2. 470
expression with the development of prostate cancer provide
potential targets for antisense or antigene methods of
therapy.
Cell-cycle control and apoptosis
Selective killing of prostate-cancer cells can be achieved by
manipulation of cell-cycle control or apoptosis. This
approach might involve delivery of genes that activate
prodrugs, tumour-suppressor genes, proapoptotic genes, or
antiangiogenic genes.
The strategy of prodrug activation (also known as the
suicide-gene strategy or genetic prodrug-activation therapy,
figure 3) introduces into target cells a gene that codes for a
drug-metabolising enzyme: target cells can convert a
systemically administered non-toxic prodrug into its toxic
form. Thus, prostate-cancer cells are
killed by the administration of prodrug
only when the appropriate gene coding
for a drug-metabolising enzyme is
present. Examples of prodrug
activation include the herpes simplex
virus gene for thymidine kinase
combined with ganciclovir prodrug,4
and the cytosine deaminase system
that converts flucytosine into
5-fluorouracil.5
The strategy of prodrug
activation has the advantage of being
less dependent on efficient gene
transfer than other approaches, owing
to the bystander effect of transduced or
transfected cells on neighbouring cells
that do not express the transgene.
Tumour regression was achieved by
use of cytosine deaminase and
flucytosine in human colorectal-cancer
cells, in which only 4% of tumour cells
contained the cytosine deaminase
gene.6
The combination of the herpes
simplex virus gene for thymidine
kinase and the prodrug ganciclovir (or
valaciclovir) has been used widely in
prostate cancer and other cancers, and
is the subject of six clinical trials on
prostate cancer.4,7,8–11
Other genes can also be used to
control cell proliferation, either directly
or indirectly. Tumour-suppressor
genes such as P53,12
and the proapop-
totic genes BAX13
and CASP9,14
inhibit
tumour growth if overexpressed from
vectors introduced into prostate-cancer
cells. Introduction of genes that code
for toxins such as diphtheria toxin A15
into prostate-cancer cells might also be
effective if specific delivery to cancer
cells can be achieved. Viral genes that
elicit toxic effects have also been
expressed in therapeutic vectors. For
example, adenoviral vectors have been
designed in which adenoviral genes needed for replication
are expressed in a prostate-specific manner, resulting in
tissue-specific adenoviral replication and cell lysis.16
Lastly,
there has been much interest in the role of angiogenesis in
tumour growth. For example, genes that encode
antiangiogenic proteins such as thrombospondin 1
indirectly inhibit the growth of prostate tumours in
immunodeficient mice.17
Activation of the immune system
Manipulation of the immune system to recognise tumour
cells as foreign antigens has been a long-term goal of many
immunotherapeutic approaches to cancer. Activation of an
immune response against tumour cells might be achieved by
expression of a tumour protein (eg, prostate-specific
Review Gene therapy for prostate cancer
Oncology Vol 5 August 2004 http://oncology.thelancet.com
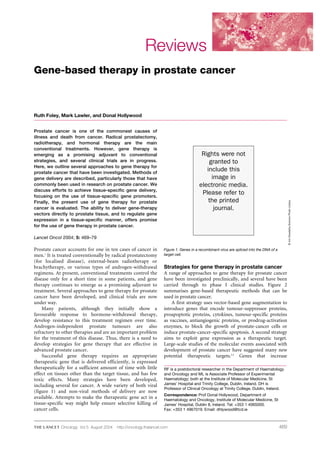
Antisense
oligonucleotide
(eg, MYC)
Triplex-forming
oligonucleotide
(eg, ETS2)
Small interfering RNA
(eg, EZH2)
Prodrug activation
(eg, thymidine kinase)
and ganciclovir
DNA decoy
(eg, androgen receptor)
Tumour suppressor
(eg, P53)
Proapoptotic gene
(eg, BAX)
Antiangiogenic gene
(eg, thrombospondin 1)
Cytokine
(eg, interleukin 2)
Tumour antigen
(eg, prostate-specific
antigen)
Cell-cycle block
Apoptosis
Tumour blood
supply inhibited
Immune system
induced to
attack tumour
Oligonucleotide
delivered to tumour
targets specific
cellular genes to
prevent protein
synthesis
Delivery of vector
encoding therapeutic
gene to tumour
causes transcription
and translation of
therapeutic protein
Figure 2. Strategies for prostate-cancer gene therapy. The ability to transfer genes or oligonucleo-
tides into prostate tumours, as well as an improved understanding of the molecular biology of
tumours, allows for the use of an increasingly wide range of mechanisms to counter tumour
growth.
3. 471
antigen),18
or by transfection of tumour cells with cytokines
(eg, interleukin 2 and granulocyte-macrophage colony-
stimulating factor).19,20
Shah and co-workers21
used a
therapeutic gene to improve indirectly the ability of the
immune system to respond to challenges such as prostate
cancer. Mice were treated with a gene that encoded a mutant
form of the receptor for transforming growth factor ,
which rendered bone-marrow cells insensitive to the
immunosuppressive effects of the growth factor and
inhibited metastasis of prostate-cancer xenografts.21
Gene expression
In vitro, several targeted approaches have been used for
prostate cancer, and less commonly in animals or phase I
clinical studies. The androgen receptor is crucial because it
stimulates proliferation of prostate-cancer cells by activating
transcription of target genes. This transcriptional activation
has been competitively inhibited by transfection of double-
stranded DNA decoy fragments that include the androgen-
receptor binding site.22
Androgen-receptor mRNA has also
been targeted by use of an antisense strategy,23
as have the
proto-oncogenes BCL224
and MYC.25
Antisense oligo-
nucleotides inhibit gene expression by binding to a specific
target mRNA that has a complementary nucleotide
sequence, resulting in degradation and inhibition of
translation of the target gene.
RNA can also be targeted by use of small interfering
RNA—short RNA duplexes that mediate sequence-specific
mRNA degradation and have a role in gene silencing in
eukaryotes.26
Small interfering RNAs targeted against EZH2
inhibited cell proliferation in prostate-cancer cell lines.27
EZH2, a homologue of a Drosophila melanogaster gene that
regulates gene transcription, was selected because micro-
array studies identified the gene as significantly upregulated
in metastatic prostate cancer compared with localised
prostate cancer.27
Triplex-forming oligonucleotides offer another mecha-
nism for sequence-specific silencing of genes, but they have
fewer potential target sequences than antisense strategies or
small interfering RNAs. Triplex-forming oligonucleotides
bind to double-stranded DNA to form a triple-helix structure
and inhibit transcription of genes such as the transcription
factor ETS2, which has been implicated in the development of
prostate cancer.28
All of the strategies discussed above require the ability to
identify genes that are upregulated in prostate cancer (or in
progression of prostate cancer) and use gene targeting to
interfere with, or specifically ablate, expression of target
genes.
