
Empfohlen
Empfohlen
Weitere ähnliche Inhalte
Was ist angesagt?
Was ist angesagt? (20)
Ähnlich wie Post Natal Growth & Development
Ähnlich wie Post Natal Growth & Development (20)
Mehr von Saibel Farishta
Mehr von Saibel Farishta (20)
Kürzlich hochgeladen
Kürzlich hochgeladen (20)
Post Natal Growth & Development
- 1. Post Natal Growth And Development PROF (Dr.) SAIBEL FARISHTA
- 2. There are many treatment modalities that can be initiated during the growing age. Post Natal Growth Of The Cranial Base The maxilla is attached to the cranial base by means of a number of sutures. The mandible is also attached to the cranial base at the TMJ. Thus growth processes occuring at the cranial base can affect the placement of maxilla and mandible. The cranial base grows post-natally by – cortical drift and remodelling, elongation at synchondroses and by sutural growth. Remodeling And Cortical Drift Remodeling refers to a process where bone deposition and resorption occurs so as to bring about change in size, shape and relationship of the bone. The cranium is divided into a number of compartments by bony elevations and ridges present in the cranial base. These elevated ridges and bony partitions show bone deposition, while the predominant part of the floor shows bone resorption. This intracranial bone resorption helps in increasing the intracranial space to accommodate the growing brain.
- 3. The cranial base is perforated by the passage of a number of blood vessels and nerves communicating with the brain. The foramina that allows these nerves and blood vessels undergo drifting by bone deposition and resorption so as to constantly maintain their relationship with the growing brain.
- 4. Most of the bones of the cranial base are formed by a cartilagenous process. Later the cartilage is replaced by bone. Certain bands of cartilage remain at the junction of various bones, these areas are called Synchondroses. These are primary cartilages and important growth sites of the cranial base. Important Synchondroses found in the cranial base are – Spheno-occipital, Spheno-ethmoidal, Inter-sphenoid and Intra-occipital synchondrosis. Elongation At The Synchondrosis • Spheno-occipital Synchondrosis – It is the cartilaginous junction between the sphenoid and the occipital bones. It is believed to be the most important and principal growth cartilage of the cranial base during childhood. It is believed to be active upto 12-15 years of age. At 20 years of age, the sphenoid and occipital segments then fuse in the midline. It provides a pressure or compression adapted bone growth, in contrast to tension adapted growth seen in sutures. This is because the cranial base supports the weight of the brain and face which bears down on the synchondrosis in the midline of the vranial base. As endochondral bone growth occurs at the spheno-occipital synchondrosis, the sphenoid and occipital bones are moved apart.
- 5. At the same time new endochondral bone is laid down in the medullary region and cortical bone is formed in the endosteal and periosteal regions. Thus the sphenoid and occipital bones increase in length and width. The direction of growth of the spheno occipital synchondrosis is upwards. It therefore carries the anterior part of the cranium bodily forwards. The growth at the synchondrosis continues till the obliteration of the same by formation of bone. Closure of the synchondrosis occurs at around 13-15 years of age.
- 6. • Spheno-ethmoid Synchondrosis – This is a cartilaginous band between the sphenoid and ethmoid bone. It ossifies by 5-25 years of age. • Inter-sphenoidal Synchondrosis – It is a cartilaginous band between the 2 parts of the sphenoid bone. It is believed to ossify at birth. • Intra-Occipital Synchondrosis – This ossifies by 3-5 years of age.
- 7. Sutural Growth The cranial base has a number of bones that are joined to one another by means of sutures. Some of the sutures that are present are – Spheno- frontal, Fronto-temporal, Spheno-ethmoid, Fronto-ethmoid and Fronto- zygomatic. As the brain enlarges during growth, bone formation occurs at the ends of the bone. Timing Of Cranial Base Growth • By Birth, 55-60% of adult size • By 4-7 years, 94% of adult size • By 8-13 years, 98% of adult size
- 8. Post Natal Growth Of Maxilla The growth of the naso-maxillary complex is produced by the following mechanisms – displacement, growth at sutures and surface remodeling. • Displacement – Maxilla is attached to the cranial base by means of a number sutures. Thus the growth of the cranial base has a direct bearing on the naso-maxillary growth. A passive or secondary displacement of the naso-maxillary complex occurs in a downward and forward direction as the cranial base grows. The passive displacement of the maxilla is an important growth mechanism during the primary dentiton years but becomes less important as growth of cranial base slows. A primary type of displacement is also seen in a forward direction. This occurs by growth of the maxillary tuberosity in a posterior direction. This results in the whole maxilla being carried anteriorly. The amount of this forward displacement equals the amount of posterior lengthening.
- 10. • Growth At Sutures – The maxilla is connected to the cranium and cranial base by a number of sutures, these are – Fronto-nasal, Fronto-maxillary, Zygomatico-temporal, Zygomatico-maxillary and Pterygo-palatine. These sutures are all oblique and more or less are parallel to each other. This allows the downward and forward repositioning of the maxilla as growth occurs at these sutures. As growth of the surrounding soft tissue occurs, the maxilla is carried downwards and forwards. This leads to opening up of space at the sutural attachments. New bone is now formed on either side of the suture. Thus the overall size of the bones on either side increases. Hence a tension related bone formation occurs at the sutures.
- 11. The following bone remodeling changes are seen in naso-maxillary complex – [i] Resorption occurs on the lateral surface of the orbital rim leading to lateral movement of the eye-ball. To compensate, there is bone deposition on the medial rim of the orbit and external surface of the lateral rim. [ii] The floor of the orbit faces superiorly, laterally and anteriorly. Surface deposition occurs here and results in growth in a superior, lateral and anterior direction. [iii] Bone deposition occurs along the posterior margin of the maxillary tuberosity. This causes lengthening of the dental arch and enlargement of the antero-posterior dimension of the entire maxillary body. This helps to accommodate the erupting molars. • Surface Remodeling – Massive remodeling of bone occurs by bone deposition and resorption, which increases the bone size, shape and its functional relationship.
