How I Think, How I Treat—Assessing, Managing, and Engaging Patients to Optimize Care in SLE and LN: Comparing Approaches With the Experts
•
0 gefällt mir•16 views

Chair and Presenter, Maureen A. McMahon, MD, Maria Dall'Era, MD, and Kenneth C. Kalunian, MD, prepared useful Practice Aids pertaining to lupus for this CME/MOC activity titled “How I Think, How I Treat—Assessing, Managing, and Engaging Patients to Optimize Care in SLE and LN: Comparing Approaches With the Experts.” For the full presentation, downloadable Practice Aids, and complete CME/MOC information, and to apply for credit, please visit us at https://bit.ly/3qEJ321. CME/MOC credit will be available until December 14, 2023.

Empfohlen
Empfohlen
Weitere ähnliche Inhalte
Ähnlich wie How I Think, How I Treat—Assessing, Managing, and Engaging Patients to Optimize Care in SLE and LN: Comparing Approaches With the Experts
Ähnlich wie How I Think, How I Treat—Assessing, Managing, and Engaging Patients to Optimize Care in SLE and LN: Comparing Approaches With the Experts (20)
Mehr von PVI, PeerView Institute for Medical Education
Mehr von PVI, PeerView Institute for Medical Education (20)
Kürzlich hochgeladen
Kürzlich hochgeladen (20)
How I Think, How I Treat—Assessing, Managing, and Engaging Patients to Optimize Care in SLE and LN: Comparing Approaches With the Experts
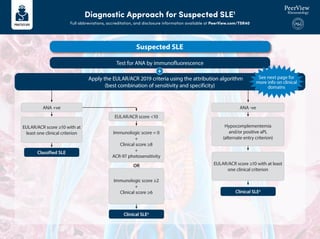
- 1. Diagnostic Approach for Suspected SLE1 Full abbreviations, accreditation, and disclosure information available at PeerView.com/TSR40 Suspected SLE Test for ANA by immunofluorescence Apply the EULAR/ACR 2019 criteria using the attribution algorithm (best combination of sensitivity and specificity) + Classified SLE Clinical SLEa Clinical SLEa Immunologic score = 0 + Clinical score ≥8 + ACR-97 photosensitivity OR See next page for more info on clinical domains ANA +ve ANA -ve EULAR/ACR score <10 EULAR/ACR score ≥10 with at least one clinical criterion Hypocomplementemia and/or positive aPL (alternate entry criterion) EULAR/ACR score ≥10 with at least one clinical criterion Immunologic score ≥2 + Clinical score ≥6
- 2. Diagnostic Approach for Suspected SLE1 Full abbreviations, accreditation, and disclosure information available at PeerView.com/TSR40 a Also consider noncriteria features (eg, Raynaud phenomenon, myocarditis, atypical rashes). 1. Fanouriakis A et al. Ann Rheum Dis. 2021;80:14-25. Clinical Domains Weight Clinical Domains Weight Fever 2 2 6 6 4 8 10 2 3 4 4 2 3 5 2 2 4 6 Pleural or pericardial effusion Hematologic Neuropsychiatric Mucocutaneous Acute pericarditis Leukopenia Thrombocytopenia Autoimmune hemolysis Delirium Psychosis Seizure Nonscarring alopecia 3 Complement proteins SLE-specific antibodies Low C3 OR low C4 4 6 Low C3 AND low C4 Anti-dsDNA OR anti-Sm antibody Oral ulcers SCLE or DLE ACLE Clinical score: 0-39 Joint involvement Proteinuria >0.5 g/24 h Renal biopsy class II or V LN Renal biopsy class III or IV LN Musculoskeletal Renal Anticardiolipin antibodies OR Anti-β2GP1 antibodies OR Lupus anticoagulant Immunologic score: 0-2 Antiphospholipid antibiodies Constitutional Immunology Domains Weight Weight Serosal Immunology Domains Within each domain, only the highest weight criterion is counted
- 3. EULAR Treatment Recommendations for SLE1 Full abbreviations, accreditation, and disclosure information available at PeerView.com/TSR40 1. Fanouriakis A et al. Ann Rheum Dis. 2021;80:14-25. First line Refractory HCG HCG GC PO/IM GC PO/IM MTX/AZA Mild First line Refractory HCG HCG GC PO/IM GC PO/IM MTX/AZA BEL CNI CNI MMF MMF Moderate First line Refractory HCG HCG GC PO/IM GC PO/IM MMF CYC CYC RTX Severe • Sun protection • Vaccinations • Exercises • No smoking • Body weight • Blood pressure • Lipids • Glucose • Antiplatelets Adjunct Target Remission Low-Disease Activity SLEDAI = 0 HCQ; no GC SLEDAI: ≤4; HCQ and prednisone ≤7.5 mg/d Immunosuppressives, in stable doses and well tolerated • Anticoagulants (in aPL-positive patients)
- 4. KDIGO 2021 Guidelines for Management of LN1 Full abbreviations, accreditation, and disclosure information available at PeerView.com/TSR40 Kidney biopsy showing class III/IV ± LN Concomitant thrombotic microangiopathy Assess activity and chronicity items Calcineurin inhibitors • Tacrolimus (trough level approximately 5.5 ng/mL [6.8 nmol/L], data mainly from Chinese patients) and reduced- dose MPAA in patients with sCr <3 mg/dL (265 mcmol/L) as initial and maintenance therapy for 24 months • Voclosporin 23.7 mg BID and MPAA in patients with eGFR >45 mL/min/1.73 m2 for 52 weeks B-lymphocyte–targeting biologics • Belimumab (IV 10 mg/kg Q2W for 3 doses then Q4W) and MPAA or IV cyclophosphamide 500 mg Q2W x 6 • Rituximab IV 1 g on days 1 and 15, as add-on therapy for refractory cases or for corticosteroids minimization MPAA for at least 6 months • MMF PO 1.0-1.5 g BID or mycophenolic acid sodium 0.72-1.08 g BID Cyclophosphamide for up to 6 months • IV 500 mg Q2W x 6 or 0.5-1.0 g/m2 monthly x 6; or PO 1.0-1.5 mg/kg/d Active class III/IV ± LN Corticosteroids Methylprednisolone IV 0.25-0.50 g/d for 1 to 3 days, then prednisone PO 0.6-1.0 mg/kg/d (not to exceed 80 mg/d) and taper over a few months to maintenance dose Chronic class III/IV ± V LN without activity Supportive treatment for CKD If concomitant class V, manage as class V 1. https://www.kidney-international.org/article/S0085-2538(21)00562-7/fulltext And