Vectors for delivery of therapeutic genes
Crucial to any strategy that relies on the introduction of
foreign genetic material to cells is the ability to deliver genes to
the appropriate cell or tissue in sufficient numbers to achieve
a therapeutic effect. Viral vectors are designed to harness the
attributes of viruses as delivery agents; the design involves
removal of many virally encoded genes (generating so-called
gutless vectors) and introduction of the therapeutic gene.
Vectors derived from retroviruses, adenoviruses, vaccinia
virus, adeno-associated virus, and herpes simplex virus are
used extensively.29
Non-viral methods of gene delivery include
use of liposomes, cationic polymers, and disruption of the cell
membrane by physical methods (eg, electroporation and
ultrasonography).30
Although bacteria have not been inves-
tigated extensively as vehicles for gene delivery, Salmonella
typhimurium has been modified to express prodrug-activation
genes, with resultant antitumour effects.31,32
Viral vectors
The biological properties of the most widely used viral
vectors have been reviewed,29
and are summarised in table 1.
Retroviruses29
integrate into the cellular genome after reverse
transcription, allowing long-term stable gene expression.
Clearly, this integration is beneficial for gene replacement in
disorders such as severe combined immunodeficiency,33
but
it is less important in most strategies of gene therapy for
cancer, in which the intention is to kill the target cells.
Integration can also result in serious adverse events if
insertional mutagenesis activates a proto-oncogene. Adverse
events have been reported in a clinical trial on retroviral gene
therapy, in which two cases of uncontrolled proliferation of
T cells were described among ten patients receiving gene
therapy for severe combined immunodeficiency
(ie, replacement of IL2RG).33
These events have raised
serious concerns about ensuring the safety of gene therapy.
With the exception of lentiviruses, retroviruses can
transduce only dividing cells—an advantage for the targeting
of malignant, rather than benign, cells. Although care is
taken to ensure that retroviral vectors are replication
deficient, the possibility of recombination in vivo resulting
in a replication-competent vector is an additional safety
concern for lentiviral vectors derived from HIV.34
The
usefulness of retroviruses is also limited by their small
genome size (8–9 kb), and the difficulty in obtaining high
viral titres during production.34
Despite these obstacles,
protocols for research on use of retroviruses as vectors
account for many trials on gene therapy for cancer, and
retroviruses have been used in two clinical trials on prostate
cancer.20,35
ReviewGene therapy for prostate cancer
Oncology Vol 5 August 2004 http://oncology.thelancet.com
Prodrug activation gene vector
Inactive prodrug Active prodrug
Enzymes
Intratumoural
Intravenous
Figure 3. The strategy of prodrug activation aims to kill tumour cells by
combined treatment with a prodrug and a therapeutic gene. A prodrug is
administered intravenously, but requires a specific prodrug-activation
enzyme to convert it to an active cytotoxic derivative. The prodrug-
activation enzyme is produced in the tumour after intratumoural injection
of a prodrug-activation gene.
4. 472
Adenovirus vectors29
have also been investigated
extensively; adenovirus type 5 is the most commonly used
vector in clinical trials on gene therapy for prostate cancer.
These parvoviruses are maintained transiently because
they do not integrate into the genome and therefore pose
no risk of insertional mutagenesis. Furthermore,
adenoviruses transduce both dividing and non-dividing
cells efficiently,29
and high titres can readily be prepared,4,9
thus offering several advantages over retroviruses.
Adenovirus vectors can accommodate inserts of up to
30 kb, but their most important drawback is undoubtedly
their immunogenicity.
Immune resistance to adenoviruses has caused
substantial problems for repeated injections of the vector.29
Because transgene expression is transient after a single
injection,7,11
adenovirus vectors are limited to applications in
which short-term gene expression is sufficient. Toxic effects
in patients because of inflammatory responses to adenovirus
are also an issue. Indeed, the only death of a patient
undergoing gene therapy occurred after an immune reaction
when an adenovirus vector was used to administer the
ornithine carbamoyltransferase gene (OTC) to a patient with
a deficiency in this enzyme36
(although the trial protocol had
not been followed).37
Adenovirus vectors have been modified
extensively to decrease their immunogenicity by deletion of
the E1 gene and other genes, including E2 and E3.4,10
Potentially, all adenovirus genes can be deleted from the
vector genome and expressed during production of vectors
by helper viruses, plasmids, or cellular genes.38
Both
replication-deficient adenoviruses4,7,8,10,39
and attenuated
replication-competent9,11,16
adenoviruses have been used in
gene therapy for prostate cancer.
Vaccinia virus and other poxviruses have emerged as
promising vectors for gene therapy. Unusually for DNA
viruses, poxviruses replicate in the cytoplasm of the host cell
rather than the nucleus and can carry substantially larger
inserts (over 30 kb) than retroviruses.29
Vectors derived from
vaccinia virus elicit a rapid and sustained humoral immune
response.40
However, this response has not been associated
with negative side-effects as much as that to adenoviruses,
possibly because of modulation by genes encoded by
vaccinia virus.7,10,41,42
Indeed, this property of fewer side-
effects has been harnessed to deliver antigens as vaccines.
Vaccinia viruses have been used in gene therapy for prostate
cancer to deliver a vaccine of prostate-specific antigen
(PSA).18,41,42
Adeno-associated viruses integrate in a non-
homologous way into chromosomal DNA and can be
maintained there over long periods.43
The ability of the
virus to integrate is beneficial (especially for diseases that
require sustained treatment), but integration also poses
risks, as for retroviruses. Although no adverse events
related to integration of adeno-associated virus have been
reported in clinical trials on gene therapy, it is nevertheless
a potential concern. Adeno-associated viruses possibly
have the best safety profile among the viruses used widely
to date because they have low immunogenicity, few toxic
effects, and no known association with any human
disease.29
However, these advantages are offset by the upper
limit of 4·5 kb on transgene size,29
which prevents the
insertion of long regulatory sequences, multiple genes, or
even a single large gene into vectors based on adeno-
associated virus.
