2. Dear Author,
Please, note that changes made to the HTML content will be
added to the article before publication, but are not reflected
in this PDF.
Note also that this file should not be used for submitting
corrections.
4. U
N
C
O
R
R
E
C
T
E
D
P
R
O
O
F
79 Pettersson-Yeo et al., 2011; Uhlhaas, 2013; van den Heuvel and Fornito,
80 2014). Recent advances in non-invasive neuroimaging techniques such
81 as diffusion tensor imaging (DTI) and graph theoretical analysis have
82 enabled quantitative mapping of brain anatomical networks in unprec-
83 edented detail. Studies of structural brain networks in schizophrenia
84 have found the presence of small-world properties in these individuals
85 albeit that there is reduction of local network connectivity (Zalesky
86 et al., 2011), increases of minimum path length and network robustness
87 (Zhang et al., 2012), loss of hubs in frontal regions (Bassett et al., 2008;
88 van den Heuvel et al., 2010), abnormal rich club organization (highly in-
89 terconnected hubs) (van den Heuvel et al., 2013). Notwithstanding the
90 significance of these findings, evidence pertaining to the intactness of
91 overall brain anatomical connectivity has not been entirely consistent
92 (for reviews, see (Fornito et al., 2012; Griffa et al., 2013)). It is also
93 worth noting that reported aberrations in structural brain networks
94 are found exclusively in cross sectional studies. As structural changes
95 can manifest and alter at various stages throughout life, longitudinal
96 studies are crucial if a more comprehensive understanding of brain ar-
97 chitecture differences and their implications is to be achieved
98 (Pfefferbaum et al., 2013). Although several longitudinal volumetric
99 studies have been successful in shedding light on important focal
100 changes in GM and WM of patients with schizophrenia (Andreasen
101 et al., 2011; Asami et al., 2012; Whitford et al., 2007), the question of
102 how network properties in schizophrenia are conserved or affected
103 over time is still largely unexplored.
104 To the best of our knowledge, this is the first study employing graph
105 theory analysis for investigating longitudinal effects of schizophrenia on
106 structural brain networks. By applying a longitudinal design over
107 5 years, we recorded repeated DTI images in 31 patients with schizo-
108 phrenia and 28 age- and gender-matched healthy individuals. Whole-
109 brain anatomical networks were constructed using the commonly
110 used deterministic tractography approach. We calculated several net-
111 work measures to assess small-world properties (e.g., clustering coeffi-
112 cient, path length, and small-worldness), global and local efficiencies,
113 and relative nodal characteristics. In the context of significance of inves-
114 tigation structural brain network topological changes in schizophrenia
115 and paucity of longitudinal data, we set out to assess: 1) how network
116 architecture is aberrant in schizophrenia, 2) how these disruptions
117 change over time, and 3) whether there is any longitudinal association
118 between the disrupted network topology and clinical variables.
119 2. Methods and materials
120 2.1. Participants
121 In this study, thirty-one patients experiencing schizophrenia and
122 twenty-eight matched healthy comparison subjects were recruited at
123 baseline from the Institute of Mental Health (IMH), Singapore, and the
124 local community by advertisements respectively. All the subjects partic-
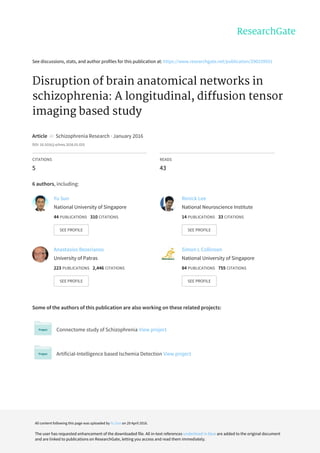
125 ipated in the follow up study with a mean gap of around 5 years. Scan
126 intervals of each participant were shown in Fig. 1. Diagnostic evaluation
127 was performed by a board-certificated psychiatrist (K. S.). The inclusion
128 and exclusion criterial are detailed in the Supplementary materials. This
129 study was approved by the Institutional Review Boards of the IMH,
130 Singapore, as well as the National Neuroscience Institute (NNI),
131 Singapore, and informed consent was obtained from each participant.
132 Antipsychotic medication dosage was recorded at baseline and mean
133 dose at follow-up was calculated by averaging the cumulative received
134 antipsychotic dose over the period of treatment. The socio-demographic
135 and clinical features of the subjects are shown in Table 1.
136 2.2. Data acquisition
137 Structural magnetic resonance images with consistent high signal-
138 to-noise ratio were recorded using a 3-Tesla whole body scanner
139 (Philips Achieva, Philips, Medical System, Eindhoven, The
140Netherlands) using an eight-element SENSE receiver head-coil at the
141National Neuroscience Institute, Singapore. A T1-weighted Magnetiza-
142tion Prepared Rapid Gradient Recalled Echo sequence (repetition time
143[TR] = 7.2 ms; echo time [TE] = 3.3 ms; flip angle = 8°) was utilized
144to obtain high-resolution T1-weighted MRI volume images (each vol-
145ume contains 180 gapless axial slices of 0.9 mm thickness, field of
146view [FOV] = 230 × 230 mm2
; acquisition matrix = 256 × 256; in-
147plane resolution: 0.9 × 0.9 mm2
) in the direction of the anterior–poste-
148rior commissures (AC–PC). A single-shot echo-planar sequence (TR =
1493275 ms; TE = 56 ms; flip angle = 90°; b-factor = 800 s/mm2
; 1 base-
150line image with b = 0 s/mm2
) from 15 separate non-parallel directions
151was utilized to obtain diffusion encoded images (each volume contain-
152ing 42 slices, 3.0 mm with no gap; FOV = 230 × 230 mm2
; acquisition
153matrix = 112 × 109, reconstructed to 256 × 256). For each participant,
154the diffusion sequences were scanned three times to improve the
155signal-to-noise ratios. During the scanning, head motion was minimized
156using restraining foam pads provided by the manufacturer. The same
157scanner was used for both the baseline (software version R2.6) and
158follow-up scans (software version R3.2). The scanning settings were
159maintained for both baseline and follow-up studies.
1602.3. Data preprocessing and structural brain network construction
161Data preprocessing and structural brain network construction were
162conducted using FSL (Smith et al., 2004), diffusion toolkit (Wang et al.,
1632007), and PANDA (Cui et al., 2013), and had been described in detail
164previously (Sun et al., 2015). In short, preprocessing approaches in-
165cluded correction for head motion and eddy current distortions through
166registering the DW images to the b0 image with an affine transforma-
167tion. The gradient direction of each DWI volume was rotated according
168to the resultant affine transformations to further reduce the influence of
169motion artifacts (Leemans and Jones, 2009). Six elements of the diffu-
170sion tensor were then estimated from which fractional anisotropy
171(FA) was calculated. Whole-brain fiber tractography was subsequently
172performed using fiber assignment by continuous tracking (FACT) algo-
173rithm (Mori et al., 1999). This algorithm computes fiber trajectories
174starting from the deep WM regions and terminating at a voxel with a
Fig. 1. Age at scan for longitudinal study. Each subject is shown in a different row, with
their scans connected by a straight line. Healthy participants (blue) and patients with
schizophrenia (red) are marked separately. Most subjects received two scans
approximately 5 years apart. There was no statistical (p N 0.05) difference in scan
intervals between both groups. (For interpretation of the references to color in this
figure legend, the reader is referred to the web version of this article.)
2 Y. Sun et al. / Schizophrenia Research xxx (2015) xxx–xxx
Please cite this article as: Sun, Y., et al., Disruption of brain anatomical networks in schizophrenia: A longitudinal, diffusion tensor imaging based
study, Schizophr. Res. (2015), http://dx.doi.org/10.1016/j.schres.2016.01.025
5. U
N
C
O
R
R
E
C
T
E
D
P
R
O
O
F
175 turning angle greater than 45° or at a voxel with FA less than 0.15. For
176 each subject, the structural brain network was then constructed by
177 combining the individual parcellation map with the WM tractography.
