Advancing the Management of Urothelial Cancer With Immuno-Oncology and Targeted Approaches: Key Concepts for Urology Professionals on the Front Lines of Care
•
2 gefällt mir•302 views

Neal D. Shore, MD, FACS, Arjun Balar, MD, and Noah M. Hahn, MD, prepared useful Practice Aids pertaining to bladder cancer for this CME activity titled "Advancing the Management of Urothelial Cancer With Immuno-Oncology and Targeted Approaches: Key Concepts for Urology Professionals on the Front Lines of Care." For the full presentation, monograph, complete CME information, and to apply for credit, please visit us at http://bit.ly/2Q6c1U4. CME credit will be available until June 5, 2020.

Empfohlen
Empfohlen
Weitere ähnliche Inhalte
Mehr von PVI, PeerView Institute for Medical Education
Mehr von PVI, PeerView Institute for Medical Education (20)
Kürzlich hochgeladen
Kürzlich hochgeladen (20)
Advancing the Management of Urothelial Cancer With Immuno-Oncology and Targeted Approaches: Key Concepts for Urology Professionals on the Front Lines of Care
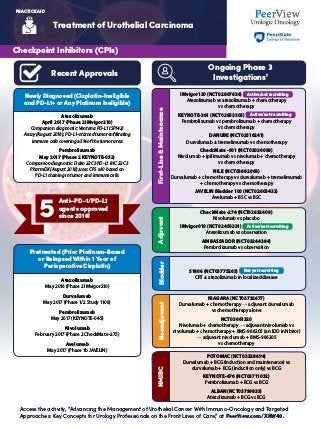
- 1. Treatment of Urothelial Carcinoma Access the activity, “Advancing the Management of Urothelial Cancer With Immuno-Oncology and Targeted Approaches: Key Concepts for Urology Professionals on the Front Lines of Care,” at PeerView.com/XNW40. PRACTICE AID Checkpoint Inhibitors (CPIs) Recent Approvals Newly Diagnosed (Cisplatin-Ineligible and PD-L1+ or Any Platinum Ineligible) Pretreated (Prior Platinum-Based or Relapsed Within 1 Year of Perioperative Cisplatin) Ongoing Phase 3 Investigations1 Atezolizumab April 2017 (Phase 2 IMvigor210) Companion diagnostic: Ventana PD-L1 (SP142) Assay (August 2018); PD-L1–stained tumor-infiltrating immune cells covering ≥5% of the tumor area Pembrolizumab May 2017 (Phase 2 KEYNOTE-052) Companion diagnostic: Dako 22C3 PD-L1 IHC 22C3 PharmDX (August 2018); uses CPS ≥10 based on PD-L1 staining in tumor and immune cells Atezolizumab May 2016 (Phase 2 IMvigor210) Durvalumab May 2017 (Phase 1/2 Study 1108) Pembrolizumab May 2017 (KEYNOTE-045) Nivolumab February 2017 (Phase 2 CheckMate -275) Avelumab May 2017 (Phase 1b JAVELIN) IMvigor130 (NCT02807636) Active/not recruiting Atezolizumab vs atezolizumab + chemotherapy vs chemotherapy KEYNOTE-361 (NCT02853305) Active/not recruiting Pembrolizumab vs pembrolizumab + chemotherapy vs chemotherapy DANUBE (NCT02516241) Durvalumab ± tremelimumab vs chemotherapy CheckMate -901 (NCT03036098) Nivolumab + ipilimumab vs nivolumab + chemotherapy vs chemotherapy NILE (NCT03682068) Durvalumab + chemotherapy vs durvalumab + tremelimumab + chemotherapy vs chemotherapy JAVELIN Bladder 100 (NCT02603432) Avelumab + BSC vs BSC First-Line&Maintenance CheckMate -274 (NCT02632409) Nivolumab vs placebo IMvigor010 (NCT02450331) Active/not recruiting Atezolizumab vs observation AMBASSADOR (NCT03244384) Pembrolizumab vs observation Adjuvant NIAGARA (NCT03732677) Durvalumab + chemotherapy → adjuvant durvalumab vs chemotherapy alone NCT03661320 Nivolumab + chemotherapy → adjuvant nivolumab vs nivolumab + chemotherapy + BMS-986205 (an IDO inhibitor) → adjuvant nivolumab + BMS-986205 vs chemotherapy Neoadjuvant POTOMAC (NCT03528694) Durvalumab + BCG (induction and maintenance) vs durvalumab + BCG (induction only) vs BCG KEYNOTE-676 (NCT03711032) Pembrolizumab + BCG vs BCG ALBAN (NCT03799835) Atezolizumab + BCG vs BCG NMIBC S1806 (NCT03775265) Not yet recruiting CRT ± atezolizumab in localized disease Bladder Anti–PD-1/PD-L1 agents approved since 2016!5
