Country level cost saving with hospital inventory system.
•Als PPT, PDF herunterladen•
0 gefällt mir•444 views

Poster for AcademyHealth about a country level cost saving with hospital inventory system.

Empfohlen
Weitere ähnliche Inhalte
Was ist angesagt?
Was ist angesagt? (20)
Ähnlich wie Country level cost saving with hospital inventory system.
Ähnlich wie Country level cost saving with hospital inventory system. (20)
Mehr von Mustafa Said YILDIZ
Mehr von Mustafa Said YILDIZ (20)
Kürzlich hochgeladen
Kürzlich hochgeladen (20)
Country level cost saving with hospital inventory system.
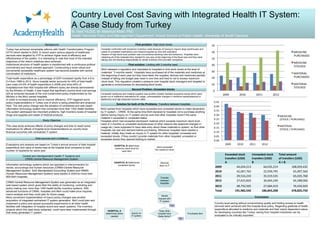
- 1. Country Level Cost Saving with Integrated Health IT System: A Case Study from Turkey M. Said YILDIZ, M. Mahmud Khan, PhD Health Services Policy and Management Department, Arnold School of Public Health, University of South Carolina Turkey has achieved remarkable reforms with Health Transformation Program (HTP) which started in 2003. In recent years various aspects of healthcare services were targeted by HTP to achieve higher level of efficiency and effectiveness of the system. It is interesting to note that most of the intended objectives of the reform initiatives were achieved. Institutional structure of health system is transformed with a continuous political commitment and result oriented approach. Constructing a more robust and conveniently accessible healthcare system has become possible with central coordination of institutions. Background This case study analyzes effects of policy changes and tries to reach some implications for effects of hospital level implementations on country-level financial outcomes with centralized IT system. Study Objective . First problem: High stock levels Hospitals confronted with excessive inventory costs because of having to require large warehouses and waste of unneeded medications and medical supplies by time with expiration. Reason of high stock level problem was conventional stocking rules and behaviors. Hospitals were obtaining all of the materials they needed for one year at the beginning of the fiscal year and they were taking over the stocking responsibility for whole inventory from provider companies. Central and interdependent Health IT Systems and CRMS-Central Resource Management System Data sources and Limitations Evaluations and analysis are based on Turkey’s annual amount of total hospital expenditure and value of stocks kept at the hospital level compared to total number of inpatients for same year Second Problem: Unneeded stocks Information technology systems which are operated in interconnection for stocks, accountings and human resources (CRMS-Central Resource Management System, SAS-Standardized Accounting System and HRMS- Human Resources Management System) were started in 2009 for more than 800 MoH hospitals. Unneeded medicines and medical supplies was another problem besides excessive stocks which were grown out of ineffective estimations for usage, unforeseeable changes in medicine needs(seasonal or epidemics) and high physician turnover rates. MoH released a regulation and mandated to hospitals to limit stock levels at the level of materials’ “3 months needs”. Hospitals have purchased all of the materials and medicines at the beginning of each year but they have taken the supplies, devices and medicines partially instead of taking one budget year need in one time and tried to not to excess maximum stock level. This regulation created a pressure over hospital stock managers and targeted to generate a consciousness for decreasing stock levels. First solution: Limiting with 3 months need Solution for both of the Problems: Transfers between hospitals MoH wanted from hospitals which have exceeded and unneeded stocks to make declaration by IT system – CRMS. At the same time MoH declared to hospitals not to purchase anything before having inquiry on IT system and be sure that other hospitals haven’t the same material in exceeded or unneeded status. Hospitals which had exceeded stock(each material which exceeds maximum stock level - need of 3 months) or unneeded stock(because of other reasons like seasonal changes in usage etc.) were supposed to have data entry about these materials to system, so that other hospitals can see and demand before purchasing. Whenever hospitals have needed a material, initially they made an inquiry in IT system for other hospitals’ unneeded and exceeded stocks. If they couldn’t provide materials from other hospitals’ unneeded or exceeded stocks they opened bidding to market. HOSPITAL B determines maximum stock level for each item HOSPITAL B Determines unneeded stocks Items exceeded the maximum level HOSPITAL A determines items needed Records them to IT system inquiry on IT system Does other hospital have these items? Sends request with IT system Transfer between hospitals Purchases item YesYes NoNo Exceeded stock transfers (USD) A Unneeded stock transfers (USD) B Total amount of transfers (USD) A + B 2009 44,024,213 64,035,219 108,059,432 2010 42,067,765 22,939,795 65,007,560 2011 29,516,233 35,519,535 65,035,768 2012 27,623,826 36,664,240 64,288,066 2013 48,750,505 27,684,419 76,434,924 Total 191,982,542 186,843,208 378,825,750 Country level saving without compromising quality and limiting access to health services were achieved with this hospital level policy. Regarding gratitude of health expenditure allocated to medicine and materials and their import dependent nature for developing countries like Turkey, saving from hospital inventories can be evaluated to be critically important. Conclusion Total health expenditure as a percentage of GDP increased rapidly from 4.8 to 5.4 from 1999 to 2012. Since hospital sector accounts for 40% of total health care costs (43.9% of health expenditure in 2008) and since 64% of hospitals(more than 800 hospital with different sizes) are directly administered by the Ministry of Health, it was hoped that significant country-level cost-savings will be achieved because of the cost containment policy implemented by the Ministry in the MoH owned hospitals. In order to increase access and to improve efficiency, HTP triggered some policy implementations in Turkey one of which is being presented and analyzed here. The new policy change was the adoption of centralized and web based information technology system that connected more than 1000 health facilities. The system addressed two important problems, high inventory levels of hospiital drugs and supplies and waste of medical products. CRMS-Central Resource Management System was generated as an integrated web based system which gives MoH the ability of monitoring, controlling and policy making over more than 1000 health facility inventory systems. With advanced functions of CRMS, hospitals and MoH could make price inquiries, macro analysis and they could plan for future usage. More convenient implementation of macro policy changes was another acquisition of integrated-centralized IT system generation. MoH could plan and implement a policy and spread successful experiments to all other health facilities with integration of hospital record and report systems. The inventory projects which this case study subjected, could have been implemented through that newly generated IT system.