New Horizons for Advanced Endometrial Cancer Treatment: Utilizing Innovative Immunotherapies and Other Novel Approaches
•
0 gefällt mir•101 views

Chair, Shannon N. Westin, MD, MPH, prepared useful Practice Aids pertaining to endometrial cancer for this CME/MOC/NCPD activity titled “New Horizons for Advanced Endometrial Cancer Treatment: Utilizing Innovative Immunotherapies and Other Novel Approaches.” For the full presentation, downloadable Practice Aids, and complete CME/MOC/NCPD information, and to apply for credit, please visit us at https://bit.ly/3ecJ3Tk. CME/MOC/NCPD credit will be available until February 6, 2024.

Empfohlen
Empfohlen
Weitere ähnliche Inhalte
Ähnlich wie New Horizons for Advanced Endometrial Cancer Treatment: Utilizing Innovative Immunotherapies and Other Novel Approaches
Ähnlich wie New Horizons for Advanced Endometrial Cancer Treatment: Utilizing Innovative Immunotherapies and Other Novel Approaches (13)
Mehr von PVI, PeerView Institute for Medical Education
Mehr von PVI, PeerView Institute for Medical Education (20)
Kürzlich hochgeladen
Kürzlich hochgeladen (20)
New Horizons for Advanced Endometrial Cancer Treatment: Utilizing Innovative Immunotherapies and Other Novel Approaches
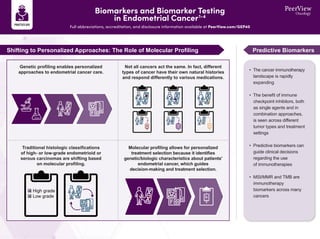
- 1. Shifting to Personalized Approaches: The Role of Molecular Profiling Predictive Biomarkers Genetic profiling enables personalized approaches to endometrial cancer care. Not all cancers act the same. In fact, different types of cancer have their own natural histories and respond differently to various medications. Traditional histologic classifications of high- or low-grade endometrioid or serous carcinomas are shifting based on molecular profiling. Molecular profiling allows for personalized treatment selection because it identifies genetic/biologic characteristics about patients' endometrial cancer, which guides decision-making and treatment selection. High grade Low grade • The cancer immunotherapy landscape is rapidly expanding • The benefit of immune checkpoint inhibitors, both as single agents and in combination approaches, is seen across different tumor types and treatment settings • Predictive biomarkers can guide clinical decisions regarding the use of immunotherapies • MSI/MMR and TMB are immunotherapy biomarkers across many cancers Biomarkers and Biomarker Testing in Endometrial Cancer1-4 Full abbreviations, accreditation, and disclosure information available at PeerView.com/GEP40
- 2. MSI-H and dMMR are considered the same population biologically—both groups of patients can be treated with the same agents • dMMR/MSI-H refers to a group of patients with mismatch repair deficiency • MMRp/MSS refers to a group of patients who are mismatch repair proficient Microsatellite Instability (MSI) MSI is detected through molecular testing Consensus definition: MSI is a condition of genetic hypermutability Characterized by the clustering of mutations in microsatellites typically consisting of repeat length alterations The presence of MSI represents evidence that MMR is not functioning normally, or dMMR MSI-H provides the phenotypic evidence of dMMR Mismatch Repair (MMR) MMR proteins are detected by IHC stain MMR protein complexes (MLH1 + PMS2 and MSH2 + MSH6) detect and correct mistakes during DNA replication Absence or loss of function of one of the four MMR proteins results in MMR deficiency, or dMMR dMMR is the cause of MSI-high, or MSI-H Biomarkers and Biomarker Testing in Endometrial Cancer1-4 Full abbreviations, accreditation, and disclosure information available at PeerView.com/GEP40 1. Kloor M et al. Trends Cancer. 2016;2:121-133. 2. Luchini C et al. Ann Oncol. 2019; 30:1232-1243. 3. Hause RJ et al. Nat Med. 2016;22:1342-1350. 4. Levine DA. Nature. 2013;497:67.