- 2. Treatment of Urothelial Carcinoma Access the activity, “Advancing the Management of Urothelial Cancer With Immuno-Oncology and Targeted Approaches: Key Concepts for Urology Professionals on the Front Lines of Care,” at PeerView.com/XNW40. PRACTICE AID Antibody–Drug Conjugates (ADCs) Mechanism of Action Selected Clinical Trials1 Target: Nectin-4, a type 1 transmembrane cell adhesion molecule overexpressed in epithelial cancers Linker: Protease cleavable Payload: MMAE Target: Trop-2, an epithelial cell-surface glycoprotein highly expressed in muscle-invasive disease Linker: Hydrolysable Payload: SN-38, the active metabolite of irinotecan Enfortumab Vedotin2 Sacituzumab Govitecan (IMMU-132)3 EV-103 (NCT02091999) Phase 1 Enfortumab vedotin dose escalation in patients with resistant/recurrent tumors expressing nectin-4, including in patients previously treated with CPIs EV-201 (NCT03219333) Pivotal Phase 2 Enfortumab vedotin in patients with locally advanced or metastatic UC who previously received CPIs EV-301 (NCT03474107) Phase 3 Enfortumab vedotin vs chemotherapy in patients with previously treated locally advanced or metastatic UC that shows radiographic progression or has relapsed during or after CPI therapy TROPHY-U-01 (NCT03547973) Phase 2 Sacituzumab govitecan in patients with unresectable locally advanced or metastatic UC who progress after platinum- based chemotherapy and CPI therapy or who are ineligible for platinum-based chemotherapy and progress after CPI 1Binds to antigen 5 Cell cycle arrest and apoptosis 2Complex is internalized 4Microtubule disruption 3Payload is released
- 3. Treatment of Urothelial Carcinoma Access the activity, “Advancing the Management of Urothelial Cancer With Immuno-Oncology and Targeted Approaches: Key Concepts for Urology Professionals on the Front Lines of Care,” at PeerView.com/XNW40. PRACTICE AID This Practice Aid has been provided as a quick reference to help learners apply the information to their daily practice and care of patients. BCG: Bacillus Calmette-Guerin; CPI: checkpoint inhibitor; CPS: combined positive score; CRT: chemoradiotherapy; ECM: extracellular matrix; FGF: fibroblast growth factor; FGFR: fibroblast growth factor receptor; IDO: indoleamine 2,3-dioxygenase 1; IHC: immunohistochemistry; MMAE: monomethyl auristatin E; NMIBC: non–muscle-invasive bladder cancer; PD-1: programmed cell death protein 1; PD-L1: programmed death ligand 1; UC: urothelial carcinoma. 1. www.clinicaltrials.gov. Accessed April 19, 2018. 2. Challita-Eid PM et al. Cancer Res. 2016;76:1-11. 3. Bardia A et al. 2018 Annual Meeting of the American Society of Clinical Oncology (ASCO 2018). Abstract 1004. 4. Touat M et al. Clin Cancer Res. 2015;21:2684-2694. 5. https://www.targetedonc.com/news/fda-grants-fast-track-designation-to-vofatamab-for-fgfr3-bladder-cancer. Accessed April 22, 2019. FGF FGF FGF FGF FGFR HSPG FGF FGF FGFRL1 SEF SPRY FRS2 PLC-y DAG STAT GAB1 SOSGRB2 RAS RAF MEK ERK MKP3 MKP1 AKT PKC PI3K Nucleus Transcription of target genes Cytoplasm Extracellular PIP2 P P P P P P P P P P P P IP3 Plasma membrane Proliferation and survival Resistance to anticancer agents Neoangiogenesis FGFR alterations: Amplification (receptor overexpression) or mutation/translocation (ligand-independent signaling) FGF ligand: Amplification (autocrine) or ECM/stromal- cell release (paracrine) FGFR Inhibitors FGFRs are a family