attach the other pad below the right collar bone, next to the breastbone If more than one rescuer: don’t interrupt CPR Stand clear & deliver shock Nobody should touch the victim - during analysis - during shock delivery If the victim starts to wake up: to move, to open eyes and to breathe normally, stop CPR. If still unconscious, turn him into the recovery position*. www.erc.edu | info@erc.edu Published October 2010 by European Resuscitation Council Secretariat vzw, Drie Eikenstraat 661, 2650 Edegem, Belgium Product reference: Poster_10_BLSAED_01_01_ENG Copyright European Resuscitation Council
- 2. european resuscitation council in-hospital resuscitation Collapsed/sick patient Shout for HELP & assess patient If NO signs of life If signs of life Call resuscitation team Assess ABCDE Recognise & treat CPR 30:2 Oxygen, monitoring, iv access with oxygen and airway adjuncts Call resuscitation team If appropriate Apply pads/monitor Handover to resuscitation team Attempt defibrillation if appropriate advanced life support when resuscitation team arrives www.erc.edu | info@erc.edu Published October 2010 by European Resuscitation Council Secretariat vzw, Drie Eikenstraat 661, 2650 Edegem, Belgium Product reference: Poster_10_IHBLS_01_01_ENG Copyright European Resuscitation Council
- 3. euRopean ResuscItatIon councIl In-hospital Resuscitation Collapsed/sick patient Shout for HELP & assess patient No Signs of life? Yes Call resuscitation team Assess ABCDE Recognise & treat Oxygen, monitoring, iv access CPR 30:2 with oxygen and airway adjuncts Call resuscitation team Apply pads/monitor If appropriate Attempt defibrillation if appropriate Advanced Life Support Handover to resuscitation team when resuscitation team arrives www.erc.edu | info@erc.edu | Published October 2010 by European Resuscitation Council Secretariat vzw, Drie Eikenstraat 661, 2650 Edegem, Belgium | Product reference: Poster_10_IHBLS-A_01_01_ENG Copyright European Resuscitation Council
- 4. european resuscitation council advanced life support Universal Algorithm Unresponsive? Not breathing or only occasional gasps Call Resuscitation Team CPR 30:2 Attach defibrillator/monitor Minimise interruptions Assess rhythm Shockable Non-shockable (VF/Pulseless VT) (PEA/Asystole) Return of 1 Shock spontaneous circulation Immediately resume: immEDiATE PoST CArDiAC Immediately resume: ArrEST TrEATmENT CPR for 2 min CPR for 2 min • Use ABCDE approach Minimise interruptions • Controlled oxygenation and Minimise interruptions ventilation • 12-lead ECG • Treat precipitating cause • Temperature control / therapeutic hypothermia DuriNg CPr rEVErSiblE CAuSES • Ensure high-quality CPR: rate, depth, recoil • Hypoxia • Plan actions before interrupting CPR • Hypovolaemia • Give oxygen • Hypo-/hyperkalaemia/metabolic • Consider advanced airway and capnography • Hypothermia • Continuous chest compressions when advanced airway in place • Thrombosis • Vascular access (intravenous, intraosseous) • Tamponade - cardiac • Give adrenaline every 3-5 min • Toxins • Correct reversible causes • Tension pneumothorax www.erc.edu | info@erc.edu Published October 2010 by European Resuscitation Council Secretariat vzw, Drie Eikenstraat 661, 2650 Edegem, Belgium Product reference: Poster_10_ALS_01_01_ENG Copyright European Resuscitation Council
- 5. european resuscitation council advanced life support Bradycardia Algorithm • Assess using the ABCDE approach • Ensure oxygen given and obtain IV access • Monitor ECG, BP, SpO2, record 12 lead ECG • Identify and treat reversible causes (e.g. electrolyte abnormalities) Assess for evidence of adverse signs: 1 Shock Yes 2 Syncope No 3 Myocardial ischaemia 4 Heart failure Atropine 500 mcg IV Satisfactory Yes Response? No risk of asystole? • Recent asystole Yes • Möbitz II AV block • Complete heart block with broad QRS • Ventricular pause > 3s interim measures: • Atropine 500 mcg IV repeat to maximum of 3 mg No • Isoprenaline 5 mcg min-1 • Adrenaline 2-10 mcg min-1 • Alternative drugs* or • Transcutaneous pacing Seek expert help observe Arrange transvenous pacing * Alternatives include: • Aminophylline • Dopamine • Glucagon (if beta-blocker or calcium channel blocker overdose) • Glycopyrrolate can be used instead of atropine www.erc.edu | info@erc.edu Published October 2010 by European Resuscitation Council Secretariat vzw, Drie Eikenstraat 661, 2650 Edegem, Belgium Product reference: Poster_10_ALS-BRAD_01_01_ENG Copyright European Resuscitation Council
