Emergency Medicine and Immuno-Oncology Intersect: Recognizing and Managing Cancer Immunotherapy–Related Adverse Effects in the Emergency Department
•
2 gefällt mir•160 views

Daniel Pallin, MD, MPH, and Douglas B. Johnson, MD, MSCI, prepared useful practice aids pertaining to immune-related adverse events for this CME/MOC/CE activity titled "Emergency Medicine and Immuno-Oncology Intersect: Recognizing and Managing Cancer Immunotherapy–Related Adverse Effects in the Emergency Department." For the full presentation, monograph, complete CME/MOC/CE information, and to apply for credit, please visit us at http://bit.ly/2PRv8Ul. CME/MOC/CE credit will be available until November 20, 2019.

Empfohlen
Empfohlen
Weitere ähnliche Inhalte
Was ist angesagt?
Was ist angesagt? (19)
Ähnlich wie Emergency Medicine and Immuno-Oncology Intersect: Recognizing and Managing Cancer Immunotherapy–Related Adverse Effects in the Emergency Department
Ähnlich wie Emergency Medicine and Immuno-Oncology Intersect: Recognizing and Managing Cancer Immunotherapy–Related Adverse Effects in the Emergency Department (20)
Mehr von PVI, PeerView Institute for Medical Education
Mehr von PVI, PeerView Institute for Medical Education (20)
Kürzlich hochgeladen
Kürzlich hochgeladen (20)
Emergency Medicine and Immuno-Oncology Intersect: Recognizing and Managing Cancer Immunotherapy–Related Adverse Effects in the Emergency Department
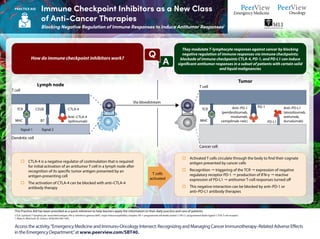
- 1. CTLA: cytotoxic T-lymphocyte–associated antigen; IFN-γ: interferon gamma; MHC: major histocompatibility complex; PD-1: programmed cell death protein 1; PD-L1: programmed death-ligand 1; TCR: T-cell receptor. 1. Ribas A, Wolchock JD. Science. 2018;359:1350-1355. This Practice Aid has been provided as a quick reference to help learners apply the information to their daily practice and care of patients. They modulate T-lymphocyte responses against cancer by blocking negative regulation of immune responses via immune checkpoints; blockade of immune checkpoints CTLA-4, PD-1, and PD-L1 can induce significant antitumor responses in a subset of patients with certain solid and liquid malignancies How do immune checkpoint inhibitors work? o Activated T cells circulate through the body to find their cognate antigen presented by cancer cells o Recognition " triggering of the TCR " expression of negative regulatory receptor PD-1 " production of IFN-γ " reactive expression of PD-L1 " antitumor T-cell responses turned off o This negative interaction can be blocked by anti–PD-1 or anti–PD-L1 antibody therapies o CTLA-4 is a negative regulator of costimulation that is required for initial activation of an antitumor T cell in a lymph node after recognition of its specific tumor antigen presented by an antigen-presenting cell o The activation of CTLA-4 can be blocked with anti–CTLA-4 antibody therapy T cells activated A Q Lymph node T cell Dendritic cell TCR MHC Signal 1 Signal 2 CD28 B7 CTLA-4 Anti–CTLA-4 (ipilimumab) Via bloodstream Tumor T cell Cancer cell TCR MHC Anti–PD-L1 (atezolizumab, avelumab, durvalumab) Anti–PD-1 (pembrolizumab, nivolumab, cemiplimab-rwlc) PD-L1 PD-1 Access the activity,“Emergency Medicine and Immuno-Oncology Intersect: Recognizing and Managing Cancer Immunotherapy–Related Adverse Effects in the Emergency Department,”at www.peerview.com/SBT40. Immune Checkpoint Inhibitors as a New Class of Anti-Cancer Therapies Blocking Negative Regulation of Immune Responses to Induce Antitumor Responses1 PRACTICE AID
- 2. CRC: colorectal cancer; CSCC: cutaneous squamous-cell carcinoma; CTLA: cytotoxic T-lymphocyte–associated antigen; dMMR: mismatch repair deficient; HCC: hepatocellular carcinoma; HNSCC: head and neck squamous cell carcinoma; MSI-H: microsatellite instability high; PD-1: programmed death 1; PD-L1: programmed death-ligand 1; RCC: renal cell carcinoma. 