Because of the natural tropism of herpes simplex virus
for nerve cells, vectors based on herpes simplex virus type I
have been used mainly to deliver genes to the CNS.44,45
Herpes simple virus type 1 virions are maintained in
neurons as latent episomes, and stable expression for
2 months has been obtained under the control of wildtype
promoters and modified latency-associated promoters.44
Herpes simplex virus vectors have been modified by deletion
of viral genes such ICP27, ICP4, and ICP34.5, in efforts to
reduce their toxic effects.45
Although the large genome size of
this virus makes deletion a more complex task than in
adenoviruses, the process also offers the useful possibility of
inserting transgenes up to 30 kb in length.29
Non-viral vectors
Liposomes are cationic lipids, or more usually a
combination of cationic and neutral lipids, which have been
used for the cellular delivery of drugs46
and to deliver
plasmids carrying therapeutic genes. The positive charge of
liposomes facilitates the formation of complexes with DNA,
and their lipid structure allows them to cross cell
membranes. Generally, liposomes have been less efficient
than viral vectors, although improved formulations47
and
formation of complexes with targeting molecules48
have been
developed to improve uptake and decrease the problem of
the sequestration of vectors in endosomes.49
Similarly, cationic polymers bind to nucleic acids to
facilitate intracellular delivery. In vitro, the dendrimer
polyethyleneimine has been used for transfection of
prostate-cancer cells.50
Plasmids have also been delivered by
use of electroporation, in which cell membranes are made
permeable temporarily by exposure to a strong electrostatic
field. Although used mainly in cell-culture systems,
electroporation has also been used to deliver transgenes to
subcutaneous prostate tumours in mice.51
Liposomes, cationic polymers, and similar complexes—
eg, poly(D,L-lactide-co-glycolide) and poly(lactic acid)—are
Review Gene therapy for prostate cancer
Oncology Vol 5 August 2004 http://oncology.thelancet.com
Table 1. Properties of viral vectors for gene therapy
Vector type Nucleic acid Insert size (kb) Integrates into chromosome? Infects quiescent cells?
Retrovirus Double-stranded RNA 8·0 Yes No (except lentiviruses)
Adenovirus Double-stranded DNA 30·0 No Yes
Poxvirus Double-stranded DNA 30·0 or greater No Yes
Adeno-associated virus Double-stranded DNA 4·5 Yes Yes
Herpes simplex virus Single-stranded DNA 30·0 No Yes
5. 473
easy to prepare, cause few toxic effects, and elicit less
immunogenicity than most viral vectors.30
Indeed, in some
circumstances, DNA can be delivered successfully without
any carrier molecule. For example, a plasmid that encoded a
PSA vaccine elicited a strong immune response in mice
when injected into muscle.52
Methods of chemical delivery
are also suitable for very large DNA molecules. Mammalian
artificial chromosomes have been delivered by use of
liposomes and maintained in 70% of cells in vitro for
2 months without the application of selection.53
Thus, non-viral methods of gene delivery, although
generally less efficient than techniques that use viruses,
might prove very useful if barriers to their efficacy are
overcome. Further research on the stability in vivo of vectors
not based on viruses, the targeting of specific cell types, entry
of vectors into cells, subsequent delivery of DNA to cell
nuclei, and avoidance of vector degradation in endosomes,
might lead to artificial vectors that have similar efficiency
but a better safety profile than vectors based on viruses.
Liposomes have already been used frequently to deliver
therapeutic genes in preclinical studies on prostate cancer54
and in several clinical trials, including one trial on prostate
cancer.19
Routes of vector administration
The anatomical route by which a vector is delivered is clearly
an important consideration for safety and efficacy. Vectors
for gene therapy in clinical trials have been delivered by
intratumoural, subcutaneous, intravenous, intramuscular,
or intradermal injection, as well as other methods such as
bone-marrow transplantation and aerosol application to the
airway. Several techniques are suitable strategies for specific
diseases, such as intratumoural injection for cancers,
intranasal delivery for cystic fibrosis, and bone-marrow
transplantation for severe combined immunodeficiency or
other disorders of haemopoietic cells. Vectors can be
delivered to the skin, vasculature, or muscle for a wide range
of applications.
Selection of an appropriate method of vector
administration depends on both the disease in question and
the therapeutic gene to be used. For example, a vector
designed to cause apoptosis should be restricted to the disease
site as much as possible, even if this involves a more invasive
method of delivery. Most clinical trials on gene therapy for
patients with prostate cancer have therefore administered
vectors into the tumour.8,9,16
Injection of vectors into prostate
tumours has been facilitated by the routine use of similar
techniques during brachytherapy. In a clinical trial10
of
prostate cancer, an adenovirus vector has been injected
directly into metastatic lesions of bone and lymph nodes.
If a vector encodes an antigen for the purpose of
immunisation (eg, PSA), specific delivery to the disease site
is not needed, and the intradermal, subcutaneous, and
intramuscular routes can be used.18,41,42,52
In a dose-escalation
clinical trial42
on PSA vaccination, lower doses of vector were
given intradermally and higher doses were given
subcutaneously because subcutaneous administration
delivers greater volumes of vector. These approaches, as well
as that of intraprostatic injection, restrict gene delivery to the
area immediately surrounding the injection site; however, a
small amount of vector might be absorbed into the systemic
circulation and delivered to other organs, especially the liver.
High concentrations of adenovirus vectors have been
reported in the liver after intravenous injection in mice.55
Intravenous administration is also limited by the presence of
serum proteins that inhibit non-virus transfection reagents,49
and this method also might not be suitable for transgenes
that, when expressed, can cause systemic toxic effects. In a
phase I clinical trial24
of prostate cancer, intravenous admin-
istration was used to deliver antisense oligonucleotides
against BCL2. Grade 4 toxic effects occurred, but could have
been due to the use of docetaxel in the study.24
The risk of inadvertent transduction of non-target cells
can be eliminated completely by gene delivery ex vivo. The
cells are obtained from a patient, cultured and transduced in
vitro, and returned to the patient. However, technical
difficulties (especially the culture conditions) have hindered
the use of gene delivery ex vivo.20
Tissue-specific gene expression
Several approaches have aimed to achieve tissue-specific
expression of the therapeutic gene. In prostate cancer,
transduction ex vivo20
and intraprostatic injection4,7–9,16
have
been used for this purpose. However, transduction outside the
body is not always suitable practically, and intraprostatic
injection in animal studies causes some vector dissemination
to other tissues.56
Alternatively, tissue specificity could be
achieved during the process of expression of the therapeutic
gene.
In addition to sequences that code for proteins, eukaryotic
genes include complex regulatory sequences that modify gene
transcription and translation. These regulatory sequences
include promoters located adjacent to transcription start sites.
As well as the basic function of allowing transcription to begin
at appropriate sites, promoters can include sequences that
restrict transcription to specific cell types by making
transcription dependent on the presence of different factors,
or by regulation of transcription through other methods.
Tissue-specific gene promoters, although rarely
completely specific, can be a very useful way of restricting
effective gene expression to the target tissue. Much research
has focused on the development of tissue-specific gene
promoters for use in prostate-cancer gene therapy, including
the challenge of achieving high promoter activity without
losing tissue specificity. The ability of a promoter to
distinguish the target tissue from liver and bladder is especially
important: high concentrations of vectors have been noted in
the liver after intravenous delivery,55
and in the bladder after
intraprostatic injection,56
in studies in mice and dogs.
Several promoters have been used, or have potential use,
in gene therapy for prostate cancer, including therapy for
metastatic and androgen-independent disease (table 2).
Most promoters have been selected because they have
preferential activity in prostate tissue; some promoters also
distinguish between benign and malignant prostate tissue.
