
Empfohlen
Weitere ähnliche Inhalte
Ähnlich wie poster presentation.pptx
Ähnlich wie poster presentation.pptx (20)
Mehr von Sadanand Indi
Mehr von Sadanand Indi (10)
Kürzlich hochgeladen
Kürzlich hochgeladen (20)
poster presentation.pptx
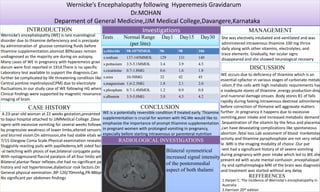
- 1. Wernicke’s Encephalopathy following Hyperemesis Gravidarum Dr.MOHAN Deparment of General Medicine,JJM Medical College,Davangere,Karnataka INTRODUCTION CASE HISTORY Wernicke’s encephalopathy (WE) is rare nuerological disorder due to thiamine defienciency and is precipate by administration of glucose containing fluids before thiamine supplementation.alomost 80%cases remain undiagnosed as the majority are during on autopsy. Many cases of WE in pregnancy with hyperemesis gravi darum were first reported in 1914.There is no specific Laboratory test available to support the diagnosis.Can further be complicated by life threatening condition like Central pontine myelinolysis(CPM) due to electrolyte fluctuations.In our study case of WE following HG where Clinical findings were supported by magnetic resonance imaging of brain A 23-year-old woman at 22 weeks gestation,presented to bapui hospital attached to JJMMedical College ,Dava ngere with excessive vomiting for several weeks followed by by progressive weakness of lower limbs,altered sensorium, and blurred vision.On admission,she had stable vitals with 7/15 Glasgow Coma Scale.Physical examination revealed Sluggishly reacting puils with papilledema,left sided faci -al twitching with ptosis of eye,bilateral conjugate palsy With nystagmusand flaccid paralysis of all four limbs with Bilateral plantar flexor reflexes.she had no significant past history and not hypertensive,diabeticor rosk factors.On General physical exmination ,BP-120/70mmhg,PR-88bpm, No significant per abdomen findings Investigations RADIOLOGICAL INVESTIGATIONS Tests Normal Range Day1 Day15 Day30 (per litre) s.chloride 98-107MMOL 96 98 106 s.sodium 137-145MMOL 129 131 140 s.pottasium 3.5-5.1MMOL 3.4 3.9 4.5 s.creatinine 0.7-1.8MG 0.6 1.6 1.8 s.urea 10-50MG 32 42 45 s.magnesium 1.6-2.3MG 1.8 2.1 2.0 s.phosphate 0.7-1.4MMOL 1.2 0.9 0.8 s.albumin 3.5-5.0MG 3.0 4.5 4.2 Bilateral symmetrical increased signal intensity of the posteromedial aspect of both thalami CONCLUSION MANAGEMENT She was electively intubated and ventilated and was administered intravenous thiamine 100 mg thrice daily along with other vitamins, electrolytes, and trace elements. Gradually, her ocular signs disappeared and she showed neurological recovery with improvement in muscle power. DISCUSSION WE occurs due to deficiency of thiamine which is an essential cpfactor in various stages of carbonate metab -olism.If the cells with high metabolic requirements hav e inadequte stores of thiamine ,energy production drop and nueronal damage ensues .Body stores B1 of falls rapidly during fasting.Intravenous dextrose adminitered before correction of thimaine will aggravate matters further .In pregnancy it happens due to excessive vomiting,poor intake and increased metabolic demand .Sequestration of the vitamin by the fetus and placenta ,can have devastating complications like spontaneous abortion ,fetal loss.Lab assesment of blood tranketolas activity and thiamine pyrophosphate are not very reliab le .MRI is the imaging modality of choice .Our pat -ient had a signoficant history of of severe vomiting during pregnancy with poor intake which led to WE.she present ed with acute mental confusion ,encephalopat -hy and opthalmoplegia.MRI of the brain was diagnostic and treatment was started without any delay WE is a potentially reversible condition if treated early. Thiamine supplementation is crucial for women with HG.We would like to emphasize the importance of prompt thiamine supplementation in pregnant women with prolonged vomiting in pregnancy, especially before starting intravenous or parenteral nutrition REFFERENCES 1.Harper C. The incidence of Wernicke's encephalopathy in Australia 2.Harrison 20th edition