Manyata Tech Park ( Call Girls ) Bangalore ✔ 6297143586 ✔ Hot Model With Sexy...
Acid base imbalance in medicine
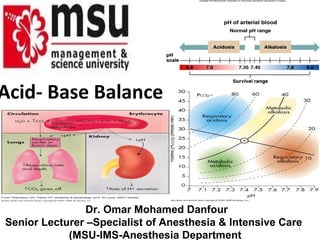
1. Acid- Base Balance
Dr. Omar Mohamed Danfour
Senior Lecturer –Specialist of Anesthesia & Intensive Care
1
(MSU-IMS-Anesthesia Department
2. pH Review
• PH = - log [H+]
• H+ is really a proton
• If [H+] is high, the solution is acidic pH
• If [H+] is low, the solution is basic or alkaline pH
• Acids are H+ donors.
• Bases are H+ acceptors, or give up OH- in solution.
• Acids and bases can be:
– Strong – dissociate completely in solution
• HCl, NaOH
– Weak – dissociate only partially in solution
• Lactic acid, carbonic acid 2
3. Acid Base -Basic Concepts
• Hydrogen Ion [H+] is tightly controlled
• [H+] is determined by the balance between PaCO2
and serum HCO3 (bicarbonate),
{normal ratio is 20 (Hco3) : 1(H2Co3)}
Henderson-Hasselbalch Equation
[H+] = 24 (PaCO2 / HCO3-)
Normal Values
– [H+] = 40 nEq/L
– pH = 7.40 (7.35-7.45)
– PaCO2 = 40 mm Hg (35-45)
– HCO3 = 24 mEq/L (22-26)
– < 6.8 or > 8.0 death occurs 3
8. Small changes in pH can produce major disturbances
• Most enzymes function only with narrow pH ranges
• Acid-base balance can also affect electrolytes (Na+,
K+, Ca++, Cl-)
• Can also affect hormones
• The body produces more acids than bases
• Acids take in with foods
• Acids produced by metabolism of lipids and
proteins
• Cellular metabolism produces CO2.
• CO2 + H20 ↔ H2CO3 ↔ H+ + HCO3- 8
9. Control of Acids
1. Buffer systems
Take up H+ or release H+ as conditions change
Buffer pairs – weak acid and a base
Exchange a strong acid or base for a weak one
Results in a much smaller pH change
CO2 + H20 ↔ H2CO3 ↔ H+ + HCO3-
Bicarbonate buffer
• Sodium Bicarbonate (NaHCO3) and carbonic acid (H2CO3)
• Maintain a 20:1 ratio : HCO3- : H2CO3
HCl strong Acid + NaHCO3 weak Base ↔ H2CO3 weak acid + NaCl
9
10. Phosphate buffer
• Major intracellular buffer
• H+(acid) + HPO42- ↔ H2PO4- (titratable acids eliminated in urine)
• OH-(Base) + H2PO4-acid ↔ H2O + H2PO42-
Protein Buffers
• Hemoglobin is rich in histidine which is an effective
buffer from PH5.7 to 7.7.(Hb in RBCs in equilibrium
as a weak acid(HHB) and a potassium salt (KHb)
• Carboxyl group gives up H+
• Amino Group accepts H+
• Side chains that can buffer H+ are present on 27 10
11. 2. Respiratory mechanisms
• Exhalation of carbon dioxide
• Powerful, but only works with volatile acids
• Doesn’t affect fixed acids like lactic acid
• CO2 + H20 ↔ H2CO3 ↔ H+ + HCO3-
• Body pH can be adjusted by changing rate and depth of
breathing
3. Kidney excretion
• Can eliminate large amounts of acid
• Can also excrete base
• Can conserve and produce bicarb ions
• Most effective regulator of pH
• If kidneys fail, pH balance fails 11
12. Rates of correction
• Buffers function almost
instantaneously (rapid)
• Respiratory mechanisms take several
minutes to hours
• Renal mechanisms may take several
hours to days
12
14. Acid-Base Imbalances
• pH< 7.35 acidosis
• pH > 7.45 alkalosis
• The body response to acid-base imbalance is called
compensation
• May be complete if brought back within normal
limits
• Partial compensation if range is still outside normals
• If underlying problem is metabolic, hyperventilation
or hypoventilation can help : respiratory
compensation.
• If problem is respiratory, renal mechanisms can
bring about metabolic compensation 14
16. Respiratory Acidosis
• Carbonic acid excess caused by blood levels of CO2
above 45 mm Hg.