An OTC gene promoter has also been developed to target
both the epithelium of the prostate tumour and stromal cells
in bone.68
ReviewGene therapy for prostate cancer
Oncology Vol 5 August 2004 http://oncology.thelancet.com
6. 474
Promoters such as the promoter of the human PSA gene
(KLK3) have a role in improving the efficacy and safety of
vectors that express anticancer genes (figure 4). Commonly,
promoters have been modified to increase their expression
while maintaining tissue specificity. Activity of the KLK3
promoter has been improved by deletion of unnecessary
sequences and by the engineering of multiple copies of
functional regions.55
The KLK3 promoter contains 15-bp
regions called androgen response elements, which bind the
androgen receptor and are important for the activation of
gene transcription. We have generated recombinant KLK3
promoters with sequence variations in androgen response
element I at sites likely to improve
activity to mimic two mutations in
breast tumours that overexpressed
PSA (figure 4), and are undertaking
tests in human prostate-cancer cell
lines.69,70
A hybrid promoter has been
generated from regions of the KLK3
promoter and the promoter of the
prostate-specific membrane antigen
gene FOLH1; the hybrid seems to
maintain the tissue specificity of the
PSA sequences while being less
androgen dependent.71
Modification
of the KLK3 promoter to become less
androgen dependent might make the
promoter more efficient in some
patients with low androgen
concentrations as a result of hormone-
withdrawal therapy.
Yoshimura and colleagues5
overcame the androgen dependence of
the KLK3 promoter by use of the Cre
recombinase system (figure 5). The
researchers introduced two thera-
peutic genes into a mouse with
prostate cancer, including a gene
derived from bacteria that codes for
the enzyme Cre recombinase, under
the control of the KLK3 promoter. In
the absence of androgen, there was
prostate-specific, but low, expression
of the enzyme. The Cre recombinase
enzyme bound specifically to two loxP
target sites in a second gene, resulting in a recombination
event and subsequent deletion of a negative regulatory
element between the two sites. After this modification by Cre
recombinase, the second gene caused high expression of the
therapeutic gene cytosine deaminase under the control of a
highly efficient (but not tissue-specific) cytomegalovirus
promoter. Because one Cre recombinase molecule can cause
recombination in many vectors, the system was designed to
increase the low expression of tissue-specific transgenes.5
The Cre recombinase system was active even in the absence
of androgen, as was the KLK3 promoter alone after
stimulation by androgens.5
Review Gene therapy for prostate cancer
Oncology Vol 5 August 2004 http://oncology.thelancet.com
Gene expressed
Cell death
Gene expressed
Cell death
Neighbouring
non-prostate
tissues
A
B C D
Prostate
tissue
PSA promoter Proapoptic gene
Vector
Figure 4. Development of prostate-specific gene promoters. For vectors expressing proapoptotic
genes, tissue-specific promoters offer greater safety and specificity to that provided by intratumoral
injection (A). Sequence of the PSA promoter (KLK3) before (B), and after (C, D), mutagenesis.
Table 2. Gene promoters with potential use in prostate-cancer gene therapy
Gene Expression profile Effectiveness in mice Refs
Rat probasin gene Generally restricted to prostate tissue in transgenic mice, but detected at Tumour regression 14, 57
low amounts in testes
BCL2 Overexpressed in androgen-independent prostate tumours Decreased tumour volume 15, 58
Kallikrein 3 (KLK3, prostate Used as clinical disease marker Tumour regression 59–63
-specific antigen)* Low or absent expression in most non-prostate tissues
Higher expression in benign tissue than malignant tissue
Folate hydrolase (FOLH1, Higher expression in malignant tissue than benign tissue Decreased tumour volume 64–67
prostate-specific membrane Upregulated expression in the absence of androgens
antigen) Variable tissue specificity in vitro Tumour regression 68
Mouse osteocalcin gene* Expressed in osteoblasts, calcified smooth muscle, and prostate tumours
*The human kallikrein 3 promoter and mouse osteocalcin promoter have been used in clinical trials.
7. 475
The search for prostate cancer-specific expression of
transgenes has also led to several other strategies. Peng and
co-workers15
have exploited the overexpression of the
proto-oncogene BCL2 in prostate cancer by use of BCL2
promoter sequences to direct expression of the gene for
diphtheria toxin A in a study in mice with prostate cancer
(table 2). This transgene was engineered further so that
expression depended on the presence of tamoxifen (figure
6).15
Two genes, a fusion gene and a therapeutic gene, were
delivered to prostate tumours in vivo. The fusion gene was
regulated by a BCL2 promoter and encoded two proteins—
a bacterial recombinase enzyme and an oestrogen receptor
modified to bind tamoxifen—that were joined, but with
each retaining its own function. After the binding of
tamoxifen to the oestrogen receptor, the conformation of
the fusion protein changed so that the recombinase was
active. The activated recombinase then deleted an
inhibitory sequence from the therapeutic-gene construct,
resulting in expression of the therapeutic gene under the
control of a non-specific but efficient promoter. Therefore,
expression of the therapeutic gene occurred only in cells
that expressed BCL2 (in other cells, the BCL2 promoter was
not active) and in the presence of tamoxifen (in other cells,
the recombinase was not active and the inhibitory sequence
remained in the therapeutic gene).15
Several approaches that used tissue-specific promoters
have shown effectiveness against prostate cancer in vivo, and
the OTC10
and KLK316
promoters have both been used in
phase I clinical trials on prostate cancer.
Clinical trials and promising
preclinical studies
Suicide-gene therapy
Gene therapy for prostate cancer based
on prodrug activation, most commonly
by use of the thymidine kinase system,
has been investigated in several clinical
trials. In a phase I trial,4
treatment of
recurring non-metastatic disease with
thymidine kinase and subsequent prodrug
administration caused sustained decreases
in serum concentration of PSA that
ranged from 6 weeks to longer than 1 year
in three of 18 patients (although one
patient developed grade 4 thrombo-
cytopenia at the highest dose of prodrug).