178 Here the widely used automated anatomical labeling (AAL) parcellation
179 scheme (90 regions in total) was used (Tzourio-Mazoyer et al., 2002).
180 These regions served as nodes within the structural brain network.
181 The parcellation process was conducted in the native DTI space for
182 each subject. Edge weight (wij) was computed as the multiplication of
183 fiber number (FN) by the mean FA along the fiber bundles between a
184 pair of cortical regions, wij = FAij × FNij (Betzel et al., 2014; Lo et al.,
185 2010). As a result, we constructed the weighted structural brain net-
186 work (90 × 90) for each participant at baseline and follow-up. Details
187 about the network construction can be found in the Supplementary ma-
188 terials (Supplementary Fig. 2).
189 2.4. Graph theoretical analysis of structural brain networks
190 Graph theoretical analysis was adopted to provide quantitative met-
191 rics to examine any difference in topological organization of structural
192 brain network between schizophrenia and healthy comparison con-
193 trols. In this study, we investigated the network architecture at both
194 global and regional levels for the constructed structural brain networks.
195 Global network architecture was quantified in terms of small-world
196 properties (weighted clustering coefficient, Cw; weighted characteristic
197 path length, Lw; and small-worldness, σ) and efficiency (global effi-
198 ciency, Eglobal; and local efficiency, Elocal). An exploratory analysis of
199 the behavior of each node was described in terms of nodal efficiency
200 (Enodal(i)). Here we provide brief, formal definitions of each of the met-
201 rics used in this study (Table 2). Greater details of the formations and in-
202 terpretations of the graph theoretical parameters can be found in the
203 Supplementary materials and reviews of this topic (Boccaletti et al.,
204 2006; Bullmore and Sporns, 2009; Rubinov and Sporns, 2010).
2052.5. Statistical analysis
2062.5.1. Longitudinal group differences
207Separate two-sample two-tailed t-test was used to test the group
208differences in baseline age, height, WRAT scores, and follow-up inter-
209vals. The gender and handedness data were analyzed using a two-
210tailed Pearson χ2
test. To assess longitudinal effects on network attri-
211butes between patients and normal controls, a general linear model
t1:1 Table 1
t1:2 Demographic and clinical features of the samples.a
t1:3 Characteristic Group (patients/controls = 31/28) Statistical
t1:4 Patients with schizophrenia Healthy controls t57 p
t1:5 Baseline scan
t1:6 Age (years) 19–54 (31.9 ± 9.7) 22–54 (31.8 ± 9.3) 0.033 0.974b
t1:7 Gender: male/female 14/17 13/15 – 0.922c
t1:8 WRAT scoresd
33–57 (50.2 ± 5.8) 40–57 (49.9 ± 4.6) 0.270 0.788b
t1:9 Handedness: right/left 29/2 25/3 – 0.557c
t1:10 Education (years) 9–16 (12.0 ± 2.0) 10–18 (14.3 ± 2.1) 4.338 b0.001b
t1:11 Age of onset 15–47 (24.8 ± 7.4) – – –
t1:12 Duration of illness (years) 3.4–40.4 (11.8 ± 8.6) – – –
t1:13 Medication dosage (mg/day)e
0–700 (234.7 ± 184.7) – – –
t1:14 Antipsychotic medication type: typical/atypical 6/25 – – –
t1:15 PANSS positive symptomsf
7–20 (9.9 ± 3.5) – – –
t1:16 PANSS negative symptoms 7–23 (9.2 ± 3.9) – – –
t1:17 PANSS general symptoms 16–32 (20.0 ± 3.4) – – –
t1:18 PANSS total 30–68 (39.2 ± 8.3) – – –
t1:19
t1:20 Second scang
t1:21 Follow-up interval (months)h
26–83 (54.5 ± 14.9) 38–83 (61.3 ± 12.5) −1.870 0.067b
t1:22 Medication dosage (mg/day)e
0–550 (221.3 ± 164.7) – – –
t1:23 Antipsychotic medication type: typical/atypical 6/25 – – –
t1:24 PANSS positive symptoms 7–14 (8.3 ± 2.2) – – –
t1:25 PANSS negative symptoms 7–15 (9.4 ± 2.6) – – –
t1:26 PANSS general symptoms 16–28 (19.1 ± 3.4) – – –
t1:27 PANSS total 30–55 (36.8 ± 6.3) – – –
t1:28 a
Data are expressed as the range of minimum–maximum (mean ± standard deviation).
t1:29 b
The p-value was obtained using a two-sample two-tailed t-test.
t1:30 c
The p-value was obtained using a two-tailed Pearson χ2
test.
t1:31 d
Wide Range Achievement Test (WRAT) reading subscales was estimated according to (Stone et al., 1995) for the IQ evaluation.
t1:32 e
Chlorpromazine (CPZ) equivalents doses were calculated using conversion rates according to (Woods, 2003).
t1:33 f
The positive and negative symptoms scale (PANSS) (Kay et al., 1987) was used to assess the psychopathology and symptom severity.
t1:34 g
Comparisons of clinical metrics between baseline and follow-up were shown in supplementary Fig. 1.
t1:35 h
Scan intervals of each participant were shown in Fig. 1.
t2:1Table 2
t2:2Introduction of topological measurements (including five global network metrics and one
t2:3nodal metric) and their meaning in structural brain networks.
t2:4Network properties Measurement and meaning
t2:5Global characteristics
t2:6Weighted clustering
t2:7coefficient (Cw)
Cw measures the extent of a local density or
cliquishness of the network.
t2:8Weighted characteristic
t2:9path length (Lw)
Lw measures the average minimal travel distance
between nodes in the network. It represents the global
integration of the network.
t2:10Small-worldness (σ) σ ¼
Cw =Crand
w
Lw =Lrand
w
is a scalar measurement of the small-world
property of a network, where Cw
rand
and Lw
rand
denote
the average Cw and Lw of an ensemble of 100 surrogate
random networks. A small-world network has high
local clustering and short paths between brain regions.
t2:11Local efficiency (Elocal) Elocal is a measure of the information exchange at the
clustering level.
t2:12Global efficiency (Eglobal) Eglobal is a measure of the global efficiency of parallel
information transfer in the network. It is inversely
related to Lw.
t2:13
t2:14Nodal characteristics
t2:15Nodal efficiency (Enodal) Enodal(i) is the inverse of the harmonic mean of the
shortest path length between node i and all other
nodes. A region with high Enodal indicates great
interconnectivity with other regions in the network.
3Y. Sun et al. / Schizophrenia Research xxx (2015) xxx–xxx
Please cite this article as: Sun, Y., et al., Disruption of brain anatomical networks in schizophrenia: A longitudinal, diffusion tensor imaging based
study, Schizophr. Res. (2015), http://dx.doi.org/10.1016/j.schres.2016.01.025
6. U
N
C
O
R
R
E
C
T
E
D
P
R
O
O
F
212 (GLM) comprising of longitudinal scan point (baseline vs. follow-up) as
213 a within-subject factor, group (NC vs. SCZ) as a between-subject factor,
214 and the scan point by group as an interaction, was performed on the ob-
215 tained network metrics. Gender, baseline age, and gender-by-age inter-
216 action were set as covariates. If any main effect was found to be
217 significant, further post-hoc t-tests were performed (paired t-test for
218 longitudinal scan point effect and two-sample two-tailed t-test for
219 group effect). All statistical analyses were performed using SPSS 17 soft-
220 ware. A value of p b 0.05 was considered significant for the global prop-
221 erties analysis. An uncorrected p-value of 0.01 was considered for
222 establishment of a significant difference for the regional characteristics.
