
Empfohlen
Weitere ähnliche Inhalte
Was ist angesagt?
Was ist angesagt? (20)
Ähnlich wie Basic airway management
Ähnlich wie Basic airway management (20)
Kürzlich hochgeladen
Kürzlich hochgeladen (20)
Basic airway management
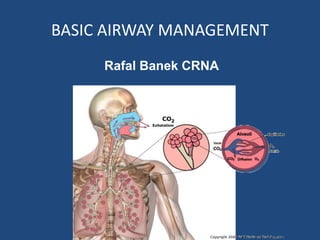
- 1. BASIC AIRWAY MANAGEMENT Rafal Banek CRNA
- 2. Learning Objectives ● Anatomy of the airway and respiratory system ● Fundamentals of Airway Management ● Familiarity with airway adjuncts
- 3. IF YOU CAN’T BREATH, NOTHING ELSE MATTERS !!! ● Airway management is one of the most critical aspect of trauma care. ● Airway compromise may quickly result in fatality yet, it may be easy to treat ● Unrecognized airway compromise may lead to patient deterioration and death within minutes. ● No trauma interventions should be undertaken before addressing the airway status……….ANY EXCEPTIONS TO THIS ?
- 4. AIRWAY ANATOMY TWO MAJOR COMPONENTS 1.Upper airway Humidification, filtration and warming of the inhaled air Filtration of bacteria (Tonsils/Adenoids) Phonation 2.Lower airway Exchange of O2, CO2 with blood Phonation
- 5. UPPER AIRWAY 1. Nasal cavity Warms, filters, humidifies air 2. Nasopharynx From the internal nostrils to lower edge of soft palate 3. Oral cavity, 4. Oropharynx Soft palate to epiglottis 5. Laryngopharynx (hypopharynx) From epiglottis to cricoid cartilage Nasal Cavity Oral Cavity Oral cavity
- 6. LOWER AIRWAY 1. Trachea 2. Bronchi Two mainstem Secondary, tertiary 3. Bronchioles 4. Alveolar ducts 5. Alveolar sacs 4. Alveoli “Balloon-like” clusters Actual sites of gas exchange Carina
- 7. Basic Airway Techniques • Everyone involved in trauma care should be familiar with and proficient in their use • These should be executed before advanced airway management is undertaken 1. Head tilt/chin lift 2. Jaw thrust (known or suspected c-spine injury) 3. Nasopharyngeal airway 4. Oropharyngeal airway 5. Bag valve mask assist or PPV
- 8. Key points to remember during initial airway evaluation Airway is patent if the victim is able to speak Muscular tone of the head and neck muscles keeps the airway open in awake conscious patient As LOC decreases, the airway muscle tone decreases leading to partial or complete obstruction The tongue is the most common cause of airway obstruction in an unconscious adult. Unconscious victim’s respirations may be sufficient to maintain life but death may result from airway obstruction Patients with head, face, neck, chest and inhalational injury have higher likelihood of airway compromise
- 10. Airway obstruction in unconscious victim Obstruction
- 11. Types of airway obstruction Partial Snoring Stridor Abnormal phonation Paradoxical motion of the abdominal and chest walls Complete Absent air movement Aphonia Rapidly ensuing hypoxia Paradoxical motion may continue
- 12. Airway Evaluation • If patient is conscious and speaking normally-provide supplemental 02, assess BS, continue close monitoring • If patient is unconscious Head tilt/chin lift or forward thrust the mandible if known or suspected c-spine trauma If facial trauma present, may need to inspect the mouth for blood, bone fragments and other foreign objects- remove or suction if necessary Look for chest movement, assess for exhaled air Consider placing simple airway adjunct to maintain the airway patency
- 13. Head tilt/chin lift Jaw thrust • One hand on forehead • Second grasping the bony portion of mandible • Avoid pressing on the soft tissue !!! • Tilt the head and lift the chin at the same time. • This lifts the tongue and creates a pocket for oxygen to travel. • Assess for air movement
- 14. Jaw thrust • Safest maneuver if c-spine injury is suspected • Avoids c-spine extension • Stand behind the patient • Heels of the hands on the temporal areas • Locate angle of the mandible • Displace jaw forward while maintaining neutral head position • Reassess for air movement
- 15. Nasopharyngeal Airway (NPA) • Better tolerated in semi- conscious patient with intact airway reflexes • Properly sized from NPA extends from the nostril to the angle of the mandible • Do not use with facial trauma or suspected skull fracture • Epistaxis not uncommon from NPA use (coagulopathic patients???)