In a phase I/II trial,8
gene therapy with
thymidine kinase in an adenovirus vector
was given in combination with radio-
therapy. In another phase I/II trial7
of
thymidine kinase therapy, 78% of patients
with local recurrence of prostate cancer
after radiotherapy achieved partial
decreases in PSA. Most interestingly, a
similar cohort of patients were treated in a
phase I trial9
with a replication-competent
adenovirus that included a fusion gene for
a cytosine deaminase and thymidine
kinase. No dose-limiting toxic effects were
seen, and two of 18 patients showed no
evidence of having prostate cancer 1 year after treatment.9
A phase I clinical trial10
of 11 patients with metastatic or locally
recurrent prostate cancer assessed the thymidine kinase gene
combined with the prodrug valaciclovir. An adenovirus
vector, which carried the thymidine kinase gene controlled by
an OTC promoter, was injected into individual lesions and led
to temporary stabilisation of disease in one patient, and grade
1–3 toxic effects.10
Use of cytosine deaminase combined with
the prodrug flucytosine has also shown effectiveness against
prostate cancer in mice.5
By use of mouse xenografts, Freytag and colleagues72
have
assessed trimodal therapy for prostate cancer, consisting of a
replication-competent adenovirus vector, a cytosine-
deaminase thymidine-kinase fusion gene and prodrugs
activated by both enzymes encoded by the fusion gene, and
radiation. The researchers found that trimodal therapy
improved the cure rate and decreased the frequency of
metastases. However, they also noted that use of virus
combined with external-beam radiotherapy caused synergistic
toxic effects. In a phase I clinical trial11
of 15 patients with
newly diagnosed non-metastatic prostate cancer, use of
trimodal therapy did not lead to any dose-limiting toxic
effects, although four cases of grade 3 adverse events were
reported that might have been a result of treatment. There was
no evidence of circulating infectious adenovirus, and toxic
effects in the liver were limited to grade 1 or 2, suggesting that
trimodal therapy is safe in patients.11
Patients in this trial who
received longer courses of prodrug therapy showed a more
rapid decline in serum concentrations of PSA.11
ReviewGene therapy for prostate cancer
Oncology Vol 5 August 2004 http://oncology.thelancet.com
Non-specific
promoter
Recombinase
target site
PSA
promoter
Recombinase
gene
Non-specific
promoter
Therapeutic
gene
Inhibitory
sequence
Recombinase
target site
Therapeutic
gene
A
Non-specific
promoter
Recombinase
target site
Inhibitory
sequence
Recombinase
target site
Therapeutic
gene
B
C
Not expressed
Therapeutic
protein
Figure 5. The Cre recombinase system amplifies low expression from a prostate-restricted
promoter.15
Two transgenes were delivered into mouse prostate tumours (A). Recombinase
enzyme was expressed in prostate cells, and deleted an inhibitory sequence in the second
transgene to activate the gene (B). A therapeutic gene was then highly expressed, indirectly
regulated by the PSA promoter KLK3 (C).
8. 476
Immunotherapy
Immunotherapy has also been investigated in the
treatment of prostate cancer. In a phase I trial,19
six of
24 patients with locally advanced or recurrent prostate
cancer had a mean decrease in serum concentration of PSA
of 39% 10 weeks after treatment with a plasmid that
expressed interleukin 2 delivered by use of liposomes. The
researchers reported an increase in the infiltration of
lymphocytes into tumours, and no toxic effects higher than
grade 2 were seen.19
An adenovirus vector that expressed
interleukin 2 was administered by intraprostatic injection
to 12 patients with prostate cancer who had clinically
localised high-risk disease.39
In this phase I trial, treatment
increased the presence of cytokines at the vaccine site.
Grade 2 or lower toxic effects were seen (apart from in one
patient, who had grade 3 lymphopenia). Transduction of
prostate-cancer cells with granulocyte-monocyte colony-
stimulating factor ex vivo followed by intradermal
injection of the transduced cells caused T-cell and B-cell
immune responses against prostate-cancer cells in a phase I
clinical trial.20
A PSA vaccine delivered by a
modified vaccinia virus has shown low
toxic effects and variable efficacy in three
phase I trials of prostate cancer,18,41,42
after
studies in animals showed that a similar
strategy elicited a strong and sustained
immune response.52
In one of six patients
with recurrent prostate cancer treated by
PSA vaccination, disease progression was
delayed for longer than 8 months after
interruption of hormonal therapy.18
A
trial41
of PSA vaccination in 33 patients
with advanced prostate cancer showed
that vaccination stabilised disease for
11–25 months in nine patients. A PSA-
specific T-cell response was seen in five
of seven patients tested, all of whom also
received granulocyte-monocyte colony-
stimulating factor.41
A clinical trial42
of
PSA vaccination involving 42 patients
with metastatic androgen-independent
prostate cancer showed a PSA-specific
immune response in four of six patients
tested. In studies on mice with prostate
cancer, a gene that encoded a modified
transforming growth factor  receptor
improved survival by overcoming sup-
pression of the immune function of bone
marrow.21
Manipulation of the cell cycle and
apoptosis
The tumour-suppressor gene BRCA1 has
been administered to patients with
advanced prostate cancer in a phase I
clinical trial35
by intraprostatic injection of
retrovirus without substantial toxic effects.
The therapeutic potential of other
tumour-suppressor genes has also been investigated.
Restoration of P53 decreased the growth and tumorigenicity
of androgen-independent human prostate-cancer cells in
vivo.73
However, this restoration did not affect a P53-null
mouse prostate-cancer cell line, which was inhibited in vivo
by transfection of the P21 gene (another cell-cycle regulator).74
A prostate-specific attenuated replication-competent
adenovirus has led to a dose-dependent decrease in serum
concentration of PSA in a phase I trial.16
Tumour regression
has been seen in mice with prostate tumours xenografted onto
the skeleton after treatment with an attenuated replication-
Review Gene therapy for prostate cancer
Oncology Vol 5 August 2004 http://oncology.thelancet.com
Search strategy and selection criteria
Data for this review were identified from PubMed and
references of relevant articles. Searches used combinations of
the search terms “prostate cancer”, “gene therapy”, “gene”,
“therapy”, “treatment”, “delivery”, “vector”, “tissue-specific”,
“prostate-specific”, and “promoter”. Abstracts of important
developments for which no full-text articles were available, and
of results from our own laboratory, were included. Only papers
published in English between 1990 and 2004 were included.
BCL2
promoter
Non-specific
promoter
Therapeutic
gene
Recombinase Modified
ER
A
B
Non-specific
promoter
Recombinase
target site
Inhibitory
sequence
Therapeutic
gene
C
D
Fusion protein
Fusion gene
Recombinase
activated
Therapeutic
protein
Fusion protein
Tamoxifen
Recombinase
target site
Figure 6. BCL2-dependent and tamoxifen-dependent expression of transgenes delivered
together into mouse prostate tumours. Expression of a recombinase-oestrogen receptor (ER)
fusion gene (A). Activation of recombinase by the binding of ER to tamoxifen (B). Recombinase
deletes an inhibitory sequence from a therapeutic gene (C). Expression of therapeutic gene
under indirect control of the BCL2 promoter (D).
9. 477
competent adenovirus controlled by an OTC promoter that
targeted the tumour and bone stroma.68
Survival of mice
xenografted with LNCaP human prostate-cancer cell lines has
been lengthened by treatment with a prostate-specific,
inducible caspase 9 gene.14
The genes for diphtheria toxin A15
and FAS ligand75
have caused inhibition of tumour growth in
mice with prostate-cancer xenografts; these genes merit
further study as therapeutic agents.