• Hypercapnia – high levels of CO2 in blood
Causes:
• Chronic conditions:
– Depression of respiratory center in brain that
controls breathing rate – drugs or head trauma
– Paralysis of respiratory or chest muscles
– COPD, pneumonia & obesity
CO2 + H20 ↔ H2CO3 ↔ H+ + HCO3-
16
18. Signs and Symptoms of Respiratory Acidosis
• Breathlessness
• Restlessness
• Lethargy and disorientation
• Tremors, convulsions, coma
• Respiratory rate rapid, then gradually
depressed
• Skin warm and flushed due to vasodilation
caused by excess CO2
18
19. Compensation for Respiratory Acidosis
• This is accomplished via two mechanisms;
a) rapid cell buffering and
• In this setting, carbonic acid (H2CO3 ) can only be
buffered by the limited intracellular buffers
(primarily hemoglobin and proteins).
H2CO3 + Hb- → HHb + HCO3-
b) an increase in net acid excretion.
• Kidneys eliminate hydrogen ion and retain
bicarbonate ion (Chronic state) 19
21. Treatment of Respiratory Acidosis
• Restore & improve alveolar ventilation
• IV lactate solution (converted to bicarbonate
ions in the liver).
• Treat underlying dysfunction or disease
e.g. pul odema, Res depression
21
22. Respiratory Alkalosis
• Carbonic acid deficit
• pCO2 less than 35 mm Hg (hypocapnea)
• Most common acid-base imbalance
• Primary cause is hyperventilation
CO2 + H20 ↔ H2CO3 ↔ H+ + HCO3-
22
23. Respiratory Alkalosis
• Conditions that stimulate respiratory center:
– Oxygen deficiency at high altitudes
– Pulmonary disease and Congestive heart failure – caused
by hypoxia
– Acute anxiety & pain
– Fever, anemia
– Early salicylate intoxication
– Cirrhosis
– Gram-negative sepsis
– Iatrogenic (ventilator induced)
23
24. Signs and Symptoms of Respiratory Alkalosis
• Alkalosis causes over excitability of the central and
peripheral nervous systems.
• Numbness
• Light headedness
• It can cause :
– Nervousness
– muscle spasms or tetany
– Convulsions
– Loss of consciousness
– Death
24
25. Compensation of Respiratory Alkalosis
• There are two mechanisms responsible for this
compensation to respiratory alkalosis;
1) Rapid cell buffering and
2) Decrease in net renal acid excretion.
• hydrogen ions move from the cells into the extracellular
fluid, where they combine with [HCO3- to form carbonic
acid in the following reaction:
H+ + HCO3- → H2CO3 (CA)
• In acute respiratory alkalosis, for every 10 mmHg decrease in the
PCO2, there is a 2meq/L decrease in the plasma HCO3-
concentration.
• In chronic state renal compensation result in a 4 meq/L reduction in
plasma [HCO3-] for every 10 mmHg reduction in PCO2. 25
27. Treatment of Respiratory Alkalosis
• Treat underlying cause
• Breathe into a paper bag ???
• IV Chloride containing solution (hydrochloric acid,
arginine chloride & ammonium chloride), Cl- ions
replace lost bicarbonate ions
27
28. Metabolic Acidosis
• Bicarbonate deficit - blood concentrations of
bicarb drop below 22mEq/L
• Occurs when pH falls below 7.35
• Causes:
– Loss of bicarbonate through diarrhea or renal
dysfunction
– Accumulation of acids (lactic acid or ketones)
– Failure of kidneys to excrete H+
[H+] = 24 ×(PCO2 / [HCO3-])
CO2 + H20 ↔ H2CO3 ↔ H+ + HCO3- 28
29. Two types of Metabolic Acidosis
– High Anion Gap = net gain of acid
– Normal anion gap = loss of bicarbonate
Anion Gap Calculation
• [Na+ + K+] – [Cl + HCO3] (Normal = 12 + 2)
E.g :- Na 140, k 4 , CL 114, HCO3 18
(140 + 4) – (114 + 18)
144 – 132 = 12 normal
E.g:- Na 140 , Cl 104, K 4.0, HCO3 10
(144) – (114) = 30 = High anion gap 29
30. Normal Anion Gap High Anion Gap Differential
(USED CARP) (MUDPILES)
• Ureterostomy • Methanol
• Small bowel fistula • Uremia
• Extra Chloride • DKA
• Diarrhea • Paraldehyde
• Carbonic anhydrase • Inborn
inhibitors Errors
• Addison’s disease • Lactic
• Renal tubular acidosis Acidosis
• Pancreatic fistulas • Ethylene
Glycol
Treatment: Replace
• Salicylates
30
31. Symptoms of Metabolic Acidosis
• Headache, lethargy
• Nausea, vomiting, diarrhea
• Coma
• Death
Compensation for Metabolic Acidosis
• Increased ventilation
• Renal excretion of hydrogen ions if possible
• K+ exchanges with excess H+ in ECF
( H+ into cells, K+ out of cells)
CO2 + H20 ↔ H2CO3 ↔ H+ + HCO3-
31
32. Compensation
• Respiratory compensation results in a 1.2 mmHg
reduction in PCO2 for every 1.0 meq/L reduction in
the plasma HCO3- concentration down to a
minimum PCO2 of 10 to 15mmHg.
