
Empfohlen
Weitere ähnliche Inhalte
Was ist angesagt?
Was ist angesagt? (20)
Ähnlich wie Rbc indices
Ähnlich wie Rbc indices (20)
Mehr von Manan Shah
Mehr von Manan Shah (15)
Kürzlich hochgeladen
Kürzlich hochgeladen (20)
Rbc indices
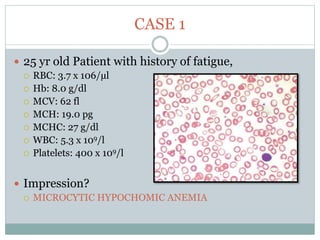
- 1. CASE 1 25 yr old Patient with history of fatigue, RBC: 3.7 x 106/µl Hb: 8.0 g/dl MCV: 62 fl MCH: 19.0 pg MCHC: 27 g/dl WBC: 5.3 x 109/l Platelets: 400 x 109/l Impression? MICROCYTIC HYPOCHOMIC ANEMIA
- 2. CASE 2 30 yr old, Male patient with fatigue RBC: 4.5 x 106/µl Hb: 11.0 g/dl MCV: 115 fl MCH: 25.0 pg MCHC: 30 g/dl WBC: 7 x 109/L Platelets: 350 x 109/L Impression? MACROCYTIC ANEMIA
- 3. CASE 3 23 yr old, Male patient RBC: 4.5 x 106/µl Hb: 11.0 g/dl MCV: 87 fl MCH: 30.0 pg MCHC: 33 g/dl WBC: 6.5 x 109/L Platelets: 350 x 109/L Impression? NORMOCYTIC NORMOCHROMIC ANEMIA
- 4. DR. MANAN SHAH P O S T G R A D U A T E M D P A T H O L O G Y DIAGNOSTIC UTILITY OF RBC INDICES
- 5. OBJECTIVES To define & calculate the RBC Indices To describe the application of RBC indices in diagnosing various disorders. To interpret RBC Histograms.
- 6. RBC INDEX It is a quantitative measurement of red blood cell, the amount and concentration of hemoglobin in them. They were first introduced by Wintrobe in 1929 to define the size (MCV) and hemoglobin content (MCH & MCHC) of red blood cells
- 7. DEFINITIONS: Mean cell volume (MCV) It is the measure of average volume of RBCs Mean cell Hemoglobin (MCH) It is a measurement of the average weight of hemoglobin in individual erythrocytes. Mean Cell Hemoglobin Concentration (MCHC) It is the average concentration of hemoglobin in erythrocytes Red cell distribution width (RDW) It is a measure of variability of erythrocyte size
- 8. WHY RBC INDICES REQUIRED? To classify the erythrocytes by their volume and Hemoglobin content This indices suggest how the RBC’s appear microscopically and provide significant information (most commonly for Anemia diagnosis) Laboratory professionals correlate the indices with Hct, Hb and RBC count to ensure that technical problems are identified when they occur
- 9. MEAN CELL VOLUME MCV = Hct(L/L) x 1000 RBC count ( x 1012/L) Normocytic: 80-100 fL Microcytic: Red cells with reduced volume(<80fL) Macrocytic: Red cells with an increased volume(>100 fL) Remember MCV is a measurement of volume whereas estimation of size of flattened cells is a measurement of cell diameter. Cell diameter and cell volume are not same
- 10. MCV Increased MCV Decreased Causes? Causes? Fig. 2 Fig. 1
- 11. MEAN CELL HEMOGLOBIN CONCENTRATION It is the average concentration of hemoglobin in a deciliter of erythrocytes and expressed in g/dl It is the ratio of hemoglobin mass to volume in which it is contained MCHC = Hb (g/dl) x 100 Hct (L/L) Normochromic: 32-36g/dl Hypochromic: <32g/dl Hyperchromic: >36g/dl
- 12. MEAN CELL HEMOGLOBIN CONCENTRATION Hypochromic: If the area of central pallor is >1/3rd of the cell size Hyperchromic: The only erythrocyte that is hyperchromic with an MCHC of > 36g/dl is the spherocyte Apparent hyperchromasia ( high MCHC) is usually due to an artifactual increase in the haemoglobin result, due to haemolysis, lipaemia, or large numbers of Heinz bodies
- 13. MCHC Decrease Causes? MCHC Increase..?? Causes? Fig. 3 Fig. 4
- 14. MEAN CELL HEMOGLOBIN It is a measurement of the average weight (in picograms 10 -12 g)of hemoglobin in individual erythrocytes. It is calculated by: MCH = Hb (g/dl) x 10 RBC( x 10 12/L) MCH varies in direct linear relationship with the MCV. Cells with less volume contain less Hb and vice versa Normal value for the MCH : 28 to 34 pg
- 15. MCH Increase MCH Decrease B12 deficiency Folic acid deficiency Reticulocyte Hemolytic anemia alcoholism Iron deficiency anemia Thalassemia Anemia of chronic disorder MEAN CELL HEMOGLOBIN
- 16. • Comment on size of RBC..? Anisocytosis Fig. 5
- 17. CASE 4 25 yr old Patient with history of fatigue RBC: 3.0 x 106 /µl Hb: 8.0 g/dl MCV: 62 fl MCH: 19.0 pg MCHC: 30 g/dl WBC: 5.3 x 109/l Platelets: 400 x 109/l Impression: MICROCYTIC HYPOCHOMIC ANEMIA Differential diagnosis?