Antisense approaches
A phase I/II clinical trial is under way to ascertain the
combined efficacy and safety of BCL2 antisense
oligonucleotide and docetaxel in progressive metastatic
prostate cancer. Four of 12 patients showed decreases in
serum concentration of PSA, although one patient had dose-
limiting grade 4 toxic effects.24
In studies in mice, antisense
oligonucleotides to MYC caused regression of prostate
tumours;25
antisense targeted to the androgen receptor has
also inhibited tumour growth.23
Conclusion
Several gene-based approaches have been devised to treat
prostate cancer, either by direct control of cancer-cell
proliferation, by activation of an immune response against the
tumour, or by inhibition of angiogenesis. Adenoviruses,
retroviruses, and liposomes are the vectors used most
commonly to deliver genes to prostate-cancer cells. Prostate-
specific gene promoters have been developed to improve the
safety profile of therapeutic vectors. To date, at least 15 phase I
or phase I/II clinical trials on gene therapy for prostate cancer
have been started; in several trials, decreases in concentration
of serum PSA have been achieved. In one trial,9
two patients
with local recurrence of prostate cancer after radiotherapy
remained in clinical remission 1 year after receiving gene
therapy based on prodrug activation. In another trial,41
25% of
patients with advanced prostate cancer given a PSA vaccine
showed stable disease for 11–25 months. Other approaches
have led to tumour regression or lengthened survival in
studies in animals. With increasing knowledge of the
molecular pathology of prostate cancer, new therapeutic
targets might also emerge in the near future.
Conflict of interest
None declared.
Acknowledgments
We received funding from the Health Research Board, Ireland, and St
Luke’s Institute for Cancer Research, Ireland.
References
1 Parkin DM, Bray FI, Devesa SS. Cancer burden in the year 2000.
The global picture. Eur J Cancer 2001; 37 (suppl): S4–66.
2 Rhodes DR, Barrette TR, Rubin MA, et al. Meta-analysis of
microarrays: interstudy validation of gene expression profiles
ReviewGene therapy for prostate cancer
Oncology Vol 5 August 2004 http://oncology.thelancet.com
reveals pathway dysregulation in prostate cancer. Cancer Res 2002;
62: 4427–33.
3 Dhanasekaran SM, Barrette TR, Ghosh D, et al. Delineation of
prognostic biomarkers in prostate cancer. Nature 2001; 412:
822–26.
4 Herman JR, Adler HL, Aguilar-Cordova E, et al. In situ gene
therapy for adenocarcinoma of the prostate: a phase I clinical trial.
Hum Gene Ther 1999; 10: 1239–49.
5 Yoshimura I, Ikegami S, Suzuki S, et al. Adenovirus mediated
prostate specific enzyme prodrug gene therapy using prostate
specific antigen promoter enhanced by the Cre-loxP system.
J Urol 2002; 168: 2659–64.
6 Huber BE, Austin EA, Good SS, et al. In vivo antitumor activity of
5-fluorocytosine on human colorectal carcinoma cells genetically
modified to express cytosine deaminase. Cancer Res 1993; 53:
4619–26.
7 Miles BJ, Shalev M, Aguilar-Cordova E, et al. Prostate-specific
antigen response and systemic T cell activation after in situ gene
therapy in prostate cancer patients failing radiotherapy.
Hum Gene Ther 2001; 12: 1955–67.
8 Teh BS, Aguilar-Cordova E, Kernen K, et al. Phase I/II trial
evaluating combined radiotherapy and in situ gene therapy with or
without hormonal therapy in the treatment of prostate cancer—a
preliminary report. Int J Radiat Oncol Biol Phys 2001; 51: 605–13.
9 Freytag SO, Khil M, Stricker H, et al. Phase I study of replication-
competent adenovirus-mediated double suicide gene therapy for
the treatment of locally recurrent prostate cancer. Cancer Res 2002;
62: 4968–76.
10 Kubo H, Gardner TA, Wada Y, et al. Phase I dose escalation clinical
trial of adenovirus vector carrying osteocalcin promoter-driven
herpes simplex virus thymidine kinase in localized and metastatic
hormone-refractory prostate cancer. Hum Gene Ther 2003; 14:
227–41.
11 Freytag SO, Stricker H, Pegg J, et al. Phase I study of replication-
competent adenovirus-mediated double-suicide gene therapy in
combination with conventional-dose three-dimensional conformal
radiation therapy for the treatment of newly diagnosed, inter-
mediate to high-risk prostate cancer. Cancer Res 2003; 63: 7497–506.
12 Asgari K, Sesterhenn IA, McLeod DG, et al. Inhibition of the growth
of pre-established subcutaneous tumor nodules of human prostate
cancer cells by single injection of the recombinant adenovirus p53
expression vector. Int J Cancer 1997; 71: 377–82.
13 Li X, Marani M, Yu J, et al. Adenovirus-mediated Bax over-
expression for the induction of therapeutic apoptosis in prostate
cancer. Cancer Res 2001; 61: 186–91.
14 Xie X, Zhao X, Liu Y, et al. Adenovirus-mediated tissue-targeted
expression of a caspase-9-based artificial death switch for the
treatment of prostate cancer. Cancer Res 2001; 61: 6795–804.
15 Peng W, Verbitsky A, Bao Y, Sawicki J. Regulated expression of
diphtheria toxin in prostate cancer cells. Mol Ther 2002; 6: 537–45.
16 DeWeese TL, van der Poel H, Li S, et al. A phase I trial of CV706, a
replication-competent, PSA selective oncolytic adenovirus, for the
treatment of locally recurrent prostate cancer following radiation
therapy. Cancer Res 2001; 61: 7464–72.
17 Jin RJ, Kwak C, Lee SG, et al. The application of an anti-angiogenic
gene (thrombospondin-1) in the treatment of human prostate
cancer xenografts. Cancer Gene Ther 2000; 7: 1537–42.
18 Sanda MG, Smith DC, Charles LG, et al. Recombinant vaccinia-PSA
(PROSTVAC) can induce a prostate-specific immune response in
androgen-modulated human prostate cancer. Urology 1999; 53:
260–66.
19 Belldegrun A, Tso CL, Zisman A, et al. Interleukin 2 gene therapy
for prostate cancer: phase I clinical trial and basic biology.
Hum Gene Ther 2001; 12: 883–92.
20 Simons JW, Mikhak B, Chang JF, et al. Induction of immunity to
prostate cancer antigens: results of a clinical trial of vaccination with
irradiated autologous prostate tumor cells engineered to secrete
granulocyte-macrophage colony-stimulating factor using ex vivo
gene transfer. Cancer Res 1999; 59: 5160–68.
21 Shah AH, Tabayoyong WB, Kundu SD, et al. Suppression of tumor
metastasis by blockade of transforming growth factor beta signalling
in bone marrow cells through a retroviral-mediated gene therapy in
mice. Cancer Res 2002; 62: 7135–38.
22 Kuratsukuri K, Sugimura K, Harimoto K, et al. “Decoy” of
androgen-responsive element induces apoptosis in LNCaP cells.
Prostate 1999; 41: 121–26.