of receptor tyrosine kinases that are upregulated in multiple different cancers and are involved in tumor cell differentiation and proliferation, tumor angiogenesis, and tumor cell survival; alterations in the FGFR gene, such as mutations and translocations, have been implicated in the pathogenesis of UC Erdafitinib Approved April 12, 2019 (Phase 2 BLC2001) Patients with locally advanced or metastatic UC, with susceptible FGFR3 or FGFR2 genetic alterations (therascreen FGFR RGQ RT- PCR Assay), that has progressed during or following platinum- containing chemotherapy, including within 12 months of neoadjuvant or adjuvant platinum-containing chemotherapy First Approval of a Targeted Therapy in UC Erdafitinib THOR (NCT03390504) Phase 3 Erdafitinib vs chemotherapy or pembrolizumab in previously treated patients with advanced UC harboring selected FGFR aberrations Cohort 1: 1-2 prior therapies, including ≥1 prior anti–PD-L1– containing regimen Cohort 2: 1 prior therapy that does not include an anti–PD-L1 agent Pemigatinib FIGHT-201 (NCT02872714) Phase 2 Pemigatinib in patients with metastatic or unresectable UC harboring FGF/FGFR alterations who have failed ≥1 therapy or are platinum ineligible NCT03914794 Phase 2 Pemigatinib in NMIBC patients with recurrent low- or intermediate-risk tumors Vofatamab FIERCE-21 (NCT02401542) Phase 1/2 Vofatamab alone or in combination with docetaxel versus docetaxel alone in FGFR3-mutant/fusion patients with stage IV, locally advanced, or metastatic UC who have relapsed after, or are refractory to, ≥1 prior line of chemotherapy FIERCE-22 (NCT03123055) Phase 1/2 Vofatamab + pembrolizumab in patients with locally advanced or metastatic UC who have progressed following platinum-based chemotherapy and are CPI naïve FIERCE-23 Vofatamab as a single agent in patients with NMIBC Selected Clinical Trials1,5 Not yet recruiting Planned Active/not recruiting FGFR Signaling Pathway4
- 4. Urologists' Guide to Managing Adverse Events Associated With Immune Checkpoint Inhibitors1,2 Access the activity, “Advancing the Management of Urothelial Cancer With Immuno-Oncology and Targeted Approaches: Key Concepts for Urology Professionals on the Front Lines of Care,” at PeerView.com/XNW40. PRACTICE AID This Practice Aid has been provided as a quick reference to help learners apply the information to their daily practice and care of patients. ASCO: American Society of Clinical Oncology; CTLA-4: cytotoxic T-lymphocyte–associated protein 4; irAE: immune-related adverse event. 1. Postow MA et al. N Engl J Med. 2018;378:158-168. 2. Brahmer JR et al. J Clin Oncol. 2018;36:1714-1768. • In general, checkpoint inhibitor therapy should be continued with close monitoring, with the exception of some neurologic, hematologic, and cardiac toxicities Minimalornosymptoms;diagnosticchangesonly Grade 1 What is the spectrum of potential irAEs?Why do irAEs occur? Immune checkpoint inhibitors are associated with important clinical benefits, but general immunologic enhancement can also lead to a unique spectrum of irAEs A team-based approach to identification and management of irAEs is important, particularly as immune checkpoint inhibitors move into management paradigms for earlier disease states General recommendations and management principles include the following: irAEs are often diagnosed by exclusion; other causes should be ruled out (including AEs of other therapies used), but immunotherapy-related toxicity