For example, if an acid load lowers the plasma HCO3-
concentration to 9 meq/L, then:
Degree of HCO3- reduction is 24 (optimal value) – 9 =
15.
Therefore, PCO2 reduction should be 15 × 1.2 = 18.
Then PCO2 measured should be 40 (optimal value) – 18
= 22mmHg.
32
34. Treatment of Metabolic Acidosis
• Treat the causes
• Improve renal perfusion & acid excretion
• NaHCO3, Dose = (weight Kg x base deficit x 0.3)
• Ensure adequate ventilation
34
35. Metabolic Alkalosis
• Characterized by
– Primary ↑ in HCO3 concentration greater than 26 mEq/
L
– Compensatory ↑ in PaCO2
• Classified according to urinary chloride
– Chloride responsive
– Chloride resistant
35
38. Symptoms of Metabolic Alkalosis
• Respiration slow and shallow
• Hyperactive reflexes ; tetany
• Often related to depletion of electrolytes
• Dysrhythmias
Compensation for Metabolic Alkalosis
• Alkalosis most commonly occurs with renal
dysfunction, so can’t count on kidneys
• Alkali load
• Acid loss - vomiting
• Respiratory compensation difficult
(hypoventilation limited by hypoxia) 38
39. Compensation contn.
• The development of alkalemia is sensed by central and
peripheral chemoreceptors, resulting in a reduction in the
rate of ventilation and a reduction in tidal volume and
thus an elevation in the pCO2.
pCO2 rises 0.7 mmHg for every 1.0 meq/L increment in the
plasma [HCO3-].
For example, if an alkali load raises the the plasma HCO3-
concentration to 34 meq/L, then:
Degree of HCO3- elevation is 34 – 24 (optimal value)= 10.
Therefore, PCO2 elevation should be 0.7 × 10 = 7
Then PCO2 measured should be 40 (optimal value) +7 =
47mmHg. 39
41. Treatment of Metabolic Alkalosis
• Electrolytes to replace those lost
• Treat underlying disorder
• IV chloride containing solution e.g saline (Chloride
Responsive)
• Aldosterone antagonist (Chloride resistant)
41
42. Miscellaneous 1
Arterial pH is related to the ratio of PCO2 to HCO3,
both pulmonary & renal compensatory mechanism
are always such that PCO2 and HCO3 change in the
same direction.
the exception occurs when there is a mixed acid
base disorder. In that situation, multiple acid base
processes coexisting may lead to a normal pH or a
mixed picture especially when PCO2 & HCO3
moves in opposite direction
If the compensatory response is more or less than
expected, by definition a mixed acid-base disorder
42
exist.
43. An Alternative Approach
An Alternative Approach that is rapid but perhaps less
precise is to correlate changes in Ph with changes in
CO2 or HCO3.
• For a respiratory disturbance, every 10mmHg changes in
CO2 should change arterial PH by approximately 0.08 U in
the opposite direction.
• During metabolic disturbance, every 6mEq change in HCO3
also changes arterial PH by 0,1 in the same direction.
• If the change in pH exceed or is less than predicted, a
mixed acid-base disorder is likely to be present.
• If the Arterial pH is relatively normal and the PCO2 and/or
HCO3 are abnormal, one can assume that a mixed 43
44. Miscellaneous 2
• The Delta Ratio (∆/∆)
• Assessment of elevated anion gap metabolic
acidosis to determine if a mixed acid base
disorder is present.