- 6. euRoPeAN ReSuSCITATIoN CouNCIL Advanced Life Support Tachycardia Algorithm • Assess using the ABCDE approach • Ensure oxygen given and obtain IV access • Monitor ECG, BP, SpO2 , record 12 lead ECG • Identify and treat reversible causes (e.g. electrolyte abnormalities) Assess for evidence of adverse signs Synchronised DC Shock* Unstable 1. Shock 2. Syncope Stable Is QRS narrow (< 0.12 sec)? Up to 3 attempts 3. Myocardial ischaemia 4. Heart failure • Amiodarone 300 mg IV over 10-20 min and repeat shock; Broad Narrow followed by: • Amiodarone 900 mg over 24 h Broad QRS Narrow QRS Irregular Regular Regular Irregular Is QRS regular? Is rhythm regular? Seek expert help • Use vagal manoeuvres Irregular Narrow Complex • Adenosine 6 mg rapid IV bolus; Tachycardia if unsuccessful give 12 mg; Probable atrial fibrillation if unsuccessful give further 12 mg. Control rate with: • Monitor ECG continuously • ß-Blocker or diltiazem • Consider digoxin or amiodarone if evidence of heart failure Anticoagulate if duration > 48h Possibilities include: If Ventricular Tachycardia Normal sinus rhythm restored? No Seek expert help • AF with bundle branch block (or uncertain rhythm): treat as for narrow complex • Amiodarone 300 mg IV over • Pre-excited AF 20-60 min; then 900 mg over 24 h Yes consider amiodarone • Polymorphic VT If previously confirmed (e.g. torsades de pointes - SVT with bundle branch block: give magnesium 2 g over 10 min) • Give adenosine as for regular narrow complex tachycardia Probable re-entry PSVT: Possible atrial flutter • Record 12-lead ECG in sinus rhythm • Control rate (e.g. ß-Blocker) • If recurs, give adenosine again & consider choice of anti-arrhythmic *Attempted electrical cardioversion is always undertaken under sedation or general anaesthesia prophylaxis www.erc.edu | info@erc.edu | Published October 2010 by European Resuscitation Council Secretariat vzw, Drie Eikenstraat 661, 2650 Edegem, Belgium | Product reference: Poster_10_ALS-TACH_01_01_ENG Copyright European Resuscitation Council
- 7. euroPean resuscitation counciL Paediatric Basic Life support Health professionals with a duty to respond UNRESPONSIVE? Shout for help Open airway NOT BREATHING NORMALLY? 5 rescue breaths NO SIGNS OF LIFE? 15 chest compressions 2 rescue breaths 15 compressions After 1 minute of CPR call national emergency number (or 112) or cardiac arrest team www.erc.edu | info@erc.edu Published October 2010 by European Resuscitation Council Secretariat vzw, Drie Eikenstraat 661, 2650 Edegem, Belgium Product reference: Poster_10_PaedBLS_01_01_ENG Copyright European Resuscitation Council
- 8. euroPean reSuScitation counciL Paediatric Life Support Advanced Life Support Unresponsive? Not breathing or only occasional gasps CPR (5 initial breaths then 15:2) Call Resuscitation Attach defibrillator/monitor Team Minimise interruptions (1 min CPR first, if alone) Assess rhythm Shockable Non-shockable (VF/Pulseless VT) (PEA/Asystole) Return of 1 Shock 4 J/Kg spontaneous circulation Immediately resume: immEDiATE PoST CArDiAC Immediately resume: ArrEST TrEATmENT CPR for 2 min CPR for 2 min • Use ABCDE approach Minimise interruptions • Controlled oxygenation and Minimise interruptions ventilation • Investigations • Treat precipitating cause • Temperature control • Therapeutic hypothermia? DuriNg CPr rEVErSiblE CAuSES • Ensure high-quality CPR: rate, depth, recoil • Hypoxia • Plan actions before interrupting CPR • Hypovolaemia • Give oxygen • Hypo-/hyperkalaemia/metabolic • Vascular access (intravenous, intraosseous) • Hypothermia • Give adrenaline every 3-5 min • Tension pneumothorax • Consider advanced airway and capnography • Toxins • Continuous chest compressions when advanced airway in place • Tamponade - cardiac • Correct reversible causes • Thromboembolism www.erc.edu | info@erc.edu Published October 2010 by European Resuscitation Council Secretariat vzw, Drie Eikenstraat 661, 2650 Edegem, Belgium Product reference: Poster_10_PALS_01_01_ENG Copyright European Resuscitation Council
- 9. europeaN reSuScitatioN couNciL At ALL StAGES ASk: DO yOu NEED HELP? Newborn Life Support Dry the baby Birth Remove any wet towels and cover Start the clock or note the time Assess (tone), 30 sec breathing and heart rate If gasping or not breathing Open the airway Give 5 inflation breaths Consider SpO2 monitoring 60 sec Re-assess If no increase in heart rate Look for chest movement if chest not moving Acceptable pre-ductal SpO2 Recheck head position 2 min: 60% Consider two-person airway control 3 min: 70% or other airway manoeuvres 4 min: 80% Repeat inflation breaths Consider SpO2 monitoring 5 min: 85% Look for a response 10 min: 90% If no increase in heart rate Look for chest movement When the chest is moving If the heart rate is not detectable or slow (< 60) Start chest compressions 3 compressions to each breath Reassess heart rate every 30 seconds If the heart rate is not detectable or slow (< 60) Consider venous access and drugs www.erc.edu | info@erc.edu Published October 2010 by European Resuscitation Council Secretariat vzw, Drie Eikenstraat 661, 2650 Edegem, Belgium Product reference: Poster_10_NLS_01_01_ENG Copyright European Resuscitation Council