This document discusses risks associated with patients slipping in the operating room, especially in Trendelenburg position. It summarizes recommendations from AORN to use anti-skid materials to prevent slipping and recommends avoiding shoulder braces and stirrups. Slipping can cause shearing injuries, nerve damage, pressure injuries and complications during robotic surgery due to shifts in patient position. Anti-skid materials can help reduce risks by preventing slipping and maintaining proper positioning.
1. Anti-skid materials
Potential risk factors associated with slipping:
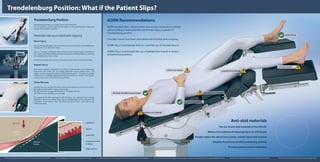
AORN Recommendations
AORN standard VIII.j.1 recommends that we take measures to prevent
patient sliding. It warns that the risk of shear injury is greater in
Trendelenburg postion.
Shoulder braces have been associated with brachial plexus injuries.
AORN: VIII.j.2 recommends that we avoid the use of shoulder braces.
AORN: VIII.j.2 recommends the use of padded foot boards in reverse
trendelenburg position.
Trendelenburg Position: What if the Patient Slips?
pressure injuries
perineal nerve damage
shearing-tissue damage
robotic arm injuries
use anti-skid materials
brachial nerve damage
avoid stirrups
eliminate shoulder braces & straps
The use of anti-skid materials in the O.R will:
Reduce the incidence of shearing injury on soft tissues
Greatly reduce the risk of nerve injury , robotic injury and necrosis
Simplify the process of safely positioning patients
Promote positive patient outcomes
Trendelenburg Position
Trendelenburg position can require a tilt of up to 40 degrees.
This can result in a gradual slipping of the patient on the operating table. Shifts of up
to six inches have been reported
Potential risks associated with slipping
Nerve Injury
Injury to the brachial plexus due to pressure exerted on the clavicle by shoulder braces
has been the most cited nerve injury.
One in 15 people undergoing robot-assisted Genito Urinary Surgery developed a
nerve injury specifically related to positioning. Injuries included weakness, numbness
or immobility in the hands or feet.
Perineal nerve injury can occur when stirrups are used, which can lead to foot drop.
Robotic Injury
Robots are incapable of adjusting to any change in patient position. As a consequence,
instruments and trocars can be wrongly positioned causing internal injury. The
robotic arm may become the primary restraint for the patient - a situation sometimes
reffered to the ‘meathook restraint technique’ and which can result in post op pain,
bruising and / or necrosis at the primary port sites.
Tissue Necrosis
Shearing forces act parallel to the skin surface and are affected by the amount of force,
the angle of incline and the surface contact area.
The skin is pulled in an opposite direction to the bones and mus
cles of the sacrum, shoulders, arms and legs.
The deeper fascia slides downward with the bone; the superficial fascia remains
attached to the dermis. Blood supply may be compromised, causing ischemia and
subsequent tissue necrosis. Shear and friction go hand in hand—one rarely occurs
without the other.
Ms Niamh Devitt, RGN, PG Dip. Clinical Practice. Clinical Education Manager, TrulifeAllen, D. (2013) Positioning and the Surgical Robot. http://www.da-surgical.com/clinical-articles.html | AORN (2013) Perioperative Standards and Recommended Practices 2013 Edition | Hess, CT. (2004) Did You Know? The Difference between Friction & Shear 17(5)p222. Advances in Skin & Wound Care | Pittman, G (2013) Robotic surgery ties to temporary nerve injuries. http://www.reuters.com/article/2013/03/29/us-robotic-surgery-idUSBRE92S0D120130329 | Wetcher, ME. (2010) Trendelenburg Slide Prevention Study. Mayo Clinic ClinicalTrials.gov
external
friction
internal
shear
gravity
peripheral nerve
endings
dermis
epidermis
capillaries
table surface