Delta ratio = ∆ Anion gap/∆ [HCO3-] or ↑anion gap/ ↓ [HCO3-]
= Measured anion gap – Normal anion gap
Normal [HCO3-] – Measured [HCO3-]
= (AG – 12)
(24 - [HCO3-])
44
45. Miscellaneous cont
Delta ratio Assessment Guidelines
< 0.4 Hyperchloremic normal anion gap acidosis
<1 High AG & normal AG acidosis
1 to 2 Pure Anion Gap Acidosis
Lactic acidosis: average value 1.6
DKA more likely to have a ratio closer to 1 due to urine
ketone loss
High AG acidosis and a concurrent metabolic alkalosis
>2 or a pre-existing compensated respiratory acidosis45
46. Compensation
Primary Disorder Compensatory Mechanism
Metabolic acidosis Increased ventilation
Metabolic alkalosis Decreased ventilation
Respiratory acidosis Increased renal reabsorption of HCO3-
in the proximal tubule
Increased renal excretion of H in the
distal tubule
Respiratory alkalosis Decreased renal reabsorption of HCO3-
in the proximal tubule
Decreased renal excretion of H+ in the
46
47. Compensator Compensatory
Initial Expected level
Primary y
chemical
disorder change compensation
Mechanism
response
PCO2 = (1.5 × [HCO3-]) +
± 2
Metabolic
↓HCO3- ↓PCO2 Hyperventilation ↓PCO2 = 1.2 ×∆ [HCO3-]
Acidosis
PCO2 = (0.9 × [HCO3-]) +
Metabolic 16 ± 2
↑HCO3- ↑PCO2 Hypoventilation
Alkalosis
↑PCO2 = 0.7 × ∆ [HCO3-]
Respiratory
↑PCO2 ↑HCO3-
Acidosis
Intracellular
Buffering
↑[HCO3-] = 1 mEq/L for
Acute (hemoglobin,
every 10 mm Hg ∆PCO2
intracellular
proteins)
Generation of new
HCO3- due to the ↑[HCO3-] = 3.5 mEq/L for
Chronic
increased excretion every 10 mm Hg ∆PCO2
of ammonium.
Respiratory
↓PCO2 ↓HCO3-
Alkalosis
Intracellular ↓[HCO3-] = 2 mEq/L for
Acute
Buffering every 10 mm Hg ∆PCO2
Decreased
reabsorption of 47
↓[HCO3-] =4 mEq/L for
48. Acidemia (PH<7.35)
PCO2
Normal
High
Or low
Incompatible Normal
[HCO3]
[HCO3] or high
Low Low
High Normal
Mixed
Chronic Acute respiratory
respiratory respiratory and metabolic Metabolic
acidosis acidosis acidosis acidosis
48
49. ↓ Plasma [HCO3]
Anion gap
Normal Increased
High anion gap
Plasma [K] metabolic acidosis
Low Normal High
Respiratory Hyperkalemic
Hypokalemic alkalosis
hyperchloremic hyperchloremic
metabolic acidosis metabolic acidosis
49
50. Alkalemia (PH>7.45)
PCO2
Low HighNormal
Normal
[HCO3] Incompatible or [HCO3]
Low
High
High Low
Normal
Mixed
Acute Chronic Metabolic
respiratory and
respiratory respiratory alkalosis
metabolic
alkalosis alkalosis alkalosis 50
52. Example
• A patient is in intensive care because he suffered
a severe myocardial infarction 3 days ago. The
lab reports the following values from an arterial
blood sample:
– pH 7.3
– HCO3- = 20 mEq / L ( 22 - 26)
– pCO2 = 32 mm Hg (35 - 45)
Diagnosis
• Metabolic acidosis
• With partial compensation
52
53. CASE 1
• A 44 year old moderately dehydrated man
was admitted with a two day history of acute
severe diarrhea. Electrolyte results: Na+ 134,
K+ 2.9, Cl- 108, HCO3- 16,
• Urea 31, Cr 1.5.
•
ABG: pH 7.31 pCO2 33 mmHg
HCO3 16 pO2 93 mmHg
53
54. CASE 2
• A 22 year old female with type I DM, presents to the
emergency department with a 1 day history of nausea,
vomiting, polyuria, polydypsia and vague abdominal pain.
P.E. noted for deep sighing breathing, orthostatic
hypotension, and dry mucous membranes.
• Labs: Na 132 , K 6.0, Cl 93, HCO3- 11 glucose 720, Urea 38,
Cr 2.6.
UA: pH 5, SG 1.010, ketones negative, glucose positive .
Plasma ketones trace.
ABG: pH 7.27 HCO3- 10 PCO2 23
• What is the acid base disorder?
54
55. CASE 3
• A 70 year old man
with history of CHF
presents with
increased shortness
of breath and leg
swelling.
ABG: pH 7.24, PCO2
60 mmHg, PO2 52
HCO3- 27
• What is the acid
base disorder? 55

![pH Review
• PH = - log [H+]
• H+ is really a proton
• If [H+] is high, the solution is acidic pH
• If [H+] is low, the solution is basic or alkaline pH
• Acids are H+ donors.
• Bases are H+ acceptors, or give up OH- in solution.
• Acids and bases can be:
– Strong – dissociate completely in solution
• HCl, NaOH
– Weak – dissociate only partially in solution
• Lactic acid, carbonic acid 2](data:image/gif;base64,R0lGODlhAQABAIAAAAAAAP///yH5BAEAAAAALAAAAAABAAEAAAIBRAA7)