- 3. Managing Immune-Related Adverse Events1-4 Full abbreviations, accreditation, and disclosure information available at PeerView.com/GEP40 Safety Considerations for Immunotherapies 1. Monitor closely for potential irAEs by evaluating blood work including liver enzymes, creatinine, and thyroid function 2. Ask patients about symptoms such as cough, shortness of breath, and diarrhea, which may be signs of pneumonitis or colitis 3. Stay in communication with patients to help mitigate and treat more common AEs such as fatigue, nausea, and anemia Pancreatitis, autoimmune diabetes Colitis Enteritis Encephalitis, aseptic meningitis Thyroiditis, hypothyroidism, hyperthyroidism Dry mouth, mucositis Hypophysitis Uveitis Pneumonitis Thrombocytopenia, anemia Hepatitis Adrenal insufficiency Nephritis Vasculitis Arthralgia Neuropathy Rash, vitiligo Myocarditis Any organ system can be affected; commonly occurring irAEs are pulmonary (pneumonitis), dermatologic (rash, pruritus, blisters, ulcers, vitiligo), gastrointestinal (diarrhea, enterocolitis, transaminitis, hepatitis, pancreatitis), and endocrine (thyroiditis, hypophysitis, adrenal insufficiency) What Is the Spectrum of Potential irAEs? • In general, checkpoint inhibitor therapy should be continued with close monitoring, with the exception of some neurologic, hematologic, and cardiac toxicities Minimal or no symptoms; diagnostic changes only Grade 1 • Hold checkpoint inhibitor therapy for most grade 2 toxicities • Consider resuming immunotherapy when symptoms and/or laboratory values revert to grade 1 or lower • Corticosteroids (initial dose of 0.5-1 mg/kg/d of prednisone or equivalent) may be administered Grade 3 toxicities • Hold checkpoint inhibitor therapy • Initiate high-dose corticosteroids (prednisone 1-2 mg/kg/d or methylprednisolone IV 1-2 mg/kg/d) • If symptoms do not improve with 48-72 hours of high-dose corticosteroids, infliximab may be offered for some toxicities • Taper corticosteroids over the course of at least 4-6 weeks • When symptoms and/or laboratory values revert to grade 1 or lower, rechallenging with immunotherapy may be offered; however, caution is advised, especially in those patients with early-onset irAEs; dose adjustments are not recommended Grade 4 toxicities • In general, permanent discontinuation of checkpoint inhibitor therapy is warranted, with the exception of endocrinopathies that have been controlled by hormone replacement Grade 2 Mild to moderate symptoms Severe or life-threatening symptoms Grades 3/4 Most significant irAEs occur in less than 5% of patients irAE Grading and Managment
- 4. 1. Postow MA et al. N Engl J Med. 2018;378:158-168. 2. Brahmer JR et al. J Clin Oncol. 2018;36:1714-1768. 3. NCCN Clinical Practice Guidelines in Oncology. Management of Immunotherapy-Related Toxicities. Version 1.2022. https://www.nccn.org/professionals/physician_gls/pdf/immunotherapy.pdf. 4. https://ctep.cancer.gov/protocoldevelopment/electronic_applications/ctc.htm. 5. Makker V et al. Oncologist. 2021;26:e1599-e1608. 6. How JA et al. Gynecol Oncol. 