should always be included in the differential There should be a high level of suspicion that new symptoms are treatment-related; early recognition, evaluation, and treatment of irAEs plus patient education are essential for best outcome Depending on severity of irAEs, management may require corticosteroid or other immunosuppressive treatment and interruption or discontinuation of therapy If appropriate immunosuppressive treatment is used, patients generally recover from irAEs Use of immunosuppressive therapy to manage irAEs does not affect response to immunotherapy How should irAEs be diagnosed and managed? • Hold checkpoint inhibitor therapy for most grade 2 toxicities • Consider resuming immunotherapy when symptoms and/or laboratory values revert to grade 1 or lower • Corticosteroids (initial dose of 0.5-1 mg/kg/d of prednisone or equivalent) may be administered Grade 3 toxicities: • Hold checkpoint inhibitor therapy • Initiate high-dose corticosteroids (prednisone 1-2 mg/kg/d or methylprednisolone IV 1-2 mg/kg/d) • If symptoms do not improve with 48-72 hours of high-dose corticosteroids, infliximab may be offered for some toxicities • Taper corticosteroids over the course of at least 4-6 weeks • When symptoms and/or laboratory values revert to grade 1 or lower, rechallenging with immunotherapy may be offered; however, caution is advised, especially in those patients with early-onset irAEs. Dose adjustments are not recommended Grade 4 toxicities: • In general, permanent discontinuation of checkpoint inhibitor therapy is warranted, with the exception of endocrinopathies that have been controlled by hormone replacement Brahmer JR et al. Management of Immune-Related Adverse Events in PatientsTreated With Immune Checkpoint InhibitorTherapy: American Society of Clinical Oncology Clinical Practice Guideline. J Clin Oncol. 2018;36:1714-1768. For organ-specific assessment and management of irAEs, please see the ASCO guidelines: Additional resources available on the ASCO website: https://www.asco.org/practice-guidelines/quality-guidelines/guidelines/ supportive-care-and-treatment-related-issues#/29866 Grade 2 Mild to moderate symptoms Severe or life-threatening symptoms Grades 3/4 Any organ system can be affected; commonly occurring are pulmonary (pneumonitis), dermatologic (rash, pruritus, blisters, ulcers, vitiligo), gastrointestinal (diarrhea, enterocolitis, transaminitis, hepatitis, pancreatitis), and endocrine (thyroiditis, hypophysitis, adrenal insufficiency) irAEs The precise pathophysiology is unknown, but translational studies have shown that T-cell, antibody, and cytokine responses may be involved Q Q Q A A A Increasing T-cell activity against antigens that are present in tumors and healthy tissue Activated T cell Antithyroid antibodies Increasing levels of inflammatory cytokines Increasing levels of pre-existing autoantibodies Enhancing complement-mediated inflammation due to direct binding of an anti–CTLA-4antibody with CTLA-4 expressed on normal tissue Activated T cell Anti–CTLA-4 antibody CTLA-4 on pituitary Complement- mediated inflammation Cytokines Tumor with antigen and activated T cells Pancreatitis, autoimmune diabetes Colitis Enteritis Encephalitis, aseptic meningitis Thyroiditis, hypothyroidism, hyperthyroidism Dry mouth, mucositis Hypophysitis Uveitis Pneumonitis Thrombocytopenia, anemia Hepatitis Adrenal insufficiency Nephritis Vasculitis Arthralgia Neuropathy Rash, vitiligo Myocarditis