
Empfohlen
Weitere ähnliche Inhalte
Ähnlich wie CIMS CASE 2 DIFF DX.pdf
Ähnlich wie CIMS CASE 2 DIFF DX.pdf (20)
Kürzlich hochgeladen
Kürzlich hochgeladen (20)
CIMS CASE 2 DIFF DX.pdf
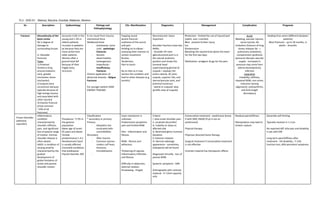
- 1. YL3 - SGD A1 Atienza, Baculna, Escobal, Malaluan, Moreno Dx Description Epidemiology Etiology and Pathophysiology Clin. Manifestation Diagnostics Management Complication Prognosis Fracture Discontinuity of the bone cortex W/ a degree of damage to surrounding tissues LI: Shoulder fractures Types 1) Proximal Humerus (ring around anatomic neck, greater trochanter, lesser trochanter) 2) Scapula (very uncommon because typically because of high energy trauma and associated with other injuries) 3) Clavicle Fracture (most common ~10% of all fractures) Accounts 4-6% in the young and 1-3% in elderly patients. Increase in pediatric px because they are more active than older patients. Women after a ground level fall because of their fragile bony structure. It can result from trauma, mechanical force Weakened bone - (metastasis, bone cyst) - pathologic fractures - Genetic abnormalities (osteogenesis imperfecta) - insufficiency fractures Chronic application of abnormal stresses - fatigue fractures For younger patient HIGH ENERGY TRAUMA Popping sound Severe fracture - erythema of the sound and pain Holding on to elbow - assessing their reaction to certain movement Bruises Tenderness Pain to touch No to hilot as it may worsen the condition and lead to other diseases (e.g bursitis) Neurovascular status important Shoulder fractions have two XRAYs: - shoulder AP view (glenohumeral joint is in the natural anatomic position and shows the humeral head superimposing glenoid of scapula + displays the entire clavicle, AC joint, scapula, superior ribs, and sternoclavicular joint, and proximal humerus) - lateral or scapular view (profile view of scapula) Protection - limited the use of injured part (splint, cast, crutches) Rest - prevent further injury Ice Compression Elevating the injured limb above the heart for the first two days Medication: analgesic drugs for the pain Acute Bleeding, vascular injuries, nerve injuries, fat embolism (fracture of long bones releases fat → pulmonary embolism), compartment syndrome (pressure disrupts vascular supply - increased in pressure may come from edema development), infection Long term Instability, stiffness, impaired ROM, non-union, malunion (wrong alignment), osteoarthritis, and limb length discrepancy Healing time varies (different between patients) Most fractures - up to 18 months, in adults - 3months Frozen Shoulder (adhesive capsulitis) Inflammatory condition characterized by shoulder stiffness, pain, and significant loss of passive range of motion. Intrinsic shoulder disease is often absent. AAOS: a condition of varying severity characterized by the gradual development of global limitation of active and passive shoulder motion Prevalence ~2-5% in the general population Mean age of onset: 65 years and above Female predominance 1.4:1 Nondominant hand is usually affected Comorbid conditions that predispose: thyroid disorder, DM Classification * secondary or primary Primary - Idiopathic but associated with comorbidities SEcondary - After trauma - Common injuries - rotator cuff tears, fractures, immobilization - Exact mechanism is unknown Predominant symptoms: pain and limited ROM Pain - inflammation and fibrosis ROM - fibrosis and adhesions Thickening of capsule, inflammatory infiltrates and fibrosis Difficulty in abduction, external rotation Kinalawang - hinged Criteria I. slow onset shoulder pain Ii. Localized discomfort Iii. Inability to sleep on affected side Iv. Restricted gleno-humeral elevation V. Extensor rotation Vi. Normal radiologic appearance - sometimes, osteopenia will be found Diagnosed clinically - loss of passive ROM Systemic symptoms - MRI Arthrography with contrast material - if <15ml capacity only Conservative treatment - prednisone (know if with DM); NSAID (if pt is not on prednisone) Physical therapy Physician directed home therapy Surgical treatment if conservative treatment is not effective Contrast material has therapeutic effects Residual pain/stiffness Manipulation may lead to tendon rupture Generally self-limiting Typically resolves in 1-3 yrs No reported diff. b/w pain and disability in pts with DM Long-term pain/stiffness after treatment - 5% disability ; 7-15% function loss; 40% persistent symptoms