- 16. NPA insertion • Lubricate-KY or Lidocaine jelly • Perpendicular to the face • Twisting motion • Avoid forcing in the device • Once placed, reassess the airway patency
- 17. Oropharyngeal airway (OPA) • Do not use in semiconscious patient with intact airway reflexes (vomiting, aspiration, laryngospasm !!!) •Properly sized from OPA extends from the mouth to the angle of the mandible
- 18. OPA insertion •Begin inserting from the inverted position •When advancing, gently rotate the device 180 degrees •Tongue blade may be used to aid the passage of the OPA •Reassess airway patency
- 19. Oxygenation and ventilation must be reassessed after airway patency has been re-established Indicators of inadequate ventilation and oxygenation Central cyanosis Rapid shallow respirations Accessory muscle use Retractions Abdominal paradoxical respirations SpO2<90%
- 20. Bag-Valve mask (BVM) ventilation (“bagging”) • Critically important airway skill • Always the first response to inadequate oxygenation and ventilation • The first “bail-out” maneuver to a failed intubation attempt • Attenuates the urgency to intubate
- 21. Golden Rules of “Bagging” • Almost anybody can be oxygenated and ventilated with a bag and a mask • Manual ventilation skill with proper equipment is a fundamental premise of basic and advanced airway management • The art of bagging should be mastered before the learning advanced airway skills
- 22. BVM Ventilation • Requires practice to master • One hand to – maintain face seal – position head – maintain patency • Sniffing position if c-spine clear • Thumb + index to maintain face seal • Middle finger under mandibular symphysis • Ring/little finger under angle of mandible • Other hand ventilates ALL fingers rest on the bony portion of the mandible
- 23. “Bagging” with C-spine precautions • Two person maneuver • Primary maintains the seal and neutral head postition • Assistant provides jaw thrust • NPA or OPA may be helpful
- 24. Predictors of difficult “bagging” •Upper airway obstruction •Lack of dentures •Beard •Midfacial trauma •Facial burns, dressings, scarring •Poor lung mechanics-resistance or compliance
- 25. Algorithm for difficulty “Bagging” • Reassess for blood, fractured teeth and foreign bodies –suction or remove if applicable • Triple maneuver if c-spine clear – Head tilt, jaw thrust, mouth opening • Nasal or/and oropharyngeal airways • Two-person, four-hand technique
- 26. Two-person, four-hand technique OPA and 2 NPA’s in place Two hands on the mask and face for optimal seal/position Two hands on the bag to ventilate
- 27. Excessive gastric distention from “bagging” • Possible consequences Gastric contnents regurgitation and aspiration Restricted diaphragmatic movement In rare cases gastric rupture • Minimizing the risks Minimize the duration of “bagging” Avoid excessive tidal volumes Minimize the positive pressure (<20 cm H2O) if possible Consider cricoid pressure Decompress the stomach with NGT or OGT after the airway is secured
- 28. What if “bagging” is difficult or impossible???? • Rescue devices Laryngeal Mask Airway (LMA) Combitube
- 29. LMA • Can be inserted blindly by unskilled personnel • Creates seal around the laryngeal inlet, enabling ventilation from immediately above the cords, • Bypasses proximal upper airway obstruction- mostly tongue • >90% rescue success rate in impossible or difficult face mask ventilation situations
- 30. LMA placement 1. Lubricate posterior part of the cuff 2. Place the tip behind pt’s upper teeth 3. Place the finger in pt’s mouth, while advancing push your finger against the palate and forward against the cuff 4. Continue advancing till resistant is felt 5. Inflate the cuff 6. Attach the bag and watch for the chest movement after each manual breath