2021;162:24-31. Managing Immune-Related Adverse Events5,6 Full abbreviations, accreditation, and disclosure information available at PeerView.com/GEP40 Consult irAE management guidelines (eg, ASCO, NCCN, SITC, ESMO) IO Pruritus Pneumonitis Myocarditis Adrenal crisis TKI Hypertension Taste changes Stomatitis Dyspepsia Cytopenia HFSR Overlapping Rash Diarrhea Hepatitis Hypothyroid AMS IO + TKI Combination Toxicities Determine which therapy is causing the AE in order to plan a management strategy Hold TKI (shorter half-life than checkpoint inhibitor) In certain cases, use appropriate supportive care If symptoms resolve in a few days, TKI was likely the cause Two mechanisms of action result in two sets of AE profiles that are not mutually exclusive PRES Encephalitis
- 5. Numerous Strategies Under Study in Advanced Endometrial Cancer Full abbreviations, accreditation, and disclosure information available at PeerView.com/GEP40 1. https://clinicaltrials.gov. 2. Daly RJ et al. Mol Cancer. 2022;21:189. 3. Bailly C et al. NAR Cancer. 2020;2(1): zcaa002. 4. Vergote IB et al. ESMO 2022. 5. Makker V et al. ASCO 2022. Abstract 5511. 6. Fung HY and Chook YM. Semin Cancer Biol. 2014;27:52-61. 7. Tai YT et al. Leukemia. 2014;28:155-165. • Immune checkpoint inhibitors work by blocking T-cell inhibitory signals, thus removing the brakes on the immune system • The combination of increased mutational load, tumor-infiltrating lymphocytes, and PD-1/PD-L1 expression makes endometrial cancer an ideal target for immunotherapeutic interventions • Exportin 1 (XPO1) is the major nuclear export protein for6 – Tumor suppressor proteins (TSPs), eg, p53, lkB, PTEN, FOXO1 • Inhibition of XPO1 results in6 – Increase in nuclear levels and activation of TSPs – Reduction of oncoprotein levels • Selinexor is an oral selective XPO1 inhibitor – Preclinical data shows reactivation of multiple TSPs (including p53 wild-type) by preventing nuclear export7 IO Monotherapy Combinations XPO1 Inhibition4,5 PD-1/PD-L1 Checkpoint Inhibition - - Without Immunotherapy With Immunotherapy MHC Antigen TCR PD-1 PD-L1 Anti– PD-L1 Anti– PD-1 Tumor cell Tumor escape Inactivation of T Cell Activation of T Cell Elimination of tumor cells • Selected trials1 – Phase 2 KEYNOTE-158 (pembrolizumab) – Phase 1 GARNET (dostarlimab) – Phase 2 PHAEDRA (durvalumab) • Selected trials1 – Phase 3 KEYNOTE-775 (pembrolizumab + lenvatanib) – Phase 3 LEAP-001 (pembrolizumab + lenvatanib) • Selected trials1 – Phase 2 SIGN – Phase 3 SIENDO – Phase 3 XPORT-EC • Angiogenesis and evasion of immune destruction are hallmarks of cancer, supporting the rationale for combining VEGFR TKI and immunotherapies targeting PD‐1/PD-L1 • Targeting TKIs may promote an immune- permissive tumor environment and enhance responses to immune checkpoint inhibitors Cell membrane Nuclear envelope Nuclear pore complex Cytoplasm Nucleus Selinexor Tumor Suppressor Proteins P53 pRb P21 IkB BRCA1 FOXO3a Oncoprotein mRNA eF4E c-Myc Bcl-6 Bcl-2 Cyclin D1 Pim1 MDM2 Glucocorticoid Receptor XPO1 IO + TKI2 IO + Chemo3 • Cytotoxic agents have immunomodulatory effects, providing a rationale for combining PD-1/PD-L1 inhibitors with chemotherapy • Chemotherapy may be synergistic in combination with immunotherapy; its ability to increase tumor immunogenicity may enhance tumor-specific T-cell activation when combined with immune checkpoint blockade • Selected trials1 – Phase 3 NRG-GY018 (pembrolizumab + chemo) – Phase 3 AtTEnd (atezolizumab + chemo) – Phase 3 RUBY (dostarlimab + chemo) – Phase 3 DUO-E (durvalumab + chemo)