- 18. CASE 4 25 yr old Patient with history of fatigue RBC: 3.0 x 106 /µl Hb: 8.0 g/dl MCV: 62 fl MCH: 19.0 pg MCHC: 30 g/dl WBC: 5.3 x 109/l Platelets: 400 x 109/l RDW: 18% Impression: MICROCYTIC HYPOCHOMIC ANEMIA Importance of RDW here?
- 19. RED CELL DISTRIBUTION WIDTH RDW is used because MCV is less reliable in describing the erythrocyte population when considerable variation in erythrocyte size occurs. RDW is a coefficient of variation in size distribution of RBCs Measured as : RDW = Standard deviation of MCV × 100 MCV Normal value:11.5-14.5% Increased value indicates ANISOCYTOSIS.
- 20. RDW and MCV
- 21. RDW RDW is increased in Iron deficiency anemia. While RDW is normal in Thalassaemia minor. Combination of low MCV and high RDW is one of the best screening test for the Iron deficiency anemia. Mentzer index..? Sideroblastic anemia..? Further evaluation..?
- 22. FURTHER EVALUATION For IDA S. ferritin level (low) TIBC (Increased) Transferrin saturation (Decreased) PBS: pencil cells, anisocytosis RBC count: Decrease For Thalassaemia PBS: target cells, polychromatic cells, basophilic stipling Rbc count: Normal / Raised. HbA2: Raised(>3.5) For Sideroblastic anemia S. iron increased S. ferritin level increased Dimorphic anemia and pappenheimer bodies seen
- 28. Echinocytes/ Burr cells Causes..? Acanthocytes/ spur cells Causes..? Fig. 8 Fig. 9
- 29. Stomatocytes/ mouth cells or cup cells Causes..? Drapanocytes/ sickle cell Causes..? Fig. 10 Fig. 11
- 32. CASE 5 26 yr, Patient of low socio economic status comes with history of weakness since 6 months, history of chronic abuse of PPI. RBC: 3.0 x 106 /µl Hb: 11.0 g/dl MCV: 75 fl MCH: 24.0 pg MCHC: 29 g/dl WBC: 5.3 x 109/l Platelets: 400 x 109/l RDW: 17% Interpretation? Microcytic hypochromic anemia Is Vit B12 def possible in this patient? A case of dimorphic anemia or combine anemia. If yes - explain MCV?
- 35. CAUSES? Folate/ Vit B12 and Iron deficiency Malnutrition Malabsorption Pregnancy Alcoholism Atrophic gastritis (Vit B12) Thalassaemia and Vit B12 / Folate deficiency Iron deficiency with hemolysis. (prosthetic valve) Peripheral blood smear examination is very critical.
- 36. CASE 6 32 yr old patient with GI Bleed/hemorrhoid, no history of drugs or hematological disorder RBC: 3.0 x 106 /µl Hb: 11.0 g/dl MCV: 102 fl MCH: 26.0 pg MCHC: 32 g/dl WBC: 5.3 x 109/l Platelets: 400 x 109/l RDW: 12% Impression? Macrocytic Normochromic anemia
- 37. RETCULOCYTES Premature RBC They contain remnants of Ribosomal RNA Number of reticulocytes in PBS is a fairly accurate reflaction of erythropoietic activity It is most useful and cost effective test in monitoring and response to iron therapy
- 38. RETCULOCYTES COUNT It can be done by two methods, Manual method Automated method Manual method. Romanowsky stain can not stain reticulocytes effectively. Suspect reticulocyte when Polychromatophilic cells on PBS with Romanowsky stain seen (erythocyte with bluish tinge) A supravital stain such as NEW METHYLENE BLUE, BRILLIANT CRESYL BLUE must be used to identify reticulocytes.