1. https://www.fda.gov/drugs/informationondrugs/approveddrugs/ucm279174.htm. Accessed August 21, 2018. This Practice Aid has been provided as a quick reference to help learners apply the information to their daily practice and care of patients. Access the activity,“Emergency Medicine and Immuno-Oncology Intersect: Recognizing and Managing Cancer Immunotherapy–Related Adverse Effects in the Emergency Department,”at www.peerview.com/SBT40. Immune Checkpoint Inhibitors as a New Class of Anti-Cancer Therapies Timeline of FDA Approvals and Current Indications1 PRACTICE AID September Pembrolizumab (melanoma) December Nivolumab (melanoma) March Ipilimumab (melanoma) 2011 2014 2015 2016 2017 2018 May Atezolizumab (bladder) August Pembrolizumab (HNSCC) October Pembrolizumab (PD-L1+ NSCLC, first line) Atezolizumab (NSCLC, second line) November Nivolumab (HNSCC) March Nivolumab (squamous NSCLC, second line) October Nivolumab (nonsquamous NSCLC, second line) Pembrolizumab (PD-L1+ NSCLC, second line) Nivolumab + ipilimumab (melanoma, first line) Ipilimumab (melanoma, adjuvant) November Nivolumab (RCC) December Pembrolizumab (melanoma, first line) January Nivolumab (bladder) March Avelumab (Merkel cell carcinoma) May Durvalumab, avelumab, pembrolizumab (bladder) Pembrolizumab + chemotherapy (nonsquamous NSCLC, first line) Pembrolizumab (MSI-H cancers) August Nivolumab (dMMR/MSI-H CRC) September Pembrolizumab (gastric) Nivolumab (HCC) December Nivolumab (melanoma, adjuvant) February Durvalumab (stage III NSCLC) April Nivolumab + ipilimumab (RCC, first line) June Pembrolizumab (PD-L1+ cervical) July Nivolumab + ipilimumab (dMMR/MSI-H CRC) August Nivolumab (SCLC, third line) Pembrolizumab + chemotherapy (nonsquamous NSCLC, first line—full approval) September Cemiplimab (CSCC) Drug Ipilimumab Nivolumab Pembrolizumab Atezolizumab Avelumab Durvalumab Mechanism Anti–CTLA-4 Anti–PD-1 Anti–PD-L1
- 3. aTTP: acquired thrombotic thrombocytopenic purpura; irAE: immune-related adverse effect; ITP: Immune thrombocytopenia. 1. https://www.asco.org/sites/new-www.asco.org/files/content-files/practice-and-guidelines/2018-management-of-irAEs-summary.pdf. Accessed September 14, 2018. This Practice Aid has been provided as a quick reference to help learners apply the information to their daily practice and care of patients. Access the activity,“Emergency Medicine and Immuno-Oncology Intersect: Recognizing and Managing Cancer Immunotherapy–Related Adverse Effects in the Emergency Department,”at www.peerview.com/SBT40. Spectrum of Immune-Related Adverse Effects Associated With Immune Checkpoint Inhibitors Used to Treat Patients With Cancer1 Immunotherapies used in oncology are associated with important clinical benefits, but general immunologic enhancement induced by these agents can also lead to a unique spectrum of irAEs Pulmonary Pneumonitis Gastrointestinal Colitis Hepatitis Cardiac Myocarditis Pericarditis Arrhythmias Impaired ventricular function with heart failure and vasculitis Venous thromboembolism Musculoskeletal Inflammatory arthritis Myositis Polymyalgia-like syndrome Dermatologic Rash/Inflammatory dermatitis Bullous dermatoses Severe cutaneous adverse reactions (SCAR) Renal Nephritis Symptomatic nephritis Hematologic Autoimmune hemolytic anemia aTTP Hemolytic uremic syndrome Aplastic anemia Lymphopenia ITP Acquired hemophilia Endocrine Primary hypothyroidism Hyperthyroidism Hypophysitis Primary adrenal insufficiency Diabetes Hepatic Transaminases Hepatitis Ocular Uveitis/iritis Episcleritis Blepharitis Neurologic Neuropathy Meningitis Guillain-Barré syndrome Myasthenia gravis Encephalitis Transverse myelitis irAEs Differ from toxicities of chemotherapies and other cancer therapies Can affect any organ system, but most commonly involve the GI tract, endocrine glands, skin, and liver Can have unpredictable onset (including early or late) Can be difficult to differentiate from other causes (diagnosed by exclusion) PRACTICE AID
- 4. Access the activity,“Emergency Medicine and Immuno-Oncology Intersect: Recognizing and Managing Cancer Immunotherapy–Related Adverse Effects in the Emergency Department,”at www.peerview.com/SBT40. Answers to Common Questions Related to irAEs That Can Occur in Patients With Cancer Treated With Immune Checkpoint Inhibitors1 • Pathophysiology unknown • T-cell, antibody, and cytokine responses may be involved Why Do irAEs Occur? • No prospective trials have defined the best treatments; recommendations based on consensus opinion • Immunosuppression used to $ excess temporary inflammation • Glucocorticoids are usually the first-line immunosuppressive agent • Additional immunosuppressants can be used if glucocorticoids are not initially effective • Side effects of glucocorticoid treatment can occur, and immunosuppression # risk for opportunistic infections How Are irAEs Treated? • Can present at any time, but typically start within the first few weeks to months after treatment initiation and can occur after treatment discontinuation • Dermatologic AEs typically occur first When Do irAEs Occur? PRACTICE AID
