Inflammatory bowel disease
•Als PPTX, PDF herunterladen•
39 gefällt mir•15,438 views


Empfohlen
Weitere ähnliche Inhalte
Was ist angesagt?
Was ist angesagt? (20)
Andere mochten auch
Andere mochten auch (20)
Ähnlich wie Inflammatory bowel disease
Ähnlich wie Inflammatory bowel disease (20)
Mehr von Subramani Parasuraman
Mehr von Subramani Parasuraman (20)
Kürzlich hochgeladen
Kürzlich hochgeladen (20)
Inflammatory bowel disease
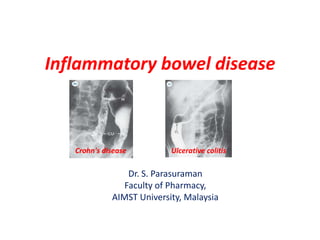
- 1. Inflammatory bowel disease Crohn's disease Ulcerative colitis Dr. S. Parasuraman Faculty of Pharmacy, AIMST University, Malaysia
- 2. Inflammatory bowel disease (IBD) • IDB is a group of inflammatory conditions of the colon and small intestine. • The major types of IBD – Crohn's disease – Ulcerative colitis • Ulcerative colitis (involves ascending colon) causes long-lasting inflammation in digestive tract. Symptoms usually develop over time, rather than suddenly. Ulcerative colitis usually affects only the innermost lining of large intestine (colon) and rectum. • Crohn's disease (involves sigmoid and descending colon) causes inflammation anywhere along the lining of digestive tract, and often spreads deep into affected tissues. This can lead to abdominal pain, severe diarrhea and even malnutrition.
- 3. Symptoms of IBD • The severity of symptoms is very form time to time and form person to person, which includes – – – – – – – – – Pain in the abdomen Weight loss Diarrhoea (sometimes with blood and mucus) Tiredness Constipation Malnutrition Nausea Vomiting Delayed or impaired growth in children.
- 4. Causes of Crohn’s disease and colitis • The causes of these diseases are unknown. • It is believed that, the cause might be a defect in the body’s immune system. Diagnosis of Crohn’s disease and colitis • Blood tests – blood cell counts and erythrocytes sedimentation rates[ESR] – red blood cell counts (anemia), low blood proteins, and low body minerals, reflecting loss of these minerals due to chronic diarrhea • Faecal (bowel motion) examination • X-rays – • Barium X-ray studies can be used to define the distribution, nature, and severity of the disease Colonoscopy and gastroscopy
- 5. Symptoms of Crohn’s disease and colitis • The severity of symptoms is very form time to time and form person to person, which includes – – – – – – – – – Pain in the abdomen Weight loss Diarrhoea (sometimes with blood and mucus) Tiredness Constipation Malnutrition Nausea Vomiting Delayed or impaired growth in children.
- 6. Characteristics in Crohn’s Disease and Ulcerative Colitis Crohn’s disease Ulcerative colitis Age of onset 10 – 40 yr 10 – 30 yr Location Large intestine (distal ileum and colon) Large or small intestine Involves ascending colon Involves sigmoid and descending colon Inflammation Skip lesions Uniform and continuous Layers involved Mainly submucosal Mainly mucosal Bloody stool Rare Common Diarrhea Common Common Malabsorption Rate Common Abdominal pain Mild to severe Mild to severe
- 7. Crohn’s disease- Pathology • Crohn’s disease affects the terminal ileum and ascending colon (70% of cases). • The inflammation is transmural (affects the whole thickness of the bowel wall) and involves the mesentery and lymph nodes and causing adhesions between loop of bowel. • The affected bowel is hard, rubbery and narrowed with a small lumen (the ‘string sing’) and become fibrosed.
- 8. Crohn’s disease-Etiology • Etiology is unknown. Possible role of pre-inflammatory cytokines in the pathogenesis may cause Crohn’s disease. • Possible association found with Mycobacterium paratuberculosis, measles and mumps infections. • Associated environmental factors: Infection, smocking, consumption of refined sugar, high fiber • Most common in distal ileum and colon. Crohn’s disease- Epidemiology • Inflammatory bowel disease affects all race and both sexes. • The incidence is generally higher in developed countries, especially in Northern Europe. • Lack of dietary fiber, environmental and genetic factor are infusing the disease progression.
- 9. Manifestations of Crohn’s disease • Diarrhea (blood is usually not evident in the stool but may be occult, i.e., detected by clinical assay) • Intestinal pain similar to indigestion • Fever • Weight loss from intestinal malabsorption • Nausea, anorexia, vomiting • Complications: intestinal obstruction, formation of fistulas • Toxic megacolon – Life-threatening distention of the colon. – May lead to perforation of the colon, septicemia and peritonitis. – Mortality associated with a perforated colon is on the order of 40% or more.
- 10. Treatment of Crohn’s disease • Nutritional supplementation (poor nutrition that can result from anorexia and intestinal malabsorption) • Total parenteral nutrition may be indicated in severe cases • Anti-inflammatory drugs: sulfasalazine, Mesalamine, corticosteroids • Antibodies that block cytokine: metronidazole, ciprofloxacin
- 11. Ulcerative colitis - Pathology • Rectum is involved in over 90% of cases of ulcerative colitis and inflammation may spread to involved the sigmoid and descending colon. • In severe cases (chronic and non-episodic), whole of the colon (pancolitis) affected. Severe causes may be life-threatening. • It may be affect terminal part of ileum. • Unlike Crohn’s disease the pattern of inflammation is continuous throughout the affected area. • Ulcerative colitis may cause 10-20 watery, bloody motions with mucus throughout a 24 h period.
- 12. Manifestations of ulcerative colitis • Chronic, bloody diarrhea • Fever, pain • Weight loss • Possible anemia from blood loss • Possible complications: toxic megacolon, perforation of the intestine, significant blood loss; an increased incidence of colon cancer
- 13. Diagnosis of ulcerative colitis • Requires a careful history and examination • Investigations include a full blood count, ESR, electrolytes, barium meal and follow-through, double-contrast barium enema, sigmoidoscopy and/or colonoscopy and biopsy, and stool cultures.
- 14. Treatment of ulcerative colitis • Anti-inflammatory drugs (salicylates) • Sulfasalazine — A combination sulfa and aminosalicylate drug. • Nicotine appears to exert a protective effect in ulcerative colitis but not Crohn’s disease. • Severe malnutrition may require nutritional supplementation. • Surgical resection of diseased bowel may be required.
- 15. Management of ulcerative colitis • Rapid symptom relief and prompt control of acute attacks • Correction of metabolic disturbances • Prevention of serious complications • Long-term immunosuppressive and/or anti-inflammatory, • Prophylactic or maintenance therapy (for some patients) • Anticipation of the need for surgery and, if possible, avoidance of emergency procedures.
- 16. Thank you