- 2. Shoulder Bursitis Bursae - sacs surrounding the synovial fluid 0.4% of all primary care visits Gender prevalence is equal in M & F Older in individuals it is because of years of wears Most common form is the subacromial bursitis often accompanies rotator cuff tendinitis Caused by ● repetitive overhead activities (Athletes, factory workers, manual laborers) ● Minor trauma or fall ● Long periods of wear and tear ● Crystal deposition ● Subacromial hemorrhage ● Autoimmune disease ● Infection ● Impingement syndrome Can be multifactorial also ● Pain in the anterolateral ● Usually does not radiate but if present, would often point to underlying pathology ● Point tenderness ● Skin is warm but no erythema (rare) ● History and PE Lab tests are usually unremarkable Imaging - not really necessary Xray - to R/O other causes of pain Utz, MRI - excellent imaging; associated tendon lesions; eval thickness of bursa Ave shoulder: Thickness of bursa ~0.25mm W/ bursitis: ~1.27mm Usually nonoperative ● Rest ● NSAIDs ● Physical therapy ● Corticosteroid injection If conservative treatment is uneffective or with recurrence ● Bursectomy or compression ● May also address problems with rotator cuff Rotator cuff damage Self-limiting condition No long-term impact Most improve with therapy Worsens as pt gets older Rotator Cuff Injury Suraspinatus is most commonly affected Infra- not involved Associated with Impingement syndrome Common cause of pain in all age group 10% - children 30% - adults 62% - >80yo RF Age is most common factor Smoking Fam history Poor posture - 50% more likely Trauma Hypercholestorelimea Occupational activities that req significant overhead activity Partial tears factors Size - small may remain dormant Symptoms - actively enlarging tears Location - anterior are more likely to progress Age - >60 develop tears that progress Macrotrauma - tear Elderly - microtrauma - degenerative tear ● Pain (acute; from trauma) ● Difficulty w/ overhead activities ● Pain can radiate to deltoid muscle ● Tenderness on insertion of 3 SITS muscle ● Limited ROM associated w/ pain Xray - narrowing Utz - eval of dynamic movement MRI - gold standard; can show tear size, location, atrophy, tendon and muscle changes History and PE Depends on age , functional demands ● <40yo w/ complete tears - surgery w/ rehab ● Most traumatic injuries respond well ● Weak evidence against surgical therapy ● Physical therapy also works 5 categories ● Repair______ ● Healthy pt, asymptomatic - repair ● Rotator cuff injury, symptomatic - surgcal treatment ● Chronic massive tears -debridement and reconstruction ● Painful pseudoparalysis w/ irreparable tear - arthroplasty Asymptomatic tear - nonoperative management Newly diagnosed tears - PT for muscle strengthening No clear advantage b/w surgical and non surgical treatment Algorithm __________ Adhesive capsulitis Weaker cuff strength Infectious arthritis Mostly bacterial; may also be fungal, viral, etc 2-6 / 100,000 children> adults Peaks b/w 2-3yo M>f; 2:1 Mc. staph aureus Streptococcus pneumoniae Sexually abused - Neisseria gonorheae ______ Systemic:Ill appearance, fever, tachycardia, Evaluation: synovial fluid analysis: culture, gram stain, crystal analysis, WBC count Can be caused by a plethora of causative mcgs ● Antimicrobial therapy Morbidity - ⅓ of pt - Increase w/ age - Joint disease