223 To address the problem of multiple comparisons, effects were also
224 tested on whether they survived a false discovery rate (FDR) threshold
225 of q = 0.05.
226 2.5.2. Relationship between network metrics and clinical variables
227 Relationships between the global network measures and clinical
228 variables were also explored in the patient group. Specifically, a gener-
229 alized estimated equation (GEE) model (Zeger et al., 1988) with ex-
230 changeable working correlation matrix was employed and
231 implemented in the statistical package, R (http://www.r-project.org/)
232 in the current study. Effects of gender, baseline age, and age-by-gender
233 interaction were controlled for the correlation analyses. The threshold
234 value for establishment of a significant relationship was set at p b 0.05.
235 3. Results
236 3.1. Clinical measurements
237 There were no statistical differences (all p N 0.05) between the
238 healthy participants and patients with schizophrenia with respect to
239 age at scan, gender, baseline WRAT scores, handedness, or the time in-
240 terval between scans (follow-up interval) (Table 1). For the clinical
241 measurements of patients between the baseline and follow-up study,
242 a significant decrease (t30 = 2.188, p = 0.037) was found in the
243 PANSS positive symptoms, whereas the rest of the clinical metrics
244 (medication dosage, PANSS negative symptoms, PANSS general symp-
245 toms, PANSS overall scores) did not show any significant change (all
246 p N 0.05) over time (Supplementary Fig. 1).
247 3.2. Group differences of global topological organization over time
248 The brain networks of both groups exhibited typical features of
249 small-world topology at both scans (Supplementary Fig. 3). Additional
250 quantitative statistical analyses revealed significant changes in global
251 network metrics between both groups over time (Table 3). Specifically,
252 a main effect of longitudinal scan was observed in the small-worldness,
253 σ, (follow-up N baseline, F1, 57 = 4.991, p = 0.029). Group main effect
254was highly significant in Lw (NC b SCZ, F1, 54 = 9.920, p = 0.003) and
255Eglobal (NC N SCZ, F1, 54 = 9.863, p = 0.003), suggesting a reduced global
256integration of the brain network in patients with schizophrenia. Inter-
257estingly, significant interaction was revealed in Lw (F1, 57 = 7.833,
258p = 0.007) and Eglobal (F1, 57 = 4.787, p = 0.033). Post hoc analysis
259shows that this significant interaction resulted from different develop-
260ment trends in normal controls and patients with schizophrenia
261(Fig. 2). i.e., compared to healthy controls who exhibit progressive im-
262provements in global integration (Lw: baseline N follow-up, t27 =
2632.531, p = 0.018; Eglobal: baseline b follow-up, t27 = −1.795, p =
2640.084), patients with schizophrenia showed insignificant worsen global
265integration in the follow-up scan (Lw: baseline b follow-up,
266t30 = −1.482, p = 0.149; Eglobal: baseline N follow-up, t30 = 1.182,
267p = 0.246).
2683.3. Group differences of regional topological organization over time
269Significant group effect was revealed on the nodal characteristic of 6
270regions (Fig. 3(A), Supplementary Table 2), where four of them (the left
271inferior frontal gyrus, triangular part, [IFGtriang.L] (p = 0.004), the right
272paracentral lobule, [PCL.R] (p = 0.002), and the bilateral insula, [INS]
273(INS.L, p = 0.004; INS.R, p = 0.002)) exhibited normal controls advan-
274tage, i.e., NC N SCZ. Regions with significant ‘NC b SCZ’ effect were the
275left superior frontal gyrus, medial part, [SFGmed.L] (p = 0.007) and
276the left supramarginal gyrus, [SMG.L] (p = 0.007). In addition, both pos-
277itive and negative time effects were found at 11 regions in total (Fig. 3
278(B), Supplementary Table 2), where half of these regions (6 among
27911), predominantly located in the left temporal and right parietal
280areas, including the left fusiform gyrus, [FFG.L] (p = 0.0003 *, * indicates
281region survived FDR threshold at q b 0.05); the left Heschl gyrus, [HES.L]
282(p = 0.0006 *); the left lingual gyrus, [LING.L] (p b 0.0001 *); the left
283caudate nucleus, [CAU.L] (p = 0.001 *) and the right caudate nucleus,
284[CAU.R] (p = 0.009), showed decreased nodal efficiency in the follow-
285up scan. Regions with significant increased nodal efficiency were mainly
286resided in the left occipital and right temporal areas, including the left
287superior occipital gyrus, [SOG.L] (p = 0.005); the right superior tempo-
288ral gyrus, [STG.R] (p = 0.004); the right temporal pole, superior part,
289[TPOsup.R] (p = 0.0010 *); the bilateral temporal pole, middle part,
290[TPOmid] (TPOmid.L, p = 0.0002 * and TPOmid.R p = 0.0008 *). More
291interesting, a significant interaction effect was observed in the left infe-
292rior frontal gyrus, opercula part, [IFGoperc.L] (p = 0.010) and right thal-
293amus, [THA.R] (p = 0.009) (Fig. 3(C), Supplementary Table 2). The post-
294hoc analysis with regard to the interaction revealed that this significant
295interaction effect was attributed to the significant progressive increase
296of nodal efficiency in healthy volunteers and a non-significant decrease
297of nodal characteristics over time in patients with schizophrenia.
2983.4. Relationship between network topology and clinical features
299We found a longitudinal association between reducing PANSS gen-
300eral scores and increasing weighted characteristic path length, Lw, (stan-
301dardized coefficient, β = −2.535, p = 0.046) and decreasing global
302efficiency, Eglobal, (β = 3.211, p = 0.013). Of note, Lw measures the over-
303all routing efficiency of the network and is inversely related to Eglobal,
304hence leading to converse correlations for both. Specifically, a develop-
305ment trend of insignificantly reduced PANSS general scores significantly
306correlates with a progression toward longer characteristics path length
307or smaller global efficiency. More interestingly, significantly reduced
308PANSS positive scores was found to be correlated with the small-
309worldness (β = −3.520, p = 0.036) in patients with schizophrenia, re-
310vealing different development trends between lower PANSS positive
311scores and higher small-worldness.
t3:1 Table 3
t3:2 Comparison of longitudinal brain network topographical changes between patients with
t3:3 schizophrenia and healthy participants.
t3:4 Network metrics General linear model (GLM)
t3:5 Group
t3:6 F1, 54 (p-value)
Scan-point
F1, 57 (p-value)
Interaction
F1, 57 (p-value)
t3:7 Cw 2.487 (0.121) 0.078 (0.782) 0.372 (0.545)
t3:8 Lw 9.920 (0.003)▲
0.428 (0.516) 7.833 (0.007)
t3:9 σ 0.074 (0.787) 4.991 (0.029)↑
0.354 (0.554)
t3:10 Eglobal 9.863 (0.003)▼
0.325 (0.571) 4.787 (0.033)
t3:11 Elocal 1.534 (0.221) 0.064 (0.801) 0.970 (0.329)
t3:12 Global network metrics are expressed as mean ± standard deviation. The statistical results
t3:13 were computed with a general linear model (GLM) with longitudinal scan point as a
t3:14 within-subject fact, group as between-subject factor, and longitudinal scan point by
t3:15 group as interaction. The effect of age at baseline, gender, and age-by-gender interaction
t3:16 were adjusted for all of these analyses. Bold indicates variables that are statistically signif-
t3:17 icant (p b 0.05).
t3:18 Note: ▼
, patients b controls, ▲
, patients N controls, ↑
, follow-up N baseline.