Useful websites
http://www.mdanderson.org/diseases/prostate/
http://www.nlm.nih.gov/medlineplus/prostatecancer.html
http://www.wiley.co.uk/genetherapy/clinical/
http://www4.od.nih.gov/oba/rdna.htm
10. 478
23 Eder IE, Hoffmann J, Rogatsch H, et al. Inhibition of LNCaP
prostate tumor growth in vivo by an antisense oligonucleotide
directed against the human androgen receptor. Cancer Gene Ther
2002; 9: 117–25.
24 Tolcher AW. Preliminary phase I results of G3139 (bcl-2 antisense
oligonucleotide) therapy in combination with docetaxel in
hormone-refractory prostate cancer. Semin Oncol 2001; 28 (suppl):
67–70.
25 Steiner MS, Anthony CT, Lu Y, Holt JT. Antisense c-myc retroviral
vector suppresses established human prostate cancer. Hum Gene
Ther 1998; 9: 747–55.
26 Shi Y. Mammalian RNAi for the masses. Trends Genet 2003; 19: 9–12.
27 Varambally S, Dhanasekaran SM, Zhou M, et al. The polycomb
group protein EZH2 is involved in progression of prostate cancer.
Nature 2002; 419: 624–29.
28 Carbone GM, McGuffie EM, Collier A, Catapano CV. Selective
inhibition of transcription of the Ets2 gene in prostate cancer cells by
a triplex-forming oligonucleotide. Nucleic Acids Res 2003; 31: 833–43.
29 Bonnet MC, Tartaglia J, Verdier F, et al. Recombinant viruses as a
tool for therapeutic vaccination against human cancers. Immunol
Lett 2000; 74: 11–25.
30 Nishikawa M, Hashida M. Nonviral approaches satisfying various
requirements for effective in vivo gene therapy. Biol Pharm Bull
2002; 25: 275–83.
31 Pawelek JM, Low KB, Bermudes D. Tumor-targeted Salmonella as a
novel anticancer vector. Cancer Res 1997; 57: 4537–44.
32 Cunningham C, Nemunaitis J. A phase I trial of genetically modified
Salmonella typhimurium expressing cytosine deaminase (TAPET-
CD, VNP20029) administered by intratumoral injection in
combination with 5-fluorocytosine for patients with advanced or
metastatic cancer. Hum Gene Ther 2001; 12: 1594–96 (abstr).
33 Hacein-Bey-Abina S, Von Kalle C, Schmidt M, et al. LMO2-
associated clonal T cell proliferation in two patients after gene
therapy for SCID-X1. Science 2003; 302: 415–19.
34 Zheng JY, Chen D, Chan J, et al. Regression of prostate cancer
xenografts by a lentiviral vector specifically expressing diphtheria
toxin A. Cancer Gene Ther 2003; 10: 764–70.
35 Steiner MS, Lerner J, Greenberg, M et al. Clinical phase I gene
therapy trial using BRCA1 retrovirus is safe. J Urol 1998; 159:
132 (abstr).
36 Barbour V. The balance of risk and benefit in gene-therapy trials.
Lancet 2000; 355: 384.
37 The Lancet. Gene therapy under cloud. Lancet 2000; 355: 329.
38 Chen HH, Mack LM, Kelly R, et al. Persistence in muscle of an
adenoviral vector that lacks all viral genes. Proc Natl Acad Sci USA
1997; 94: 1645–50.
39 Trudel S, Trachtenberg J, Toi A, et al. A phase I trial of adenovector-
mediated delivery of interleukin-2 (AdIL-2) in high-risk localized
prostate cancer. Cancer Gene Ther 2003; 10: 755–63.
40 Gnant MF, Noll LA, Irvine KR, et al. Tumor-specific gene delivery
using recombinant vaccinia virus in a rabbit model of liver
metastases. J Natl Cancer Inst 1999; 91: 1744–50.
41 Eder JP, Kantoff PW, Roper K, et al. A phase I trial of a recombinant
vaccinia virus expressing prostate-specific antigen in advanced
prostate cancer. Clin Cancer Res 2000; 6: 1632–38.
42 Gulley J, Chen AP, Dahut W, et al. Phase I study of a vaccine using
recombinant vaccinia virus expressing PSA (rV-PSA) in patients
with metastatic androgen-independent prostate cancer. Prostate
2002; 53: 109–17.
43 Nakai H, Iwaki Y, Kay MA, Couto LB. Isolation of recombinant
adeno-associated virus vector-cellular DNA junctions from mouse
liver. J Virol 1999; 73: 5438–47.
44 Palmer JA, Branston RH, Lilley CE, et al. Development and opti-
mization of herpes simplex virus vectors for multiple long-term gene
delivery to the peripheral nervous system. J Virol 2000; 74: 5604–18.
45 Lilley CE, Groutsi F, Han Z, et al. Multiple immediate-early gene-
deficient herpes simplex virus vectors allowing efficient gene
delivery to neurons in culture and widespread gene delivery to the
central nervous system in vivo. J Virol 2001; 75: 4343–56.
46 Ishida T, Kirchmeier MJ, Moase EH, et al. Targeted delivery and
triggered release of liposomal doxorubicin enhances cytotoxicity
against human B lymphoma cells. Biochim Biophys Acta 2001;
1515: 144–58.
47 Shi F, Nomden A, Oberle V, et al. Efficient cationic lipid-mediated
delivery of antisense oligonucleotides into eukaryotic cells: down-
regulation of the corticotropin-releasing factor receptor.
Nucleic Acids Res 2001; 29: 2079–87.
48 Otomo T, Yamamoto S, Morishita R, Kaneda Y. EBV replicon
vector system enhances transgene expression in vivo: applications to
cancer gene therapy. J Gene Med 2001; 3: 345–52.
49 Meyer O, Kirpotin D, Hong K, et al. Cationic liposomes coated with
polyethylene glycol as carriers for oligonucleotides. J Biol Chem
1998; 273: 15621–27.
50 Frønsdal K, Engedal N, Slagsvold T, Saatcioglu F. CREB binding
protein is a coactivator for the androgen receptor and mediates
cross-talk with AP-1. J Biol Chem 1998; 273: 31853–59.
51 Mikata K, Uemura H, Ohuchi H, et al. Inhibition of growth of
human prostate cancer xenograft by transfection of p53 gene: gene
transfer by electroporation. Mol Cancer Ther 2002; 1: 247–52.
52 Kim JJ, Trivedi NN, Wilson DM, et al. Molecular and immuno-
logical analysis of genetic prostate specific antigen (PSA) vaccine.
Oncogene 1998; 17: 3125–35.
53 Mejía JE, Willmott A, Levy E, et al. Functional complementation
of a genetic deficiency with human artificial chromosomes.
Am J Hum Genet 2001; 69: 315–26.
54 Iyer M, Wu L, Carey M, et al. Two-step transcriptional amp-
lification as a method for imaging reporter gene expression using
weak promoters. Proc Natl Acad Sci USA 2001; 98: 14595–600.