- 5. CTLA: cytotoxic T-lymphocyte–associated antigen; irAE: immune-related adverse effect; PD-1: programmed cell death protein 1; PD-L1: programmed death-ligand 1. 1. Postow MA et al. N Engl J Med. 2018;378:158-168. This Practice Aid has been provided as a quick reference to help learners apply the information to their daily practice and care of patients. Access the activity,“Emergency Medicine and Immuno-Oncology Intersect: Recognizing and Managing Cancer Immunotherapy–Related Adverse Effects in the Emergency Department,”at www.peerview.com/SBT40. Answers to Common Questions Related to irAEs That Can Occur in Patients With Cancer Treated With Immune Checkpoint Inhibitors1 PRACTICE AID • Clinical outcomes are similar between patients who do and do not require immunosuppression to treat irAEs • Beneficial responses can persist despite the use of immunosuppressive agents Does Immunosuppression to Treat irAEs Affect Response to Immune Checkpoint Blockade? • irAEs associated with one type of agent (eg, anti–CTLA-4 antibodies) may not necessarily recur during subsequent treatment with another agent (eg, anti–PD-1/–PD-L1 antibodies) • The safety of retreatment likely depends on the severity of the initial irAE • Patients who have had a favorable response to immune checkpoint blockade and then discontinue treatment because of irAEs generally maintain responses; prospective data are needed to address the necessity of restarting immunotherapy Can Immunotherapy Be Safely Restarted After a Major irAE? • Patients with # risk for irAEs (eg, those with pre-existing autoimmune conditions) may still benefit from treatment • Age alone should not be used to exclude patients from treatment, since benefit appears to be similar regardless of age Can Patients at an Increased Risk of irAEs Be Safely Treated With Immune Checkpoint Blockade? • Conflicting data exist regarding whether the occurrence of irAEs is associated with # treatment efficacy • irAEs not required for treatment benefit, although certain AEs (eg, vitiligo) are linked to # treatment response Are There Associations Between irAEs and Treatment Efficacy?
- 6. CAR: chimeric antigen receptor; DDx: differential diagnosis; irAE: immune-related adverse effect; PMHx: past medical history. This Practice Aid has been provided as a quick reference to help learners apply the information to their daily practice and care of patients. Access the activity,“Emergency Medicine and Immuno-Oncology Intersect: Recognizing and Managing Cancer Immunotherapy–Related Adverse Effects in the Emergency Department,”at www.peerview.com/SBT40. Managing Immune-Related Adverse Effects in the Emergency Department PAST MEDICAL HISTORY o Ask about history of cancer o If positive, ask about cancer therapies received within past year – Does treatment history include cancer immunotherapy (eg, immune checkpoint inhibitors, CAR-T cell therapy)? IMMUNOTHERAPY IN PMHx " MODIFY DDx o Almost any inflammatory conditions, endocrinopathies from checkpoint inhibitors o Cytokine-release syndrome, neurotoxicity from CAR-T cell therapy irAEs in the ED Change your practice! ALWAYS CALL THE ONCOLOGIST! AVOID PREMATURE CLOSURE o Don't settle too early on any oncologic or nononcologic diagnoses o Examples Premature Closure on a Nononcology Diagnosis Your Diagnosis Sepsis Depression Benign headache Cellulitis Viral syndrome Pneumonia Real Diagnosis Cytokine-release syndrome Adrenal insufficiency Hypophysitis Immune-mediated dermatitis or radiation recall Immune-mediated hepatitis Immune-mediated pneumonitis Premature Closure on an Oncology Diagnosis Your Diagnosis Immune-mediated colitis Cytokine-release syndrome Real Diagnosis C. difficile colitis Sepsis SIMPLIFY TREATMENT DECISIONS o Immunosuppression used to reduce excessive state of temporary inflammation o Glucocorticoids should typically be used as first-line immunosuppressive therapy o Additional immunosuppressive agents can be used if glucocorticoids are not initially effective Always coordinate with oncology! PRACTICE AID