4 Y. Sun et al. / Schizophrenia Research xxx (2015) xxx–xxx
Please cite this article as: Sun, Y., et al., Disruption of brain anatomical networks in schizophrenia: A longitudinal, diffusion tensor imaging based
study, Schizophr. Res. (2015), http://dx.doi.org/10.1016/j.schres.2016.01.025
7. U
N
C
O
R
R
E
C
T
E
D
P
R
O
O
F
312 4. Discussion
313 By applying a longitudinal design over 5 years, this study investi-
314 gated the longitudinal changes in structural brain networks in schizo-
315 phrenia for the first time. The significant findings are as follows: first,
316 a scan-point independent significant deficit of global integration was
317 found in patients with schizophrenia; second, compared with healthy
318 controls who exhibited an improvement in global integration, patients
319 with schizophrenia showed a decrease of global integration over time;
320 third, two specific brain regions (the left inferior frontal gyrus, opercula
321 part, and the right thalamus) showed a significant group-by-longitudi-
322 nal scan interaction effect, attributing to a progressive increase of
323nodal efficiency in healthy controls compared to patients; and fourth,
324the disruption of the brain anatomical network was longitudinally cor-
325related with the clinical symptom ratings on the PANSS in patients with
326schizophrenia.
327The identification of small-world architecture has made a great im-
328pact on our understanding the topological organization of brain net-
329works (Bullmore and Sporns, 2009). In particular, small-world
330architecture is characterized by high local clustering of connections be-
331tween neighboring brain regions but with short path length. This char-
332acteristic is thought to provide the brain with an optimal structure to
333simultaneously support locally segregated and globally integrated pro-
334cessing (Sporns, 2011). Moreover, this neural architecture has the
Fig. 2. Post-hoc statistical analysis of global network metrics. Normal controls and patients with schizophrenia are marked separately: NC1 = normal controls at baseline (unfilled blue
triangle), NC2 = normal controls at follow-up (filled blue triangle), SCZ1 = patients at baseline (unfilled red circle), and SCZ2 = patients at follow-up (filled red circle). Median
values of the network metrics are marked with a horizontal line for each group. Each number represents the p-value of a t-test (paired t-test for longitudinal scan point effect and
two-sample two-tailed t-test for group effect). (For interpretation of the references to color in this figure legend, the reader is referred to the web version of this article.)
Fig. 3. The spatial distribution of cortical regions showing significant effect of (A) group, (B) scan point, and (C) group-by-scan point interaction on the nodal characteristics and the post-
hoc statistical analysis for the significant interaction effect. The color bar represents F values. Significant (gray background, p b 0.05, FDR-corrected; no-background, p b 0.01, uncorrected)
regions are overlaid on inflated surface maps at the Medium view with BrainNet Viewer software (Xia et al., 2013). The nodal regions are located according to their centroid stereotaxic
coordinates. For the abbreviations of the cortical regions, see Supplementary Table 1. Of note, the subcortical regions including the bilateral CAU in (B) were not presented in the surface
spatial distribution here. L = left, R = right. (For interpretation of the references to color in this figure legend, the reader is referred to the web version of this article.)
5Y. Sun et al. / Schizophrenia Research xxx (2015) xxx–xxx
Please cite this article as: Sun, Y., et al., Disruption of brain anatomical networks in schizophrenia: A longitudinal, diffusion tensor imaging based
study, Schizophr. Res. (2015), http://dx.doi.org/10.1016/j.schres.2016.01.025
8. U
N
C
O
R
R
E
C
T
E
D
P
R
O
O
F
335 capacity to process information in parallel, which is computationally
336 much more efficient than serial or hierarchical processing. Here we
337 found that the brain structural networks of both groups exhibited typi-
338 cal features of small-world topology at both scans. These findings were
339 consistent with prior observations in both healthy participants (Iturria-
340 Medina et al., 2008) and patients with schizophrenia (van den Heuvel
341 et al., 2010; Zalesky et al., 2011). Given that the small-world topology
342 is robust to random and targeted disruptions, the presence of typical
343 small-world architecture in patients with schizophrenia at both scan
344 points may suggest compensatory reactions to developmental
345 neuropathology.
346 In addition, we found a significant deficit of global integration inde-
347 pendent of scan points in patients with schizophrenia. This observation
348 was consistent with prior findings from functional (Liu et al., 2008) and
349 structural network studies (Ottet et al., 2013; Wang et al., 2012; Zhang
350 et al., 2012), which have shown increased connection distance within
351 brain networks in schizophrenia in comparable age groups. Therefore,
352 our finding adds to earlier work and provides further evidence
353 supporting the notion of schizophrenia as a disconnection syndrome.
354 More importantly, we found a significant interaction effect in the global
355 integration, i.e., patients with schizophrenia exhibited a development
356 trajectory heading toward less global efficiency of brain anatomical net-
357 works while healthy controls showed an improvement in global inte-
358 gration. In accordance with our observation in healthy subjects, Wu
359 and colleagues found in their longitudinal study of healthy adults that
360 improved brain topological architecture related to structural brain net-
361 work changes occurring from young to middle age (Wu et al., 2013).
362 Similar observations of improved network integration were also found
363 in a recent cross sectional study of the structural connectome in adoles-
364 cents and adults (Dennis et al., 2013). Previous evidence suggested that
365 high global integration assures effective integrity or rapid transfers of
366 information across remote regions that are believed to constitute the
367 basis of cognitive processing (Sporns and Zwi, 2004). More recently, Li
368 et al. revealed a positive correlation between the global integration of
369 anatomical brain networks and intellectual performance (Li et al.,
370 2009). Therefore, our finding of improvement in global integration in
371 normal controls may reflect a maturation process in the network. Whilst
372 there is no comparable longitudinal anatomical data involving small-
373 world properties in schizophrenia, these trends were consistent with
374 most cross sectional observations to data across different age spans,
375 suggesting that disruption of brain topological networks and impaired
376 higher order neural function in schizophrenia occurs over time (for re-
377 views, see (Fornito et al., 2012; van den Heuvel and Fornito, 2014)). In
378 one meta-analysis of longitudinal volumetric deficits in schizophrenia
379 investigating 27 studies with a total of 928 patients, Olabi et al. found
380 progressive brain volume reduction (Olabi et al., 2011). More recently,
381 Asami and colleagues showed in their longitudinal neuroimaging volu-
382 metric study that patients with schizophrenia showed widespread GM
383 volume reductions in brain neocortical regions including frontal, parie-
384 tal, and limbic regions when compared to heathy participants and these
385 volumetric reductions were not correlated with medication dosage
386 (Asami et al., 2012). Cerebral GM contains neuronal cell bodies, den-
387 drites, and short protrusions which play an important role in informa-
388 tion processing. Our observation of a progressive trend toward less
389 economical topology of brain networks might be attributed to the sig-
390 nificant concomitant loss of GM in patients with schizophrenia occur-
391 ring over time.
392 Aberrations of nodal characteristics are increasingly implicated in
393 normal aging (Wu et al., 2012) or various brain diseases (Crossley
394 et al., 2014), and may underlie the neuropsychiatric basis for schizo-
395 phrenia symptoms (for a review, see (Rubinov and Bullmore, 2013)).