- 12. [iv] Bone resorption occurs on the lateral wall of the nose leading to an increase in size of the nasal cavity. [v] Bone resorption is seen on the floor of the nasal cavity. To compensate, there is bone deposition on the palatal side. Thus s downward shift occurs leading to increase in maxillary height. [vi] The zygomatic bone moves in a posterior direction. This is achieved by resorption on the anterior surface and deposition on the posterior surface. [vii] The face enlarges in width by bone formation on the lateral surface of the zygomatic arch and resorption on its medial surface. [viii] The ANS prominence increases due to bone deposition. [ix] As the teeth start erupting, bone deposition occurs at the alveolar margins. This increases the maxillary height and depth of the palate. [x] The entire wall of the sinus, except the mesial wall undergoes resorption. This results in increase in size of the maxillary antrum.
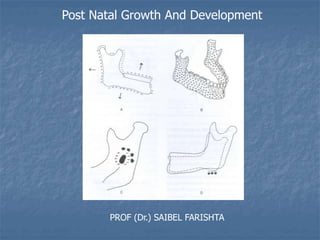
- 14. Post Natal Growth Of Mandible Of the facial bones, the mandible undergoes the largest amount of post natal growth and also exhibits the largest variability in morphology. While the mandible appears in the adult as a single bone, it is developmentally and functionally divisible into several skeletal sub-units. The basal bone or the body of the mandible forms one unit, to which is attached the alveolar process, the coronoid process, the condylar process, the angular process, ramus, lingual tuberosity and the chin. Ramus The ramus moves progressively posteriorly by combination of deposition and resorption. Resorption occurs on the anterior part and deposition on the posterior region. This results in a drift of the ramus posteriorly. The functions of remodeling of the ramus are: to accommodate the increasing mass of masticatory muscles inserted into it, to accommodate the enlarged breadth of the pharyngeal space and to facilitate the lengthening of the mandibular body, which in turn accomodates the erupting molars.
- 15. Corpus or Body Of Mandible The anterior border of the adult ramus exhibits bone resorption, while the posterior border shows bone deposition. The displacement of the ramus results in the conversion of former ramal bone into the posterior part of the body of mandible. In this manner the body of the mandible lendthens. Thus additional space made available by means of resorption of the anterior border of the ramus is made use of to accommodate the erupting permanent molars. Angle of The Mandible On the lingual side of the angle of mandible - resorption takes place on the posterio-inferior aspect, while deposition occurs on the antero-superior aspect. On the buccal side, resorption occurs on the anterio-superior part, while deposition takes place on the postero- superior part. This results in flaring of the angle of the mandible as age advances.
- 17. The Lingual Tuberosity The lingual tuberosity is a direct equivalent of the maxillary tuberosity, which forms a major site of growth for the lower bony arch. It forms the boundary between the ramus and the body. The lingual tuberosity moves posteriorly by deposition on it’s posteriorly facing surface. The lingual tuberosity protrudes in a lingual direction lies well towards the midline of the ramus. The prominence of the tuberosity is increased by the presence of a large resorption field just below it. This resorption field produces a depression, the lingual fossa. The combination of resorption in the fossa and depositionon the medial surface of the tuberosity itself accentuates the prominence of the lingual tuberosity. The Alveolar Process Alveolar process develops in response to the presence of tooth buds. As the teeth erupt the alveolar process develops and increases in height by bone deposition at the margins. The alveolar bone adds to the height and thickness of the body of the mandible and is manifested as a ledge extending lingual to the ramus to accommodate the 3rd molars. In case of absence of teeth, the alveolar bone fails to develop and it resorbs in the event of tooth extraction.
- 19. The Chin In infancy, the chin is usually under developed. As age advances the chin growth becomes significant. It is influenced by sexual and specific genetic factors. Usually males have prominent chin. The mental protuberance forms by bone deposition during childhood. Its prominence is accentuated by bone resorption that occurs in the alveolar region above it. The deepest point in this concavity is known as Point B. The Condyle The condyle is an important growth site. The condylar head is covered by a thin layer of cartilage called the condylar cartilage. The presence of condylar cartilage covering the condyle is an adaptation to withstand the compression that occurs at the joint. There are two schools of thought regarding the role of the condyle – • It was earlier believed that growth occurs at the surface of the condylar cartilage by means of bone deposition. Thus the condyle grows towards the cranial base. As the condyle pushes against the cranial base, the entire mandible gets displaced forwards and downwards.
- 20. • It is now believed that the growth of soft tissues including the muscles and connective tissues carries the mandible forwards away from the cranial base. Bone growth follows secondarily at the condyle to maintain constant contact with cranial base. The condylar growth rate increases at puberty reaching a peak between 12.5 – 14 years. The growth ceases around 20 years.
- 21. The Coronoid Process The growth of the coronoid process follows the enlarging ‘V’ principle. Viewing the longitidanal section posteriorly - deposition occurs on the lingual [medial] surfaces of the left and right coronoid process. Although additions take place on the lingual side, the vertical dimension of the coronoid process also increases. It follows the ‘V’ principle. From the occlusal aspect, the deposition on the lingual of the coronoid process brings about a posterior growth movement in the ‘V’ patern. Briefly, the coronoid process has a propeller like twist, so that its lingual side faces three general directions all at once – posteriorly, superiorly and medially.
- 22. THANK YOU