- 31. Combitube • Inserted blindly • Easy to use by the unskilled rescuers • Esophageal placement is most likely (90% of the insertions) • Easy to use by the unskilled rescuers • Provides better esophageal seal than LMA • Success rate 75-100% in pre- hospital setting
- 32. Combitube insertion • Head tilt (clear C-spine?) with lower jaw lift • Advance gently with other hand trying to follow curvature of the tongue, until transverse lines are adjacent to the teeth • If this is emergency airway, inflate both lumens •
- 33. Combitube insertion • Inflate proximal cuff (#1) first (80-10mL) then distal (5-15mL) • Attempt ventilation via #1, assess for CO2, BS, chest movement • If no CO2 return and no breathsounds are present from #1 endotracheal placement has occurred, switch to #2 and ventilate • Congratulations!!!, you have just placed ETT, may deflate cuff #1 >90% placements <10% placements #1 #2
- 34. Combitube troubleshooting • If ventilations are ineffective, through either lumen, the tube is to deep in esophagus • Withdraw at 1cm increments • Reassess BS, CO2, chest movement as you withdraw
- 35. Exhaled CO2 (ETCO2)monitoring • Golden standard to ascertain patent airway and correct placement of advance airway device • 2 types of monitors Capnograph – bedside monitoring “Easy cap”-Responds quickly to exhaled CO2 with a simple color change, breath-to-breath response, highly portable, What color if CO2 is present? • Golden standard to ascertain patent airway and correct placement of advance airway device • 2 types of monitors Capnograph – bedside monitoring “Easy cap”-Responds quickly to exhaled CO2 with a simple color change, breath-to-breath response, highly portable,
- 36. Key points • Airway compromise can be quickly fatal but in most cases is easy to correct • Tongue is the most frequent cause of airway obstruction • In the absence of severe extremity hemorrhage, airway is evaluated and treated first, regardless of severity of other injuries • Bag-valve mask ventilation is the most critical airway management skill set, the first responders must learn • ETCO2 monitoring is the golden standard for ascertaining the airway patency
- 37. References 1. Kovacs G, Law JA. Airway Management in Emergencies. McGraw Hill Medical; 2008:33-51
- 38. ??????????????
Hinweis der Redaktion
- Basic airway management is the most critical skill for anyone who deals with the trauma victim Untreated airway obstruction will result in death from cerebral anoxia within several minutes. Fortunately, most causes of airway obstruction can easily be reversed. In the absence of visible massive hemorrhage at the point of injury, the airway status evaluation and treatment should be the first action undertaken. We all remember MARCH (massive hemorrhage, airway, respirations, circulation, head trauma) from the CLS class.
- Airway has 2 major divisions, lower and upper airway Upper airway warms humidifies purifies air and protects respiratory system from infections Lower airway effects exchange of gases Both components of the airway participate in phonation
- 1. Air enters the airway mainly through the nasal cavity and in lesser degree through the oral cavity. 3. Nasal cavity functions as the warmer, filter and humidifier of the inhaled air. 2. From oral and nasal cavities air travels through the pharynx and its three segments (nasopharynx, oropharynx, laryngopharynx) and enters the lower airway. 4. Vocal cords are considered to be the dividing structure between upper an lower airway 5. From bronchiae into our lungs. 6. Our lungs are filled with branches of alveaolar ducts and those ducts are made of many alveolar sacs. 7. These sacs are breaking down even further into alvenius. 8. Surrounding these alvenius are tiny blood vessels and capillaries This where air and blood exchanges take place and how oxygenated blood travels to the heart. 9. Finally the heart then pumps the blood throughout the body making each cells, organs, and body system function.