396 In line with previous studies, we found that schizophrenia was associ-
397 ated with reduced regional efficiency in the left inferior frontal gyrus,
398 right paracentral lobule as well as the bilateral insula and increased
399 nodal efficiency in the left superior frontal gyrus and the left
400 supramarginal gyrus. Insula, a cortical structure with extensive
401connections to many areas of the cortex and limbic system, has repeat-
402edly showed functional and structural deficits in patients with schizo-
403phrenia (for a review, see (Wylie and Tregellas, 2010)). Moreover, in
404healthy subjects, the insula and inferior frontal gyrus were typically
405identified as hubs, which played a central role in receiving convergent
406inputs from multiple cortical regions (He et al., 2007; Iturria-Medina
407et al., 2008; Wu et al., 2012). Taken together, we speculate that the pro-
408foundly affected regional centrality in these hub regions may indicate
409more isolated network architecture in schizophrenia, leading toward
410the observed deficits in global integration. In addition, both positive
411and negative longitudinal time effects on regional efficiency were
412found across cerebral cortex, suggesting a putative compensatory
413mechanism of cortical network reorganization over time (Park and
414Reuter-Lorenz, 2009). The results of this longitudinal study extend the
415findings of aging modulated regional efficiency in several cross-
416sectional connectivity studies (Dennis et al., 2013; Gong et al., 2009b)
417and support the view that longitudinal changes are primary characteris-
418tics of the association and paralimbic cortex as opposed to primary cor-
419tex (Albert and Knoefel, 2011). Of note, several brain regions, including
420the superior occipital gyrus, the superior temporal gyrus, the fusiform
421gyrus, and the lingual gyrus, consistently exhibited an alteration of re-
422gional efficiency with normal aging (Gong et al., 2009b; Wu et al.,
4232012). Furthermore, we found a significant interaction effect on nodal
424efficiency of the left inferior frontal gyrus, opercula part, [IFGoperc.L]
425and the right thalamus, [THA.R] attributed to a deficit of improvement
426in patients. In previous longitudinal volumetric neuroimaging studies,
427considerable loss of both GW and WM in these regions was consistently
428revealed in schizophrenia (Andreasen et al., 2011; Asami et al., 2012).
429Another interesting finding of the current study is that within pa-
430tients, the longitudinal course of the alterations of the network topolog-
431ical properties was associated with clinical symptom progression on the
432PANSS. Specifically, we found different progression trends between sig-
433nificantly reduced PANSS positive scores and the increased small-
434worldness. Since the small-worldness represents the balance between
435local clustering and global integration; the smaller PANSS positive
436scores over time, the higher the small-worldness, the correlation was
437in the expected direction. When combined with the observations of
438small-world characteristics across two scan points, this finding might
439suggest that maintenance of the optimal small-world properties is re-
440lated to improvement in positive symptoms. Moreover, a longitudinal
441association between the reduced PANSS general symptoms and wors-
442ening global integration was also revealed, suggesting some degree of
443specificity in the way that distinct symptoms correlate with overall con-
444nectivity variations in different neural circuits (Fornito et al., 2012;
445Meyer-Lindenberg and Weinberger, 2006). As revealed by van den
446Heuvel and Fornito in their recent review paper of connectomic findings
447in schizophrenia, a robust relationship between abnormal network or-
448ganization and schizophrenia clinical symptoms has emerged (van
449den Heuvel and Fornito, 2014). Our findings therefore support a general
450trend in the literature showing a direct correspondence between net-
451work measurements and clinical symptomatology and suggest the use-
452fulness of brain network properties as potential biomarkers for
453evaluation the severity and progression of the disease.
454Longitudinal investigations of the disruptions of structural brain net-
455works in schizophrenia, as in this study, are significant for several rea-
456sons. First, they allow better appreciation of the extent of brain
457network properties that are affected over time in schizophrenia which
458may suggest specific biomarkers of illness progression. Second, how
459these brain network properties relate to specific brain regions over
460time can highlight underlying neural pathways disruptions in these
461complex brain networks. Third, prospective anatomical connectivity
462disturbances can complement extant and future functional connectivity
463evaluation in order to better understand the circuitry disturbances in
464schizophrenia. Fourth, examining changes in the network properties
465over time can suggest mechanisms being exerted to maintain the effi-
466ciency of brain networks in illness. Taken together, we believe that
6 Y. Sun et al. / Schizophrenia Research xxx (2015) xxx–xxx
Please cite this article as: Sun, Y., et al., Disruption of brain anatomical networks in schizophrenia: A longitudinal, diffusion tensor imaging based
study, Schizophr. Res. (2015), http://dx.doi.org/10.1016/j.schres.2016.01.025
9. U
N
C
O
R
R
E
C
T
E
D
P
R
O
O
F
467 employing longitudinal design in addition to cross sectional studies is
468 important for more comprehensive understanding of the neural mech-
469 anisms of various brain diseases and how they manifest and evolve
470 throughout life.
471 Several issues need to be further addressed. First, the effect of differ-
472 ent medication dosage among patients across both scan points might
473 potentially be a confounding factor. For instance, previous neuroimag-
474 ing studies of schizophrenia have reported pharmacological changes
475 in localized brain regions and connections (Andreasen et al., 2011;
476 Kanaan et al., 2009; Navari and Dazzan, 2009). Nonetheless, evidence
477 pertaining to the association between network measurements and
478 medication dosage are not entirely consistent (Liu et al., 2008;
479 Micheloyannis et al., 2006). Some have suggested that medication is un-
480 likely to be a confounding factor and may, on the contrary, exert to a
481 normalizing influence (Rubinov et al., 2009). Moreover, the significant
482 difference between groups in years of education may also be a potential
483 confounding factor. To address these issues, we performed separate sta-
484 tistical analysis with medication dosage and years of education as addi-
485 tional covariates and found the key results of the study remain
486 unchanged (data not shown). As such, we consider that the observed
487 longitudinal effect reflects the intrinsic disease process rather than the
488 effect of direct pharmacological treatment or group differences in
489 years of education. Second, in this study, structure brain network edge
490 weight was constructed with considering the fiber number (FN) and
491 FA values. FA value is an important index to evaluate fiber integrity
492 (Beaulieu, 2002) and exhibits a high correlation with conductivity
493 (Tuch et al., 2001); and FN may reflect the white matter structure
494 (Hagmann et al., 2007). Through calculating the multiplication of FN
495 and FA, the edge weight would provide a comprehensive view of
496 white matter anatomical structure. To obtain the FN and FA values, a
497 computationally inexpensive deterministic local tensor based
498 tractography method was used. However, due to the fiber crossing
499 problem, the deterministic method always terminates the fiber tracking
500 when it reaches regions with fiber crossing and low FA values, which
501 may lead to the loss of some existing fibers between brain regions or
502 to the inclusion of some non-existent fibers (Li et al., 2009). In the Sup-
503 plementary materials (Supplementary Fig. 4), we assessed the credibil-
504 ity of our tracking results through showing seven well-known WM fiber
505 bundles (including 2 short white matter tracts and 5 major tracts) from
506 four randomly selected subjects at baseline. Consequently, the recon-
507 structed fiber bundles are faithful to the human WM anatomy from pre-
508 vious studies (Gong et al., 2009a; Li et al., 2009). Furthermore, structural
509 connectivity networks reconstructed in this study exhibited attributes
510 that are consistent with previous cross-sectional brain connectome
511 studies of schizophrenia (Griffa et al., 2013; Uhlhaas, 2013; van den
512 Heuvel and Fornito, 2014). Nonetheless, a probabilistic tractography
513 may be a better solution for future studies as recent studies have dem-
514 onstrated the better performance in overcoming the fiber crossings
515 and robustness to the image noise (Buchanan et al., 2014). Third, the
516 widely used AAL template (Tzourio-Mazoyer et al., 2002) was used to
517 define the nodes of the brain anatomical networks. Recent studies
518 have revealed that different parcellation scales might result in different
519 properties of brain networks (Fornito et al., 2010; Zalesky et al., 2010).