- 39. RETCULOCYTES COUNT Automated methods By Fluorescent flow cytometry Or by scattered light with methylene blue staining In automated method >30,000 RBCs are assessed So the method is more precise and has high degree of accuracy than the manual method. (where only 1000 RBCs are assessed) It is also more accurate when reticulocyte count is low
- 40. RETCULOCYTES COUNT Corrected reticulocyte count Used to adjust the reticulocyte count in proportion to the severity of anemia Corrected retic count= patient hematocrit Normal hematocrit x % reticulocyte Its practical importance is to assess the degree of erythropoiesis in anemic patient. In anemic patient <2% of corrected retic count associated with hypo cellular bone marrow
- 41. Reticulocyte production index This index is used to correct the time of prolongation of maturation of reticulocyte due to sever anemia Calculated by = patient hematocrit x retic count (%) normal hematocrit x retic maturation time(days) Also known as SHIFT CORRECTION INDEX PCV% MATURATION DAY(S) 45% 1 35% 1.5 25% 2 15% 2.5
- 43. Fig. 14 Fig. 15 Heinz bodies Howell-jolly bodies
- 44. RETICULOCYTES A higher reticulocytes count may indicate: Anemia due to RBC being destroyed earlier than normal (hemolytic anemia) Bleeding (GI Bleeding) Blood disorder in a fetus or newborn (erythroblastosis fetalis) Kidney disease, with increased production of erythropoietin Reticulocyte count may be higher during pregnancy. A lower reticulocytes count may indicate: Bone marrow failure (eg. drug, tumor, radiation Rx or infection) Cirrhosis of the liver Untreated patient of pernicious / megaloblastic anemia Chronic kidney disease
- 45. STRESS RETICULOCYTE OR STRESS ERYTHROPOIESIS In sever anemia when human body is in need of reticulocyte or when there is a overproduction of RBC, these is increase in reticulocyte in blood. This is called as Shift reticulocyte or stress reticulocyte. This is similar to shift to left in WBC.
- 47. CASE 7 65 yr, Male, chronic cigarette smoker. H/o chronic cough and confusion since few weeks. Complete blood count of the patient done… RBC: 7.0 x 106/µl Hb: 20 g/dl MCV: 70.o fl Hct: 60% WBC: 16 x 109/l Platelets: 625 x 109/l Reticulocyte: 3.5% Differential diagnosis..?
- 48. CASE 7 Detail history… Presented with no change in voice No h/o haemoptysis, weight loss. No change in pattern of cough, and not affecting his sleep. Enlarged spleen, slightly purple-red discoloration of facial skin Chest X-ray: hyperinflation, no evidence of lung cancer Differential Diagnosis..? Diagnosis: Polycythemia vera
- 49. RBC COUNT It is total number of RBC per µL or a liter of blood. The test can help to diagnose anemia with low number of RBCs and other conditions affecting red blood cells. Conditions require RBC count are, Kidney diseases Anemia Bonemarrow disorder like mylofibrosis
- 50. RBC COUNT Mature RBC is a biconcave disc about 7-8 µ in diameter. Normal volume is 80-100 fl, normal hemoglobin content is 28-34 pg/dl. Normal RBC count Male: 4.3 – 5.9 (x 1012/l or 106/µl) Female: 3.5 – 5.0 (x1012/l or 106/µl)
- 51. RBC COUNT Higher numbers of RBCs may be due to: Cigarette smoking Failure of the right side of the heart (cor pulmonale) Dehydration (for example, from severe diarrhea) Kidney tumor (renal cell carcinoma) Low blood oxygen level (hypoxia) Bone marrow disease that causes abnormal increase in RBCs (polycythemia vera) Drugs like gentamycin / methyldopa
- 52. RBC COUNT Low number of RBC may be due to: Anemia Bleeding Bone marrow failure (for example, from radiation, toxins, or tumor) Deficiency of a hormone called erythropoietin (due to kidney disease) RBC destruction (hemolysis) due to transfusion, blood vessel injury, or other cause Malnutrition Multiple myeloma Deficiency of iron, copper, folic acid, vit B6, or vit B12 in the diet Over hydration Pregnancy
- 53. POLYCYTHEMIA Polycythemia is a general term used to describe erythrocytosis resulting in an increase in both hemoglobin concentration and hematocrit ie increase in number of RBC It can be due to, Relative polycythemia Due to decrease plasma volume There is normal or even decrease red cell mass It is generally mild polycythemia Due to dehydration, hemoconcentration Secondary polycythemia Physiologic stimulus is present hense the name secondary Elevated plasma EPO levels (unlike polycythemia vera) Polycythemia vera
- 54. POLYCYTHEMIA VERA Increased in Red Cell Mass Acquired myloproliferative disorder Over production of all 3 cell line, mostly RBC Increased HB > 18.5 g/dl in Male > 16.5 g/dl in Female Increased Hematocrit > 52% in Male >48% in Female Also known as 1° polycythemia, Polycythemia rubra vera and Osler Syndrome. Result from the mutation in JAk2, a signaling molecule in 95% of cases.