- 3. Orthopedic emergency Can cause significant joint damage and cause death RF for children ● Hemophilia cs ● Immunoco mpromised (sickle cell, HIV) ● Treated w/ chemo RF for adults ● Starts at 80yo ● Comorbiditi es (DM, recent surgery, arthritis, ulceration) ● HIV ● Sexual activity ( gonococcal infection) Trauma Abdominal infection Might be due to punctured wounds, intraarticular injections, contiguous spread, hematologic problem (osteomyelitis) Occur w/ bacterial invasion of synovium - inflammatory process irritability, decreased appetite Most staph infections - monoarticular Neisseria - multiple joints (polyarticular) Group B Strep: sternoclavicular, sacroiliac joints Joints affected with prosthetics - drain sinus (>50,000) with diff (increased neutrophil) Laboratory CBC, ESR, CRP, blood cultures Imaging Plain radiograph: widened joint spaces, bulging of some tissues or subchondral bony changes (normal radiograph does not r/o IA) MRI: sensitive for the early detection of joint fluid and delineates the extant of cartilaginous involvement Bone scan: not specific but useful in evaluating sacroiliac, and hip joint - Empiric - done after aspiration; anti-staph, anti-neisseria - vancomycin; immunocompromized, 3rd gen ceph; - Gram stain ● Joint fluid drainage - If affected area is hip, shoulder or prosthetic joint, inadequate aspiration of fluid, no improvement ○ Daily needle aspiration Complications: - Osteomyelitis - Chronic pain - Osteonecrosis - Discrepancy in leg length - Sepsis (leads to death) Osteosarcoma Spindle cell neoplasm that produces osteoid. Deadly form of msk cancer. The common cause of death of px is pulmonary metastatic disease. Most arise as solitary lesions with the top 3 affected areas: distal femur, proximal tibia, and humerus. Although it could affect any bone. Multifocal is rare and occurs in px younger than 10 years. Classification 75% - classic (composed of obsteoblastic, chondroblastic, fibroblastic) 25% - variant (based on the clinical, morphological Considered as the most common malignant bone tumor 40% are osteosarcoma 60% are in children/adolescents until 19 years old 10% are in the third decade of life In those in the 5th decade are due to radiation therapy Bimodal age distribution (diagnosed at 2nd-3rd decade and second peak at >65) Males > females (1.5-2x) Black > white Usually occurs in the metaphysis of the long bone distal femur, proximal tibia, and proximal humerus Unknown exact etiology and pathophysiology Risk Factors 1. Rapid bone growth 2. Genetic predisposition (RB gene is the commonly mutated + radiation therapy = increase in risk) Li Fraumeni Syndrome (p53), Roth 3. Environmental Risk Factor - radiation induced (secondary cancer in mostly elderly) - May present for weeks and months before px is diagnosed - Most pressing symptom: pain w/ activity - Often w history of trauma (unclear contribution) - Swelling is dependent on size and location - Systemic symptoms are rare - Findings are limited in the site of primary tumor (palpable mass may or may not be present - increased skin vascularity, pulsation or bruit may be found) - Decreased ROM Laboratory Studies - Relate to the use of chemotherapy (monitoring of organ fxn) - ALP and LPH are the most impt test - CBC - Liver Function (ALT, AST) - Electrolyte level (sodium - Renal Function Tests Imaging Studies Plain radiography (Xray) - Elevation of periosteum (new bone formation) CODMAN TRIANGLE - Sunburst appearance Bone Scanning - 99 MPC/MDP/MPI - Multifocal disease (metastasis) - Not always used CT Scan Chemotherapy ● Diet is not restricted Excision ● Wide-resection; margins on all side must contain normal tissue Limb-sparing surgery ● Resection ● Reconstruction ○ Not required for Non-weight bearing bones ○ 2 types: endoprosthetic replacement and biological reconstruction Biological reconstruction - Allograph, autograph,... - Depends on staging and using of appropriate management for diff. stages
- 4. characteristics, and location - Involvement is obvious on PE - Lymph node involvement is uncommon - Obtained before biopsy (less ambiguity that arise after post-anaesthesia atelectasis) - Metastasis MRI - Best method of assessing intramedullary disease, soft tissues masses, skip lesions - MOST ACCURATE for surgical system - Enneking Staging System Histologic grade Anatomic location presence/absence of metastasis IA: low, intra IB: low, extra IIA: high, intra IIB: high, extra III: w/ metastases Intracompartmental: any individual bone, intra articular space