520 Furthermore, regions on the AAL template differ in size, which may
521 have a confounding effect on the link weight of the network nodes
522 (van den Heuvel et al., 2010; Wang et al., 2012). To verify this, we per-
523 formed a post-hoc analysis on the region size difference between both
524 groups at both baseline and follow-up and found no significant result
525 (data not shown), suggesting an equivalent effect of region size on the
526 network metrics in both groups. Although several network edge
527 weighting methods (e.g., streamline density and streamline density
528 with fiber length correction) have been introduced to compensate the
529 ROI size effect (Buchanan et al., 2014; Hagmann et al., 2008), the choice
530 of the most accurate representation of the underlying neurobiological
531 connectivity remains an open question (Jones et al., 2013). The primary
532 focus of the current work is to investigate the longitudinal disruption of
533the brain anatomical network in schizophrenia. We believe that graph
534theoretical analyses with different spatial resolutions and more accurate
535edge weighting method in future studies would be important for better
536understanding the etiology and its progression of schizophrenia. Finally,
537as our study is one of the first exploratory investigations of longitudinal
538effects of schizophrenia on the structural brain network, an uncorrected
539p-value of 0.01 was employed for establishing the significance and pre-
540senting the regional results. It is possible that some of the nodal results
541may have occurred by chance and some caution is needed when
542interpreting these results. In the current study, we focused primarily
543on the interpretation of the general pattern of the findings and
544highlighted those survived multiple comparisons correction for the
545reader's interpretation. Nonetheless, future studies using a larger inde-
546pendent longitudinal study sample with multiple intervals and
547hypothesis-driven study design are expected to confirm our
548observations.
549In conclusion, in this first-ever brain connectome study of longitudi-
550nal changes in brain structural networks in schizophrenia, we found
551progressive disruption of brain anatomical networks in patients with
552schizophrenia, which correlated with the clinical symptoms longitudi-
553nally. These findings highlight the potential of brain network measures
554as neural biomarkers for clinical presentation, illness progress as well as
555response to treatment.
556Role of funding source Q3
557This work was supported by the National Healthcare Group (NHG 11003 & NHG
55812003) awarded to Kang Sim, and the Agency for Science, Technology, Research/
559Singapore BioImaging Consortium (ASTART/SBIC009/2006) awarded to Kang Sim. The au-
560thors thank the National University of Singapore for supporting the Cognitive Engineering
561Group at the Singapore Institute for Neurotechnology (SINAPSE) under grant number R-
562719-001-102-232. The sponsors of the study had no role in study design, data collection,
563data analysis, results interpretation, writing the paper, and the decision to submit the
564paper for publication.
565Contributors
566Kang Sim conceived, designed and performed the experiments. Yu Sun., Renick Lee,
567and Yu Chen undertook the data analysis, performed the statistical analysis and literature
568search. Yu Sun., Anastasios Bezerianos, Simon Collinson, and Kang Sim interpreted the re-
569sults and wrote the first draft of the manuscript. All authors contributed and approved the
570final manuscript for publication. Kang Sim had full access to all of the data in the study.
571Conflict of interest
572All authors have reported no known biomedical financial interests or other potential
573conflicts of interest. All the grant and financial support as well as technical support has
574been listed.
575Acknowledgements
576This work was supported by the National Healthcare Group (NHG 11003 & NHG
57712003) awarded to Kang Sim, the Agency for Science, Technology, Research/Singapore
578BioImaging Consortium (ASTART/SBIC009/2006) awarded to Kang Sim. The authors
579thank the National University of Singapore for supporting the Cognitive Engineering
580Group at the Singapore Institute for Neurotechnology (SINAPSE) under grant number R-
581719-001-102-232. The authors are very grateful to Dr. Chan Yiong Huak for his insightful
582advices in relation to the statistical aspects of this work. The authors would also like to
583thank all patients and controls for their participation.
584Appendix A. Supplementary data
585Supplementary data to this article can be found online at http://dx.
586doi.org/10.1016/j.schres.2016.01.025.
587References
588Abdul-Rahman, M.F., Qiu, A., Sim, K., 2011. Regionally specific white matter disruptions of
589fornix and cingulum in schizophrenia. PLoS One 6 (4), e18652.
590Albert, M.L., Knoefel, J.E., 2011. Clinical Neurology of Aging. Oxford University Press.
591Andreasen, N.C., Nopoulos, P., Magnotta, V., Pierson, R., Ziebell, S., Ho, B.C., 2011. Progres-
592sive brain change in schizophrenia: a prospective longitudinal study of first-episode
593schizophrenia. Biol. Psychiatry 70 (7), 672–679.
594Asami, T., Bouix, S., Whitford, T.J., Shenton, M.E., Salisbury, D.F., McCarley, R.W., 2012. Lon-
595gitudinal loss of gray matter volume in patients with first-episode schizophrenia:
596DARTEL automated analysis and ROI validation. NeuroImage 59 (2), 986–996.
7Y. Sun et al. / Schizophrenia Research xxx (2015) xxx–xxx
Please cite this article as: Sun, Y., et al., Disruption of brain anatomical networks in schizophrenia: A longitudinal, diffusion tensor imaging based
study, Schizophr. Res. (2015), http://dx.doi.org/10.1016/j.schres.2016.01.025
10. U
N
C
O
R
R
E
C
T
E
D
P
R
O
O
F
597 Bassett, D.S., Bullmore, E., Verchinski, B.A., Mattay, V.S., Weinberger, D.R., Meyer-
598 Lindenberg, A., 2008. Hierarchical organization of human cortical networks in health
599 and schizophrenia. J. Neurosci. 28 (37), 9239–9248.
600 Beaulieu, C., 2002. The basis of anisotropic water diffusion in the nervous system — a
601 technical review. NMR Biomed. 15 (7-8), 435–455.
602 Betzel, R.F., Byrge, L., He, Y., Goni, J., Zuo, X.N., Sporns, O., 2014. Changes in structural and
603 functional connectivity among resting-state networks across the human lifespan.
604 NeuroImage 102, 345–357.
605 Boccaletti, S., Latora, V., Moreno, Y., Chavez, M., Hwang, D.-U., 2006. Complex networks:
606 structure and dynamics. Phys. Rep. 424 (4), 175–308.
607 Buchanan, C.R., Pernet, C.R., Gorgolewski, K.J., Storkey, A.J., Bastin, M.E., 2014. Test-retest
608 reliability of structural brain networks from diffusion MRI. NeuroImage 86, 231–243.
609 Bullmore, E., Sporns, O., 2009. Complex brain networks: graph theoretical analysis of
610 structural and functional systems. Nat. Rev. Neurosci. 10 (3), 186–198.
611 Collinson, S.L., Gan, S.C., Woon, P.S., Kuswanto, C., Sum, M.Y., Yang, G.L., Lui, J.M., Sitoh,
612 Y.Y., Nowinski, W.L., Sim, K., 2014. Corpus callosum morphology in first-episode
613 and chronic schizophrenia: combined magnetic resonance and diffusion tensor imag-
614 ing study of Chinese Singaporean patients. Br. J. Psychiatry 204 (1), 55–60.
615 Crossley, N.A., Mechelli, A., Scott, J., Carletti, F., Fox, P.T., McGuire, P., Bullmore, E.T., 2014.
616 The hubs of the human connectome are generally implicated in the anatomy of brain
617 disorders. Brain 137 (Pt 8), 2382–2395.
618 Cui, Z., Zhong, S., Xu, P., He, Y., Gong, G., 2013. PANDA: a pipeline toolbox for analyzing
619 brain diffusion images. Front. Hum. Neurosci. 7, 42.
620 Dennis, E.L., Jahanshad, N., McMahon, K.L., de Zubicaray, G.I., Martin, N.G., Hickie, I.B.,
621 Toga, A.W., Wright, M.J., Thompson, P.M., 2013. Development of brain structural con-
622 nectivity between ages 12 and 30: a 4-Tesla diffusion imaging study in 439 adoles-
623 cents and adults. NeuroImage 64, 671–684.
624 Douaud, G., Smith, S., Jenkinson, M., Behrens, T., Johansen-Berg, H., Vickers, J., James, S.,
625 Voets, N., Watkins, K., Matthews, P.M., James, A., 2007. Anatomically related grey
626 and white matter abnormalities in adolescent-onset schizophrenia. Brain 130 (Pt
627 9), 2375–2386.