- 55. FURTHER EVALUATION OF PV EPO level are normal or low in PV On PBS RBC overcrowding and with feathered edge seen Leukocyte aggregate in PBS of PV patient. Increased WBC count and platelet number BONE MARROW BIOPSY Shows red cell hyperplasia
- 57. CASE 8 A 20 yr old male, with history of weakness since few month RBC: 1.0 x 106/µl Hb: 6 g/dl MCV: 110.o fl Reticulocyte count: <1% WBC: 0.4x 109/l Platelets: 10 x 109/l Impression..? PANCYTOPENIA Causes of Pancytopenia?
- 58. APLASTIC ANEMIA It is condition of pancytopenia with hypocellular bonemarrow Diagnostic criteria: Bone marrow cellularity: <25% (hypocellularity) Plus two of following Granulocyte count: <0.5x109/L Platelet count: <20x 109/L Anemia with corrected reic count: <1%
- 59. HEMATOCRIT Hematocrit measures the volume that the RBC occupy within whole blood. It is expressed in percentage or L/L. In automated analyzer, the hematocrit is usually calculated by the measured MCV and RBC count by using formula Hematocrit = MCV (fl) x RBC count (x1012/l) 1000
- 60. HEMATOCRIT Elevated hematocrit Dengue fever (sign of an increased risk of DSS) Polycythemia vera COPD Hemolytic anemias False high hematocrit Dehydration Burns patient Sever vomiting If Sample is not mixed properly Low hematocrit Iron deficiency anemia Leukemia False low hematocrit Hemodilution Volume overload pregnancy
- 61. HEMATOCRIT One should interprets accuracy of RBC count, hematocrit and hemoglobin value using quick formula called the “RULE OF THREE”. RBC Count x 3 = hemoglobin x 3 = hematocrit(%) If error > 3% of the measured value, a measurement error or instrument malfunction suspected. DIURNAL VARIATION RBC Count, hematocrit and hemoglobin concentration shows diurnal variation These values are higher in the morning
- 63. MICRO HEMATOCRIT Definition: A procedure for determining the ratio of the volume of packed red blood cells to the volume of whole blood by centrifuging a minute quantity of blood in a capillary tube coated with heparin. (RED color marked capillary tube). Uses: Sample is very less Pediatric age group
- 64. LIMITATIONS OF RBC INDICES Though the test for RBC INDICES is cost effective and simple, it has its own limitations. Such as, It is a screening test not a diagnostic test MCV is not reliable when Anisocytosis is present In combine or dimorphic anemia again MCV is not reliable MCV does not reflect the diameter of the RBC, It is a volume of RBC False high or false low value, which should be evaluated further Automated Reticulocyte count is not standardized yet. And manual method has inter-observer bias.
- 65. RBC HISTOGRAM PRICE – JONES CURVES
- 66. X axis: RBC volume Y axis: RBC Number
- 67. Salient Features RBC Histogram is a bell shaped curve The instrument counts cell as erythrocyte with volume sizes between 25 fl to 250 fl Area of the peak is used to calculate the MCV and the RDW. This area represents 60-125 fl. Shift to right- RBC are larger (Macrocytes) Shift to left- RBC are smaller (Microcytes)
- 77. SUMMERY RBC index (MCV, MCH, MCHC) and RBC count helps in diagnosis of anemia Combination of various RBC indices (MCV, MCH, MCHC) especially with RDW is useful in differential diagnosis of anemia Reticulocyte count is a important indicator of bone marrow activity and it can also be useful in monitoring and response to iron therapy
- 78. REFERENCES McKenzie SB, Williams JL. Clinical laboratory hematology. 3rd edition. New jersey: Pearson education inc; 2015 Bain BJ, Bates I, Laffan MA, Lewis SM. Practical hematology. 11th edition. Netherlands: Elsevier; 2012 Lokwani DP. Interpretation of complete blood count and histograms McCann S, Foa R, Smith O, Conneally E. Clinical cases uncovered: Hematology. New jersey: Wiley- Blackwell; 2009