- Trachea bifurcates at the carina, into right and left main stem bronchi Right mainstem bronchus is shorter and straighter, left mainstem is longer and more angled Main bronchi further branch into secondary and then tertiary bronchi which then branch into bronchioles Bronchioles further brunch into alveolar ducts which terminate into alveolar sacs There are about 300 million alveoli in the adult’s respiratory system Alveoli are surrounded by a dense network of pulmonary capillaries This capillary network brings the CO2 and carries the oxygen away from the alveoli
- As mentioned in one of the first slides, airway structures have important role in phonation, so if our patient is able to talk we can rest assured that he has patent airway Muscle tone mainly the tongue are responsible for patency of the airway. If patient has altered LOC either from trauma or pharmacologic interventions, partial or complete obstruction may ensue. The tongue is the most common cause of airway obstruction in the adult patient Many unconscious victims may be able to maintain adequate spontaneous respirations but may die if airway obstruction is not relieved Several types of injuries are more likely to result in airway obstruction due to damage to the airway structures or due to developing edema. These include head, face, neck, chest and inhalational injury
- In the conscious victim the muscle tone keeps the tongue away from posterior pharyngeal wall allowing for unobstructed passage of air Red lines represent the air pathway
- As the victim becomes unconscious, the muscle tone is lost, causing the tongue and epiglottis to rest on the posterior pharyngeal wall The air passage is blocked
- There are 2 types of airway obstruction, partial and complete Partial obstruction occurs when the airflow is still present but the airway lumen is narrowed. Signs of incomplete airway obstruction include snoring, stridor, difficulty speaking and “rocking motion” of the abdomen and chest when during attempted inspiration the abdomen rises and chest falls. Partial obstruction if untreated may progress to complete airway obstruction With complete obstruction, there is no detectable airway movement, if patient is conscious he/she will be unable to speak, the rocking motion may still continue, desaturation may occur very quickly
- Victim should be in the supine position, preferably on the firm surface One hand is firmly placed on the forehead while 2 or 3 fingers of the other hand grasp bony portion of the mandible Be careful not to push against the soft structures of the chin as this may actually worsen the obstruction This maneuver should lift the tongue and relieve the obstruction To assess if airway patency has been re-established you can feel or listen for exhaled air, look for the fog in the oxygen mask, ask the second person to listen for breathsounds. If snoring was present due to partial obstruction, it should dissappear.
- Lubrication eases placement, decreases trauma from insertion, lidocaine jelly may alleviate the discomfort while the device is in place It should be oriented perpendicular to the face to follow the curvature of the floor of nasal cavity Twisting motion may make the passage easier If significant resistance is felt, withdraw device and attempt the opposite nostril Once the device is inserted, reassess the patency of the airway by feeling for exhaled air, listening for breathsounds, fog in the mask
- After the airway patency is restored we must assess patient for adequate ventilatory effort Signs of poor ventilatory effort inlclude the following Central cyanosis Rapid shallow respirations Accessory muscle use Retractions Abdominal paradoxical respirations SpO2<90%
- If the rescuer is not satisfied with patient’s spontaneous ventilations, BVM must be used to assist the patient or to deliver positive pressure ventilations until advanced airway device is placed
- This slide demonstrates E-C technique for proper manual ventilation The middle, ring and little finger rest on the bony portions of the mandible. We must be careful to avoid pressing on soft tissues of the mandible as this may obstruct the airway
- These factors may cause difficulties with adequate BVM venilation
- The photo on the left represents classic double E-C grip In the photo on the right, jaw thrust is attempted to further improve air passage
- During the positive pressure ventilation some of the air will unavoidably be forced into the stomach. If the gastric insufflation is excessive, various complications may occur. These include regurgitation of gastric contents and pulmonary aspiration, Overinflation of the stomach may restrict diaphragmatic expansion further increasing difficulty with ventilation. In some extreme cases gastric rupture may occur To minimize the complications from gastric insufflation we should minimize the duration of bagging if advanced airway is planned and skilled personnel available, further lowest possible volume and pressure should be used to deliver the each breath. Cricoid pressure application may be helpful in minimizing entry of air into the stomach. As soon as the airway is secured gastric tube should be placed to decompress the stomach
- When properly seated in the pharynx, the inflated cuff forms a seal around the laryngeal inlet, enabling ventilation from immediately above the cords,
- As earlier mentioned, over 90% of the time the distal lumen will end up in esophagus and less than 10% in the trachea After placement to the correct land mark inflate cuff #1 then #2 Since most placements are esophageal, attempt ventilations via #1 and assess for placement If ventilations through lumen #1 are ineffective, distal lumen is in the trachea switch to #2 and ventilate In this situation, combitube will function as the regular ETT