628 Ellison-Wright, I., Bullmore, E., 2010. Anatomy of bipolar disorder and schizophrenia: a
629 meta-analysis. Schizophr. Res. 117 (1), 1–12.
630 Fitzsimmons, J., Kubicki, M., Shenton, M.E., 2013. Review of functional and anatomical
631 brain connectivity findings in schizophrenia. Curr. Opin. Psychiatry 26 (2), 172–187.
632 Fornito, A., Zalesky, A., Bullmore, E.T., 2010. Network scaling effects in graph analytic stud-
633 ies of human resting-state FMRI data. Front. Syst. Neurosci. 4, 22.
634 Fornito, A., Zalesky, A., Pantelis, C., Bullmore, E.T., 2012. Schizophrenia, neuroimaging and
635 connectomics. NeuroImage 62 (4), 2296–2314.
636 Friston, K.J., 1998. The disconnection hypothesis. Schizophr. Res. 30 (2), 115–125.
637 Gong, G., He, Y., Concha, L., Lebel, C., Gross, D.W., Evans, A.C., Beaulieu, C., 2009a. Mapping
638 anatomical connectivity patterns of human cerebral cortex using in vivo diffusion
639 tensor imaging tractography. Cereb. Cortex 19 (3), 524–536.
640 Gong, G., Rosa-Neto, P., Carbonell, F., Chen, Z.J., He, Y., Evans, A.C., 2009b. Age- and
641 gender-related differences in the cortical anatomical network. J. Neurosci. 29 (50),
642 15684–15693.
643 Griffa, A., Baumann, P.S., Thiran, J.P., Hagmann, P., 2013. Structural connectomics in brain
644 diseases. NeuroImage 80, 515–526.
645 Hagmann, P., Kurant, M., Gigandet, X., Thiran, P., Wedeen, V.J., Meuli, R., Thiran, J.P., 2007.
646 Mapping human whole-brain structural networks with diffusion MRI. PLoS One 2 (7),
647 e597.
648 Hagmann, P., Cammoun, L., Gigandet, X., Meuli, R., Honey, C.J., Wedeen, V.J., Sporns, O.,
649 2008. Mapping the structural core of human cerebral cortex. PLoS Biol. 6 (7), e159.
650 He, Y., Chen, Z.J., Evans, A.C., 2007. Small-world anatomical networks in the human brain
651 revealed by cortical thickness from MRI. Cereb. Cortex 17 (10), 2407–2419.
652 Howes, O.D., Murray, R.M., 2014. Schizophrenia: an integrated sociodevelopmental-
653 cognitive model. Lancet 383 (9929), 1677–1687.
654 Iturria-Medina, Y., Sotero, R.C., Canales-Rodriguez, E.J., Aleman-Gomez, Y., Melie-Garcia,
655 L., 2008. Studying the human brain anatomical network via diffusion-weighted MRI
656 and Graph Theory. NeuroImage 40 (3), 1064–1076.
657 Jones, D.K., Knosche, T.R., Turner, R., 2013. White matter integrity, fiber count, and other
658 fallacies: the do's and don'ts of diffusion MRI. NeuroImage 73, 239–254.
659 Kanaan, R., Barker, G., Brammer, M., Giampietro, V., Shergill, S., Woolley, J., Picchioni, M.,
660 Toulopoulou, T., McGuire, P., 2009. White matter microstructure in schizophrenia: ef-
661 fects of disorder, duration and medication. Br. J. Psychiatry 194 (3), 236–242.
662 Kay, S.R., Fiszbein, A., Opler, L.A., 1987. The positive and negative syndrome scale (PANSS)
663 for schizophrenia. Schizophr. Bull. 13 (2), 261–276.
664 Konrad, A., Winterer, G., 2008. Disturbed structural connectivity in schizophrenia primary
665 factor in pathology or epiphenomenon? Schizophr. Bull. 34 (1), 72–92.
666 Kuswanto, C.N., Teh, I., Lee, T.S., Sim, K., 2012. Diffusion tensor imaging findings of white
667 matter changes in first episode schizophrenia: a systematic review. Clin.
668 Psychopharmacol. Neurosci. 10 (1), 13–24.
669 Kyriakopoulos, M., Frangou, S., 2009. Recent diffusion tensor imaging findings in early
670 stages of schizophrenia. Curr. Opin. Psychiatry 22 (2), 168–176.
671 Leemans, A., Jones, D.K., 2009. The B-matrix must be rotated when correcting for subject
672 motion in DTI data. Magn. Reson. Med. 61 (6), 1336–1349.
673 Li, Y., Liu, Y., Li, J., Qin, W., Li, K., Yu, C., Jiang, T., 2009. Brain anatomical network and in-
674 telligence. PLoS Comput. Biol. 5 (5), e1000395.
675 Liu, Y., Liang, M., Zhou, Y., He, Y., Hao, Y., Song, M., Yu, C., Liu, H., Liu, Z., Jiang, T., 2008.
676 Disrupted small-world networks in schizophrenia. Brain 131 (Pt 4), 945–961.
677 Lo, C.Y., Wang, P.N., Chou, K.H., Wang, J., He, Y., Lin, C.P., 2010. Diffusion tensor
678 tractography reveals abnormal topological organization in structural cortical net-
679 works in Alzheimer's disease. J. Neurosci. 30 (50), 16876–16885.
680 McDonald, C., Marshall, N., Sham, P.C., Bullmore, E.T., Schulze, K., Chapple, B., Bramon, E.,
681 Filbey, F., Quraishi, S., Walshe, M., Murray, R.M., 2006. Regional brain morphometry in
682patients with schizophrenia or bipolar disorder and their unaffected relatives. Am.
683J. Psychiatry 163 (3), 478–487.
684Meyer-Lindenberg, A., Weinberger, D.R., 2006. Intermediate phenotypes and genetic
685mechanisms of psychiatric disorders. Nat. Rev. Neurosci. 7 (10), 818–827.
686Micheloyannis, S., Pachou, E., Stam, C.J., Breakspear, M., Bitsios, P., Vourkas, M., Erimaki, S.,
687Zervakis, M., 2006. Small-world networks and disturbed functional connectivity in
688schizophrenia. Schizophr. Res. 87 (1-3), 60–66.
689Mori, S., Crain, B.J., Chacko, V.P., van Zijl, P.C., 1999. Three-dimensional tracking of axonal
690projections in the brain by magnetic resonance imaging. Ann. Neurol. 45 (2),
691265–269.
692Navari, S., Dazzan, P., 2009. Do antipsychotic drugs affect brain structure? A systematic
693and critical review of MRI findings. Psychol. Med. 39 (11), 1763–1777.
694Olabi, B., Ellison-Wright, I., McIntosh, A.M., Wood, S.J., Bullmore, E., Lawrie, S.M., 2011. Are
695there progressive brain changes in schizophrenia? A meta-analysis of structural mag-
696netic resonance imaging studies. Biol. Psychiatry 70 (1), 88–96.
697Ottet, M.C., Schaer, M., Debbane, M., Cammoun, L., Thiran, J.P., Eliez, S., 2013. Graph theory
698reveals dysconnected hubs in 22q11DS and altered nodal efficiency in patients with
699hallucinations. Front. Hum. Neurosci. 7, 402.
700Park, D.C., Reuter-Lorenz, P., 2009. The adaptive brain: aging and neurocognitive scaffold-
701ing. Annu. Rev. Psychol. 60, 173–196.
702Pettersson-Yeo, W., Allen, P., Benetti, S., McGuire, P., Mechelli, A., 2011. Dysconnectivity in
703schizophrenia: where are we now? Neurosci. Biobehav. Rev. 35 (5), 1110–1124.
704Pfefferbaum, A., Rohlfing, T., Rosenbloom, M.J., Chu, W., Colrain, I.M., Sullivan, E.V., 2013.