55 Wu L, Matherly J, Smallwood A, et al. Chimeric PSA enhancers
exhibit augmented activity in prostate cancer gene therapy vectors.
Gene Ther 2001; 8: 1416–26.
56 Steiner MS, Zhang Y, Carraher J, Lu Y. In vivo expression of
prostate-specific adenoviral vectors in a canine model. Cancer Gene
Ther 1999; 6: 456–64.
57 Wu X, Wu J, Huang J, et al. Generation of a prostate epithelial cell-
specific Cre transgenic mouse model for tissue-specific gene
ablation. Mech Dev 2001; 101: 61–69.
58 McDonnell TJ, Troncoso P, Brisbay SM, et al. Expression of the
protooncogene bcl-2 in the prostate and its association with
emergence of androgen-independent prostate cancer. Cancer Res
1992; 52: 6940–44.
59 Small EJ, Roach M 3rd. Prostate-specific antigen in prostate cancer:
a case study in the development of a tumor marker to monitor
recurrence and assess response. Semin Oncol 2002; 29: 264–73.
60 Rodriguez R, Schuur ER, Lim HY, et al. Prostate attenuated
replication competent adenovirus (ARCA) CN706: a selective
cytotoxic for prostate-specific antigen-positive prostate cancer cells.
Cancer Res 1997; 57: 2559–63.
61 Wei C, Willis RA, Tilton BR, et al. Tissue-specific expression
of the human prostate-specific antigen gene in transgenic mice:
implications for tolerance and immunotherapy. Proc Natl Acad Sci
USA 1997; 94: 6369–74.
62 Bright RK, Vocke CD, Emmert-Buck MR, et al. Generation and
genetic characterization of immortal human prostate epithelial cell
lines derived from primary cancer specimens. Cancer Res 1997; 57:
995–1002.
63 Spitzweg C, O’Connor MK, Bergert ER, et al. Treatment of prostate
cancer by radioiodine therapy after tissue-specific expression of the
sodium iodide symporter. Cancer Res 2000; 60: 6526–30.
64 Sweat SD, Pacelli A, Murphy GP, Bostwick DG. Prostate-specific
membrane antigen expression is greatest in prostate adenocar-
cinoma and lymph node metastases. Urology 1998; 52: 637–40.
65 Wright GL Jr, Grob BM, Haley C, et al. Upregulation of prostate-
specific membrane antigen after androgen-deprivation therapy.
Urology 1996; 48: 326–34.
66 Uchida A, O’Keefe DS, Bacich DJ, et al. In vivo suicide gene therapy
model using a newly discovered prostate-specific membrane antigen
promoter/enhancer: a potential alternative approach to androgen
deprivation therapy. Urology 2001; 58 (suppl): 132–39.
67 Good D, Schwarzenberger P, Eastham JA, et al. Cloning and
characterization of the prostate-specific membrane antigen
promoter. J Cell Biochem 1999; 74: 395–405.
68 Matsubara S, Wada Y, Gardner TA, et al. A conditional
replication-competent adenoviral vector, Ad-OC-E1a, to cotarget
prostate cancer and bone stroma in an experimental model of
androgen-independent prostate cancer bone metastasis.
Cancer Res 2001; 61: 6012–19.
69 Foley R, Molloy K, Hollywood D, Lawler M. Suicide gene therapy
approaches for prostate cancer: potential synergy with radio-
therapy. Cancer Gene Ther 2000; 7 (suppl): S21–22 (abstr).
70 Majumdar S, Diamandis EP. The promoter and the enhancer region
of the KLK 3 (prostate specific antigen) gene is frequently mutated in
breast tumours and in breast carcinoma cell lines. Br J Cancer 1999;
79: 1594–602.
Review Gene therapy for prostate cancer
Oncology Vol 5 August 2004 http://oncology.thelancet.com
11. 479
71 Lee SJ, Kim HS, Yu R, et al. Novel prostate-specific promoter derived
from PSA and PSMA enhancers. Mol Ther 2002; 6: 415–21.
72 Freytag SO, Paielli D, Wing M, et al. Efficacy and toxicity of
replication-competent adenovirus-mediated double suicide gene
therapy in combination with radiation therapy in an orthotopic
mouse prostate cancer model. Int J Radiat Oncol Biol Phys 2002;
54: 873–85.
73 Yang C, Cirielli C, Capogrossi MC, Passaniti A. Adenovirus-
mediated wild-type p53 expression induces apoptosis and suppresses
tumorigenesis of prostatic tumor cells. Cancer Res 1995; 55: 4210–13.
74 Eastham JA, Hall SJ, Sehgal I, et al. In vivo gene therapy with p53 or
p21 adenovirus for prostate cancer. Cancer Res 1995; 55: 5151–55.
75 Nakanishi H, Mazda O, Satoh E, et al. Nonviral genetic transfer of
Fas ligand induced significant growth suppression and apoptotic
tumor cell death in prostate cancer in vivo. Gene Ther 2003;
10: 434–42.
ReviewGene therapy for prostate cancer
Oncology Vol 5 August 2004 http://oncology.thelancet.com
Clinical picture
A 69-year-old woman with nephrolithiasis and end-stage
renal disease presented at our clinic with recurrent, central
abdominal pain, which had persisted for 3 months. She had
been on haemodialysis for the past 10 years and had been
diagnosed with bilateral carpal tunnel syndrome.
Colonoscopy showed a circumferential tumour at the
transverse colon. After a preoperative diagnosis of
obstructive carcinoma of the colon, the patient had an
exploratory laparotomy. A bulky tumour was identified in
the proximal transverse colon adhering to a segment of the
mid-ileum, which needed an extended right hemicolectomy
and an en bloc resection of the ileum. Histological analysis
of the resected tissue (figure A) did not show any carcinoma
cells; instead, a pink amorphous deposit at the vessel wall in
the submucosa was noted. The amorphous substance stained
positively with Congo red and showed green birefringence
under polarised light.
3 years later, the patient was referred to a gynaecological
oncologist after she detected a 2-cm mass in her right vulva;
she underwent a Tru-cut biopsy. Histological analysis of the
vulval tissue showed extensive deposition of a fragmented
pink amorphous substance within fibrous tissue.
A diagnosis of dialysis-associated amyloidosis, which
manifested as a tumour-like subcutaneous vulval mass, was
made. Positive staining with Congo red (figure B)
supported this diagnosis.
Amyloidosis presenting as malignant disease
K M Chow, P C L Choi, and C C Szeto
Correspondence: Dr Kai Ming Chow, Department of Medicine and Therapeutics, Prince of Wales Hospital, Chinese University of Hong
Kong, Shatin, Hong Kong, China. Tel: +852 2632 3131. Fax: +852 2637 5396. Email: Chow_Kai_Ming@alumni.cuhk.net