705Variation in longitudinal trajectories of regional brain volumes of healthy men and
706women (ages 10 to 85 years) measured with atlas-based parcellation of MRI.
707NeuroImage 65, 176–193.
708Rubinov, M., Bullmore, E., 2013. Schizophrenia and abnormal brain network hubs. Dia-
709logues Clin. Neurosci. 15 (3), 339–349.
710Rubinov, M., Sporns, O., 2010. Complex network measures of brain connectivity: uses and
711interpretations. NeuroImage 52 (3), 1059–1069.
712Rubinov, M., Knock, S.A., Stam, C.J., Micheloyannis, S., Harris, A.W., Williams, L.M.,
713Breakspear, M., 2009. Small-world properties of nonlinear brain activity in schizo-
714phrenia. Hum. Brain Mapp. 30 (2), 403–416.
715Smith, S.M., Jenkinson, M., Woolrich, M.W., Beckmann, C.F., Behrens, T.E., Johansen-Berg,
716H., Bannister, P.R., De Luca, M., Drobnjak, I., Flitney, D.E., Niazy, R.K., Saunders, J.,
717Vickers, J., Zhang, Y., De Stefano, N., Brady, J.M., Matthews, P.M., 2004. Advances in
718functional and structural MR image analysis and implementation as FSL. NeuroImage
71923 (Suppl. 1), S208–S219.
720Sporns, O., 2011. The human connectome: a complex network. Ann. N. Y. Acad. Sci. 1224,
721109–125.
722Sporns, O., Zwi, J.D., 2004. The small world of the cerebral cortex. Neuroinformatics 2 (2),
723145–162.
724Stone, M.H., Jastak, S., Wilkinson, G., 1995. Wide Range Achievement Test (WRAT-3).
725Rasch Meas. Trans. 403.
726Sun, Y., Chen, Y., Collinson, S.L., Bezerianos, A., Sim, K., 2015. Reduced hemispheric asym-
727metry of brain anatomical networks is linked to schizophrenia: a connectome study.
728Cereb. Cortex [Epub ahead of print].
729Szeszko, P.R., Ardekani, B.A., Ashtari, M., Kumra, S., Robinson, D.G., Sevy, S., Gunduz-Bruce,
730H., Malhotra, A.K., Kane, J.M., Bilder, R.M., Lim, K.O., 2005. White matter abnormalities
731in first-episode schizophrenia or schizoaffective disorder: a diffusion tensor imaging
732study. Am. J. Psychiatry 162 (3), 602–605.
733Tuch, D.S., Wedeen, V.J., Dale, A.M., George, J.S., Belliveau, J.W., 2001. Conductivity tensor
734mapping of the human brain using diffusion tensor MRI. Proc. Natl. Acad. Sci. U. S. A.
73598 (20), 11697–11701.
736Tzourio-Mazoyer, N., Landeau, B., Papathanassiou, D., Crivello, F., Etard, O., Delcroix, N.,
737Mazoyer, B., Joliot, M., 2002. Automated anatomical labeling of activations in SPM
738using a macroscopic anatomical parcellation of the MNI MRI single-subject brain.
739NeuroImage 15 (1), 273–289.
740Uhlhaas, P.J., 2013. Dysconnectivity, large-scale networks and neuronal dynamics in
741schizophrenia. Curr. Opin. Neurobiol. 23 (2), 283–290.
742van den Heuvel, M.P., Fornito, A., 2014. Brain networks in schizophrenia. Neuropsychol.
743Rev. 24 (1), 32–48.
744van den Heuvel, M.P., Mandl, R.C., Stam, C.J., Kahn, R.S., Hulshoff Pol, H.E., 2010. Aberrant
745frontal and temporal complex network structure in schizophrenia: a graph theoreti-
746cal analysis. J. Neurosci. 30 (47), 15915–15926.
747van den Heuvel, M.P., Sporns, O., Collin, G., Scheewe, T., Mandl, R.C., Cahn, W., Goni, J.,
748Hulshoff Pol, H.E., Kahn, R.S., 2013. Abnormal rich club organization and functional
749brain dynamics in schizophrenia. JAMA psychiatry 70 (8), 783–792.
750Wang, R., Benner, T., Sorensen, A., Wedeen, V., 2007. Diffusion toolkit: a software package
751for diffusion imaging data processing and tractography. Proc. Intl. Soc. Mag. Reson.
752Med., p. 3720
753Wang, Q., Su, T.P., Zhou, Y., Chou, K.H., Chen, I.Y., Jiang, T., Lin, C.P., 2012. Anatomical in-
754sights into disrupted small-world networks in schizophrenia. NeuroImage 59 (2),
7551085–1093.
756Whitford, T.J., Grieve, S.M., Farrow, T.F., Gomes, L., Brennan, J., Harris, A.W., Gordon, E.,
757Williams, L.M., 2007. Volumetric white matter abnormalities in first-episode schizo-
758phrenia: a longitudinal, tensor-based morphometry study. Am. J. Psychiatry 164
759(7), 1082–1089.
760Woods, S.W., 2003. Chlorpromazine equivalent doses for the newer atypical antipsy-
761chotics. J. Clin. Psychiatry 64 (6), 663–667.
762Wu, K., Taki, Y., Sato, K., Kinomura, S., Goto, R., Okada, K., Kawashima, R., He, Y., Evans,
763A.C., Fukuda, H., 2012. Age-related changes in topological organization of structural
764brain networks in healthy individuals. Hum. Brain Mapp. 33 (3), 552–568.
765Wu, K., Taki, Y., Sato, K., Qi, H., Kawashima, R., Fukuda, H., 2013. A longitudinal study of
766structural brain network changes with normal aging. Front. Hum. Neurosci. 7, 113.
8 Y. Sun et al. / Schizophrenia Research xxx (2015) xxx–xxx
Please cite this article as: Sun, Y., et al., Disruption of brain anatomical networks in schizophrenia: A longitudinal, diffusion tensor imaging based
study, Schizophr. Res. (2015), http://dx.doi.org/10.1016/j.schres.2016.01.025
11. U
N
C
O
R
R
E
C
T
E
D
P
R
O
O
F
767 Wylie, K.P., Tregellas, J.R., 2010. The role of the insula in schizophrenia. Schizophr. Res.
768 123 (2-3), 93–104.
769 Xia, M., Wang, J., He, Y., 2013. BrainNet Viewer: a network visualization tool for human
770 brain connectomics. PLoS One 8 (7), e68910.
771 Zalesky, A., Fornito, A., Harding, I.H., Cocchi, L., Yucel, M., Pantelis, C., Bullmore, E.T., 2010.
772 Whole-brain anatomical networks: does the choice of nodes matter? NeuroImage 50
773 (3), 970–983.
774 Zalesky, A., Fornito, A., Seal, M.L., Cocchi, L., Westin, C.F., Bullmore, E.T., Egan, G.F., Pantelis,
775 C., 2011. Disrupted axonal fiber connectivity in schizophrenia. Biol. Psychiatry 69 (1),
776 80–89.
777Zeger, S.L., Liang, K.Y., Albert, P.S., 1988. Models for longitudinal data: a generalized esti-
778mating equation approach. Biometrics 44 (4), 1049–1060.
779Zhang, Y., Lin, L., Lin, C.P., Zhou, Y., Chou, K.H., Lo, C.Y., Su, T.P., Jiang, T., 2012. Abnormal
780topological organization of structural brain networks in schizophrenia. Schizophr.
781Res. 141 (2-3), 109–118.
782
9Y. Sun et al. / Schizophrenia Research xxx (2015) xxx–xxx
Please cite this article as: Sun, Y., et al., Disruption of brain anatomical networks in schizophrenia: A longitudinal, diffusion tensor imaging based
study, Schizophr. Res. (2015), http://dx.doi.org/10.1016/j.schres.2016.01.025
View publication statsView publication stats